Power Lecture Chapter 16 Reproductive Systems Learning Objectives

Power. Lecture: Chapter 16 Reproductive Systems

Learning Objectives Ø Ø Ø Describe the structure and function of the human male and female reproductive systems. Describe the actions and interactions of the hormones regulating reproduction. List the events and timing of the menstrual cycle. Know the principal means of controlling human fertility. Describe the major sexually transmitted diseases and how to avoid getting them.

Impacts/Issues Sperm with a Nose for Home?

Sperm with a Nose for Home? Human sperm have olfactory receptors. Ø l l Researchers are attempting to identify the chemical that is produced by human eggs to attract the sperm. This knowledge could be used to attract more sperm to eggs to treat infertility; conversely such information could be used to create a new type of contraceptive.

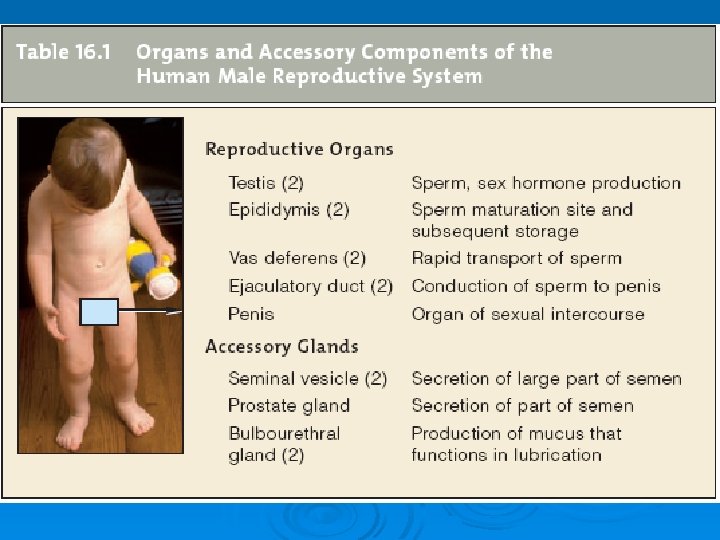
Sperm with a Nose for Home? The male and female reproductive systems are the only body systems that do not contribute to homeostasis; their only role is to reproduce the species. Ø l l Male and female reproductive systems consist of primary reproductive organs, the gonads, plus accessory glands and ducts. Male gonads are testes, which produce sperm; female gonads are ovaries, which produce eggs.

How Would You Vote? To conduct an instant in class survey using a classroom response system, access “Join. In Clicker Content” from the Power. Lecture main menu. Ø Would you support a law that requires unmarried minors to get a parent’s written consent in order to obtain contraceptives? l l a. Yes, teens have the right to sexual privacy; if they didn't, it might discourage use of contraception. b. No, parents should have the right to know all issues regarding their minor child's health.

Section 1 The Male Reproductive System
 develop from germ cells. Ø l l")
The Male Reproductive System Sperm (and eggs) develop from germ cells. Ø l l l Human germ cells possess the diploid number of chromosomes (46) and eventually give rise to sperm and egg cells. Sperm and egg cells are called gametes; gametes have only half the total number of chromosomes (23) and are thus called haploid. Haploid gametes meet at fertilization to restore the diploid number of chromosomes.

The Male Reproductive System Sperm form in the testes. Ø l l The testes reside in the scrotum, which must remain a few degrees cooler than body temperature to allow for proper sperm development. Each testis contains a large number of small, highly coiled tubes called the seminiferous tubules; sperm begin their formation within these tubules.

pelvic girdle urinary bladder scrotum Fig. 16. 2, p. 291

The Male Reproductive System Sperm mature and are stored in the coiled epididymis. Ø l l Sperm are not quite mature when they leave the testes, so they are stored in the epididymides (singular: epididymis) for a period of time. During ejaculation the sperm move from the epididymides through the vas deferentia (singular vas deferens)>>> ejaculatory ducts >>> urethra (inside the penis).

The Male Reproductive System Substances from seminal vesicles and the prostate gland help form semen. Ø l l The sperm bearing fluid—semen—is formed by secretions from the seminal vesicles (fructose and prostaglandins) and the prostate gland (buffers against acidic vagina). The bulbourethral glands secrete a mucus rich fluid into the urethra during sexual arousal. A typical ejaculation contains from 150 to 350 million sperm. The testes and prostate gland are both sites of cancer in men.

Animation: Male Reproductive System CLICK TO PLAY

ejaculatory duct prostate gland urinary bladder urethra seminal vesicle anus urethra bulbourethral gland vas deferens erectile tissue penis testis © 2007 Thomson Higher Education epididymis Fig. 16. 1, p. 290

Section 2 How Sperm Form

How Sperm Form Sperm form in seminiferous tubules. Ø l Each testis is divided into lobes (up to 30) containing the seminiferous tubules (2 3 tubules per lobe). • • The walls of the tubules contain spermatogonia, where sperm formation begins. Two processes of cell division are necessary for sperm formation: mitosis and meiosis.

vas deferens seminal vesicle prostate gland bulbourethral gