Practical Clinical Pathology Liver Disease Wendy Blount DVM

Practical Clinical Pathology Liver Disease Wendy Blount, DVM Nacogdoches, TX

Primary vs Secondary Liver Disease • • One of the most difficult tasks of dealing with liver disease is to distinguish one from another Primary Liver disease must be treated at it’s cause, if we are to do anything but palliate Secondary Liver Disease just distracts us from the primary problem, whether liver disease, and/or something else Secondary Liver Disease = Reactive Hepatopathy

Primary vs Secondary Liver Disease Is the liver sick? ? ? Or is the liver just doing it’s job? ? Or is it an innocent bystander suffering from collateral damage? 1. Determine if you have liver disease 2. Determine if it is primary or secondary 3. Whether primary and/or secondary, determine the cause and hope to treat it 4. Support the liver as needed, to minimize collateral damage

Lisa Drapela – Lufkin TX

Primary vs Secondary Liver Disease Signs of Primary Liver Disease – The Liver Is Sick! • Change in liver size or shape – – – Hepatomegaly Microhepatia Liver mass Irregular liver margins Radiographs the best test for liver size Ultrasound the best test for liver shape and to find masses

Primary vs Secondary Liver Disease Signs of Primary Liver Disease – The Liver Is Sick! • Change in liver size or shape – – – Hepatomegaly Microhepatia Liver mass Irregular liver margins Radiographs the best test for liver size Ultrasound the best test for liver shape and to find masses

Primary vs Secondary Liver Disease Signs of Primary Liver Disease – The Liver Is Sick! • Change in liver size or shape – – – • • • Hepatomegaly Microhepatia Liver mass Irregular liver margins Radiographs the best test for liver size Ultrasound the best test for liver shape and to find masses Icterus without anemia Hepatic encephalopathy Prolonged recovery from anesthesia

Primary vs Secondary Liver Disease Signs of Primary Liver Disease • Acholic feces • Third space effusions – – – • Portal hypertension – transudate or modified transudate in the abdomen and not in the pleural space Increased sodium retention and plasma volume expansion Hypoabuminemia (loss of venous oncotic pressure) Tendency to sepsis – – Hepatic RE system detoxifies blood from gut via portal circulation FUO can be the only overt symptom

Primary vs Secondary Liver Disease Signs of Primary Liver Disease • Coagulopathy – The Liver Is Very Sick!! – GI hemorrhage death spiral 1. Increased stomach acidity – – Decreased hepatic clearance of gastrin Increased bile acids further stimulate HCl secretion 2. Clotting factor’s, AT 3 not produced adequately – Poor clotting and thromboembolic disease 3. DIC – more AT 3 consumption – more thromboembolic disease • Positive Feedback Loop #1 - GI Bleeding exacerbates hepatic encephalopathy • Positive Feedback Loop #2 - Large bleed can cause depletion coagulopathy – Hemorrhage elsewhere only when near death • Petechiae, bruising, bleeding into cavities

Primary vs Secondary Liver Disease Signs of Secondary Liver Disease • Icterus without anemia – – • Specific for hepatobiliary disease, but can be primary or secondary Chicken or Egg? ? Sepsis can cause secondary liver disease or be a result of primary liver disease Symptoms and Syndromes with many other causes – – – • Third Space effusions PU-PD coagulopathies Non-specific signs – many other causes – – anorexia, weight loss, lethargy, vomiting, diarrhea Fever

Problems Causing Reactive Hepatopathy • Any Systemic infection or inflammation – • Disease of organ drained by portal vein – • • • Gut, spleen, pancreas (ultrasound the best test) Hyperthyroidism in cats Severe muscle disease Hypoxia, passive congestion – – • Occult - urinary tract, metritis, prostatitis, dental disease, etc. heart failure, respiratory disease, severe anemia hypotension Drugs causing liver enzyme induction

Diagnostics for Liver Disease First Tier Tests: • CBC, panel, urinalysis • Fecal flotation, direct smear, cytology • HWAg in the dog, Fe. LV/FIV in the cat Second Tier Tests: • Bile Acids • Complete Abdominal Ultrasound (not focused liver/GB and not Global. FAST®) • Liver sampling • • • FNA Ultrasound guided biopsy – 50% diagnostic Wedge biopsy – more likely to be diagnostic

Diagnostics for Liver Disease Third Tier Tests: • if Bile Acids are equivocal and PSS is suspected – – • Ammonia tolerance test Splenic portagram Coagulation tests if significantly systemically ill, severe liver disease is suspected, or liver sampling will be done • • • FNA – normal BMBT and platelet count are sufficient Ultrasound guided biopsy or Wedge biopsy – platelet count, PTT, BMBT If coags abnormal, have whole blood on hand Always do liver sampling in the morning, and preferably not on a Friday Hunt for causes of secondary liver disease • Imagine - radiographs and ultrasound

Pattern Recognition - Liver Disease • High liver enzymes – – • Low albumin – – • • ALT – hepatocellular disease (hepatocellular membrane) ALKP, GGT – more sensitive indicator of cholestasis than bilirubin (from biliary epithelium) low alb indicates severe disease (90% loss of hepatic function) Beware human labs (falsely low values) - Abaxxis Low fasting glucose (70% loss of hepatic function) High prost-prandial glucose Low BUN Abnormal cholesterol, triglycerides

ALT Gems The enzyme formerly known as SGPT • RBC & skeletal muscle contain small amts of ALT – • Hemolysis and muscle damage cause moderate elevations in ALT (2 -3 x) ALT - t 1/2 – 1 -2 days – the first to improve – – • Starts improving within 1 -2 weeks of liver disease resolution remains elevated during hepatic regeneration DDx hepatocellular turnover – – Hepatocellular disease Poor perfusion – hypotension, passive congestion, anemia • – – Marker for anaphylaxis, along with increased PTT and FAST sonogram Trauma – surgery, trauma, peritonitis Toxicity

ALKP Gems • Bone disease can also cause ALKP elevation – • Neoplasia, osteomyelitis, hyper. PTH, growth & healing DDx cholestasis: – Gallbladder disease • • – Intramural - Gallbladder sludge, mucocoele, stones, infection Mural - Gallbladder wall polyps, masses, infection Extramural – Pancreatitis, abdominal mass, duodenal foreign body Gallbladder trauma or rupture Liver Disease – microscopic cholestatic disease (infectious, inflammatory, toxic), liver trauma, neoplasia, lipidosis

ALKP Gems • DDx cholestasis: – Systemic cholestatic disease • • Endocrine – diabetes mellitus, hyperadrenocorticism, chronic stress, hyperthyroidism Passive congestion – RHF, pericardial disease Diaphragmatic hernia Systemic infection/inflammation – especially sepsis, rickettsial disease

GGT Gems • less influenced by secondary liver disease or acute hepatic necrosis than ALKP Not confounded by bone disease as ALKP more useful in cats than in dogs • • – – • increases suspicion of fatty liver when ALKP high and GGT not so high Do ultrasound and liver FNA cytology Otherwise, follows ALKP
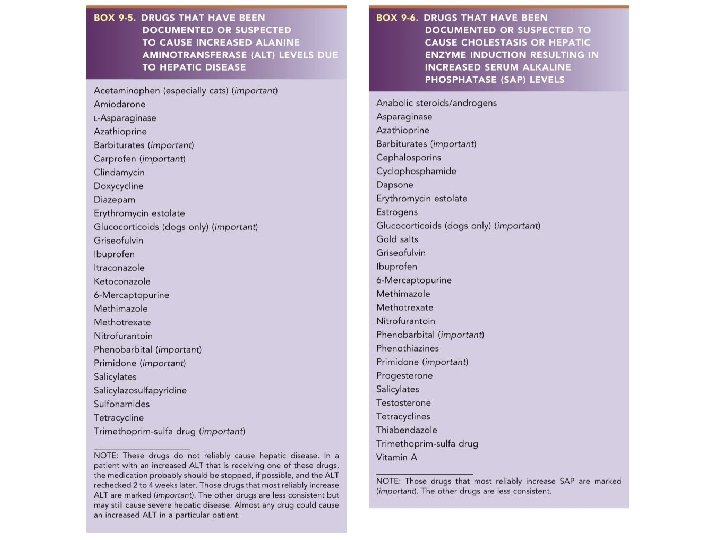

Hepatotoxic Drugs • Drug induced ALKP does not necessarily indicate hepatic pathology – – • • • Assess with bile acids if concerned Phenobarbital can also cause hepatotoxicity, but glucocorticoids almost never do GGT increases markedly with corticosteroid enzyme induction in dogs Drug induced ALKP takes weeks to months to resolve after stopping the drug Glucocorticoids almost always elevate ALKP (and ALT) in dogs, but almost never in cats

Hepatotoxic Drugs • • Drugs that increase ALT are more likely to cause hepatic damage if continued At a marked increase in ALT, the offending drug should ideally be stopped, and ALT rechecked in 30 days Lomustine - missing from the chart, but can cause potentially life threatening hepatotoxicity indicated first by increased ALT and then decreased albumin. Use of any drug on either chart indicates monitoring of liver nz + bile acids, albumin

Elevated Liver Enzymes in the Cats are not little dogs – Thumb Rules • Cats with persistently elevated enzymes should be worked up – – • • T 1/2 of liver enzymes is hours in the cat, not days as in the dog cats have 1/3 the liver ALKP compared to dogs Cats with significant cholangiohepatitis can have normal liver enzymes, though that problem often causes very high ALT GGT in cats has higher sensitivity but lower specificity for biliary disease • If a cat has biliary disease, GGT is likely high • If cat does not have biliary disease, GGT can still sometimes be high

Elevated Liver Enzymes in the Cats are not little dogs • ALKP elevation significantly exceeds GGT elevation only in hepatic lipidosis High bile acids in the cat indicate liver disease nearly 100% of the time Most common causes of ALKP elevation in the cat • • – – Cholangiohepatitis, cholangitis Hyperthyroidism Fatty liver, diabetes mellitus (not hyperadrenocorticism alone) (Lymphoma, Pancreatitis)

Jes Odes Adkins – Fairfield TX

Elevated Liver Enzymes in Well Dogs Grrrr… Reactive Hepatopathy or Liver Disease? 1. 2. Expect ALKP to be high in growing dogs (2 x) Explore the history & exam for untreated problems that might cause reactive hepatopathy treat Treat empirically for common things first Treat subclinical cholangiohepatitis 3. • – • Amoxicillin 10 mg/lb PO BID x 3 weeks Supplement to curtail hepatic inflammation – Denosyl®, Denamarin® – dosage chart in package • – – – Now available in chewables (Denosyl®, Denamarin®) Be careful of SAMe supplements not in foil packages Milk thistle (Marin®) Combination antioxidants (Vetri. Science Cell Advance®)

Elevated Liver Enzymes in Well Dogs 4. Recheck Liver enzymes in 30 days 5. Proceed with further diagnostics for liver disease if still significantly elevated (2 -3 x) – – – Assess liver function with bile acids Abdominal ultrasound and liver cytology ACTH stim or Low Dose Dex if signs of Cushing’s 6. If Step 4 reveals no significant problems, Proceed to 3 Tier Liver Diagnostics

Pattern Recognition Canine Liver Enzymes • ALT is highest with: – – – • • • Acute hepatic necrosis Primary hepatic neoplasia (except lymphoma) Chronic inflammatory hepatitis Cushing’s Disease without elevated liver enzymes is rare, especially ALKP GGT increases before ALKP in cholestasis Scotties can have very high liver enzymes with no identifiable pathology

Pattern Recognition Canine Liver Enzymes • Most common causes of increased ALKP – – – • Hepatobiliary disease Glucocorticoids (Cushing’s, iatrogenic or stress) (Barbiturate anticonvulsant therapy) Other Causes: – – Cholestasis causing hepatotoxicity Systemic Causes of increased ALKP • • • Sepsis, toxemia Vacuolar hepatopathy Systemic inflammation or infection

Pattern Recognition Canine Liver Enzymes • GGT in dogs is less sensitive but more specific than ALKP for biliary disease in dogs – – • Albumin and BUN most often low with – – – • If GGT is high, the dog probably has biliary disease If GGT is normal, the dog still might have biliary dz chronic inflammatory hepatitis PSS cirrhosis Steroid hepatopathy causes mild if any increase in bile acids

Significant Liver Disease that may show Normal ALT & SAP • End stage liver disease (cirrhosis) • Hepatic Lymphoma ** • Metastatic neoplasia • Portasystemic shunt (especially if advanced) • Feline Cholangiohepatitis • FIP** • Feline pancreatitis** • Histoplasma** **Not uncommon to cause icterus without elevated liver enzymes, in cats

Splenic or Rectal Portagram • 1. Splenic is often preferred to rectal portagram Radioactive isotope put into the rectum or injected into the spleen 2. Put dog on the camera 3. See which lights up first – heart or liver • Liver first = normal • Heart first = PSS (can calculate shunted fraction) • Hospitalized for 1 -3 days Can’t always distinguish • Extrahepatic, intrahepatic, microvascular dysplasia

Pattern Recognition – PSS • Signalment & History – usually but not always a young dog who has been a poor doer and intermittently ill with any symptoms of hepatic disease • may not have done well after first surgery – Sometimes found in older dogs who have been generally well – Most common symptom in cats with PSS: • Hypersalivation • Other common signs – hepatic encephalopathy, GI upset • CBC – low MCV (Microcytosis) • Serum panel – usually a liver pattern, but could possibly be normal – Advanced PSS more likely to be normal than early PSS – Creatinine can be low due to poor muscle mass – Almost never icteric

Pattern Recognition – PSS • Urinalysis – ammonium biurate crystals or stones are 33 - 50% sensitive for PSS • Bile acids – usually markedly elevated – possible but unlikely to have intermittently normal bile acids • Ammonia – almost always elevated • Imaging – small liver – – Congenital – fails to receive trophic factors (80%) Acquired – fibrosis and cirrhosis (20%) • Spenic Portagram – Extrahepatic and Intrahepatic shunts will show shunting which can be measured – Sometimes single shunts, if large, can be visualized on the scan – Microvascular dysplasia will give variable scan results, but often normal

Bile Acids 1. 12 hour fast – red top tube 2. Feed 1 -2 Tablespoons a/d (not low fat – need gallbladder contraction) 3. 2 hour post prandial red top tube Overfeeding can induce HE • • • If not fasted, doing only the post-prandial can be a screen for liver insufficiency Can’t run bile acids on a lipemic sample Don’t bother checking bile acids in an icteric animal – they are high

Bile Acids • The best test we have for liver function, but not entirely specific for liver function • Cholestatic diseases also can elevate bile acids • A very rare urea cycle birth defect can result in hepatic encephalopathy without elevated bile acids – Ammonia levels are very high – Urea cycle enzymes and liver biopsy required for diagnosis, by a lab that is familiar with the disease (call the TAMU GI Lab for information)

Bile Acids Bile acids >30 -40 umol/L in the dog and >20 -30 umol/L in the cat warrant further investigation Idexx SNAP test tells you • • <12 umol/L; 12 -25 umol/L; >25 umol/L Can tell you if a cat needs more work-up, but is of little use in the dog, other than to rule in really healthy liver function “Backwards” bile acids (post-prandial higher) due to blocked enterohepatic circulation or dysbiosis

Bile Acids • Things that decrease bile acids: – – Cholestryamine Severe disease or resection of the ileum Prolonged anorexia Delayed gastric emptying and intestinal hypomotility (delayed delivery to the ileum) – Intestinal malabsorption • Ursodiol increases bile acids • Gallbladder removal makes bile acid assays inaccurate

Ammonia Normal in the dog 20 -80 ug/dl Normal in the cat 20 -120 ug/dl Danger value >1000 ug/dl (HE) • • • Elevated resting ammonia is significant Idexx Vet. Test/Catalyst does ammonia assays Falsely increased by hemolysis Centrifuge and decant within 30 minutes Run assay within 2 hours Sending to outside lab can be difficult

Ammonia Tolerance Test: 1. Sample - 12 hour fast 2. NH 3 Cl capsules 45 mg/lb max dose 3 g PO or 5% solution given rectally 3. Sample - 30 minutes later • Each sample taken in a red top ice chilled tube and kept stoppered and on ice • Increase should be <32% • Nearly 100% sensitive for PSS

Ammonia DO NOT GIVE NH 3 Cl if resting ammonia elevated • • Can induce HE Do not give if any symptoms of HE Can cause vomiting Not recommended for cats Things that increase ammonia • • • Allowing sample to stand too long Valproic acid, asparaginase, narcotics, diuretics, ammonium salts Hyperalimentation, high protein meals, GI bleeding Urinary obstruction with UTI (urease producing bacteria) Bing a juvenile Scottish Deerhound Things that decrease ammonia • Antibiotic therapy, probiotics, lactulose, diphenhydramine • enemas
 • Better than a single bile acid value,")
Urine Bile Acid: Creatinine Ratio (UBAC) • Better than a single bile acid value, if you can’t keep the patient for 2 hours, or can’t make a fractious animal eat • Treatment with ursodiol does not interfere • Hematuria and hemoglobinuria my interfere

Protein C • Plasma anticoagulant that works at the endothelial cell surface • Vitamin K dependent – drops prior to PT, PTT with anticoagulant rodenticides • Low value identifies hypercoagulable state • May help distinguish PSS from MVD – <70% for PSS – >70% for MVD • Rise in Protein C after shunt surgery can mean hepatic flow was re-established • Low in dogs with aflatoxin poisoning • Cornell

Stephen Garner – Nacogdoches TX

Liver Aspiration Cytology • • Side effects very unlikely if platelet count and BMBT normal Hypoechoic lesions or very large liver increase bleeding Sedation rarely necessary, unless fractious Most helpful for: – – – Hepatic lipidosis Histoplasmosis, Cytauxzoon Cholangiohepatitis – inflammation & cholestasis (include CBC) • – Some neoplasias • • Can do bacterial culture & sensitivity if bacterial seen (cat) Good for histiocytic, aggressive carcinoma, MCT, metastasis OK for LSA , moderate grade carcinoma Not food for hepatoma, low grade carcinoma, HSA Least helpful for Fibrosis, PSS

Liver Aspiration Cytology fatty liver normal hepatocytes histoplasmosis, fatty liver hepatic carcinoma

Liver Aspiration Cytology bacterial cholangiohepatitis cytauxzoonosis hepatic carcinoma

Liver Aspiration Cytology metastatic sarcoma histiocytic sarcoma hepatic lymphoma

Liver Aspiration Cytology vacuolar hepatopathy hepatic mast cell tumor

DDx Chronic Inflammatory Liver Dz the disease formerly known as Chronic Active Hepatitis Infectious Canine Hepatitis (CAV 2) Leptospirosis Chronic GI Disease (Leaky Gut) **Copper Storage Disease** ** Autoimmune Disease In many cases, etiology can not be determined, and does not affect treatment choices Early detection is essential, to prevent cirrhosis

PSS Liver Histopath Portasystemic Shunt Microvascular Dysplasia Hepatic atrophy: • Proximity of portal triads • Compressed hepatic cords • Inconspicuous portal veins • End stage cirrhosis if prolonged Hypoplastic portal venules: • Small portal vessels • Portal endothelial hyperplasia • Portal venule dilation Collapse of hepatic lobules Random juvenile intralobular vessels Proliferation of hepatic arterioles • “reduplication” Central vein changes: • Mural hypertrophy • fibrosis

Chronic Inflammatory Liver Dz Histopathology • • • Inflammation starts at the portal triads Then extends to the hepatic lobule Eventual necrosis and bridging fibrosis between adjacent portal areas Then nodular hyperplasia Then cirrhosis Other frequent characteristics: • • • Cholestasis – treat with ursodiol Inflammation predominantly mononuclear Suppurative inflammation suggests bacteria Bile duct hyperplasia (reduplication) and cholestasis Secondary copper accumulation can accelerate disease

Chronic Inflammatory Liver Dz Histopathology • • • Inflammation starts at the portal triads Then extends to the hepatic lobule Eventual necrosis and bridging fibrosis between adjacent portal areas Then nodular hyperplasia Then cirrhosis Other frequent characteristics: • • • Cholestasis – treat with ursodiol Inflammation predominantly mononuclear Suppurative inflammation suggests bacteria Bile duct hyperplasia (reduplication) and cholestasis Secondary copper accumulation can accelerate disease

Feline Cholangiohepatitis Forms: • • Lymphocytic-plasmacytic – immune mediated Eosinophilic – immune mediated, parasitic Suppurative - bacterial End stage – biliary cirrhosis (rare) Concurrent Problems: • • • Triaditis – pancreatitis, IBD Bile duct obstructions, cholelithiasis Sepsis Abdominal pain indicates bacterial cholangiohepatitis or bacterial cholecystitis in dogs and cats

Gall Bladder Aspiration • The only indication is culture and sensitivity – • For chronic bacterial cholangiohepatitis/cholangitis Easily performed with ultrasound guidance if gall bladder is enlarged Deep sedation or short general anesthesia is required • – – To prevent gall bladder rupture Rupture can happen even if all goes well Rupture requires emergency surgery repair Risky in practices without 24 -hour care

Icterus Wendy Blount, DVM Practical. Vet. Med Seminars

Detecting Icterus • Yellow to orange serum/plasma - >1 mg/dl bili • orange urine – renal threshold > 0. 6 -0. 8 mg/dl bili

Detecting Icterus • Bilirubinuria • Mild to moderate bilirubinuria can be normal in the dog • Never normal in the cat – Cats have higher renal threshold for bili than dogs – Can be used to monitor cholestatic disease at home

Detecting Icterus • Icteric eyes, mucous membranes and skin > 2 -3 mg/dl

Detecting Icterus • Icterus on exam – 2. 0 -3. 0 mg/dl – – • Can be seen at lower bili if cholestasis More delta bilirubin that is not cleared by the kidneys Most common cause of icterus in the cat – • Feline Cholangiohepatitis (bacterial) Most common cause of icterus in the dog – canine inflammatory hepatitis (immune mediated)
 – RBC destroyed at a high rate, faster than")
DDx Icterus 1. Pre-Hepatic (hemolysis) – RBC destroyed at a high rate, faster than the liver can process the Hb & conjugate the bili (PCV <20%) 2. Hepatic (hepatocellular disease) – Liver cells cannot conjugate the bili to be excreted by the gall bladder – Happens when <10% of liver function remains 3. Post-Hepatic (bile duct obstruction) – Bile duct obstructed – cannot excrete bili into the duodenum

DDx Icterus Hepatic and post-hepatic icterus are difficult to separate • • Bile acids retained by obstruction are hepatotoxic Ultrasound is the best to determine cause of hepatic and/or post-hepatic icterus

Candace Novak – Lake Jackson TX
 2. Cholangiohepatitis – bacterial, fungal")
DDx Hepatic Icterus • Cats 1. Hepatic Lipidosis (30%) 2. Cholangiohepatitis – bacterial, fungal (20%) 3. Lymphoma (20%) – FIP – Drug toxicity (methimazole, diazepam) – Sepsis – Protozoal – Cytauxzoon spp

DDx Hepatic Icterus • Dogs – DDx acute hepatic failure – Sepsis – pyometra, prostatitis, GI obstruction, fight wounds, pneumonia, pyelonephritis, etc. – Leptospirosis – Acute hepatic necrosis – Toxicity (next slide) – Exacerbation of chronic liver disease – Viral – infectious canine hepatitis (CAV 2) – SIRS

Hepatotoxins • • • • Acetaminophen Aflatoxins Anabolic Steroids Anticonvulsants Antineoplastics Arsenicals Blue Green Algae Carprofen Castor Beans (Ricin) Diazepam Diethylcarbamazine Griseofulvin Iron – chronic overdose • • • • Itraconazole Kava Ketoconazole Mebendazole Mitotane Mushrooms (Amanita) Oxabendazole Phenols (Lysol®) Sago Palm (seeds) Sulfonamides Thiabendazole TMPS Xylitol
 - #1 2. Gall bladder mucocoele,")
DDx Post-Hepatic Icterus Most common: 1. Pancreatitis (15%) - #1 2. Gall bladder mucocoele, cholecystitis – dogs #2 3. Neoplasia (10%) – liver, bile duct, pancreas, duodenum

DDx Post-Hepatic Icterus Less common causes of post-hepatic icterus • Pancreatic abscess, neoplasia or granuloma • Liver, Bile Duct, Duodenal Abscess or Granuloma, severe IBD • Cholelithiasis or inspissated bile plugs • Duodenal foreign body • parasite migration, pancreatic or liver flukes

Icterus Work-Up 1. MDB - CBC, panel – Anemia, icterus pursue hemolysis • – – <20% in the cat, <25% in the dog No anemia – pursue liver dz, bile obstruction Remember that icteric cats can have ACID (nonregenerative – need a retic count to be sure) 2. Imaging - Abdominal rads & ultrasound – liver, pancreas 3. Sample the liver + bile – Cytology, histopathology, culture/sensitivity 4. Syndrome specific diagnostics
 DDx - FIP,")
Cats with elevated bili and normal liver nz (ALT & SAP) DDx - FIP, Hepatic lymphoma, Pancreatitis, Histoplasma Diagnostic Trifecta for FIP 1. 2. 3. • • Lymphopenia <1500/ul Coronavirus titer 1: 160 or greater Globulins >5. 1 g/dl Positive predictive value 89% Negative predictive value 99% Histopath and fluid analysis supportive Fluid analysis chart – pancreatitis section

Icterus Thumb Rules • • • Danger value for bili <20 mg/dl dogs (kernicterus brain toxicity, renal toxicity); cats unknown PSS and steroid hepatopathy patients are almost never icteric Slight elevations in bili are rarely clinically significant Lipemia & hemolysis falsely elevate bili Measurement of direct (conjugated) and indirect (unconjugated) fractions is not useful because hemolytic, hepatic an biliary tract diseases have unpredictable variation in each fraction

Summary Power. Points -. pptx, . pdfs – 1 and 6 slides per page Vet Handouts • • Blount - Bicarbonate administration Blount - Fluid analysis diagnostic chart Blount - IV potassium supplementation Idexx – SNAP Bile Acids Willard – Algorithm for Increased ALT Willard – Algorithm for increased ALKP Willard – Algorithm for increased Bili

Summary Client Handouts • • • Cholangiohepatitis Chronic Liver Disease Fatty Liver Icterus Portasystemic Shunt Hidden Slides • AST Gems • Prehepatic Icterus

Summary Cases -. pptx, . pdfs 1 & 6 slides per page • • • Diego – microvascular dysplasia Pockets – chronic inflammatory liver disease Popcorn – cirrhosis Benzer – acute hepatic necrosis Sebastian – chronic and acute liver failure, GI ulcer

Acknowledgments • Dr. Adam Honeckman, ACVIM. “Icteric Cats – More than Just Lipidosis. ” Mobile Veterinary Diagnostics, Orlando, FL. • De. Novo RC, Chapter 5, “Diseases of the Stomach, ” in Todd R Tams Small Animal Gastroenterology, 2 nd Edition. • Richter KP, Chapter 9, “Diseases of the Liver and Hepatobiliary System, ” in Todd R Tams Small Animal • Gastroenterology, 2 nd Edition.

Acknowledgments • Stacy Simmonds, DVM, DACVECC • Emergency Animal Hospital of Northwest Austin • Michael Connolly, DVM • Connolly Animal Clinic, Nacogdoches TX • Tam Garland, DVM, Ph. D, DABVTT • Toxicology Consultant • Adam Honeckman, DACVIM • Mobile Veterinary Diagnostics, Orlando FL

Acknowledgments • Margie Scherck, DABVP, VIN Consultant • Willard MD and Tvedten H. Small Animal Clinical Diagnosis by Laboratory Methods, 5 th ed. Chapter 7 – Gastrointestinal, Pancreatic and Hepatic Disorders. Eds Willard MD and Tvedten H. 2014.
- Slides: 76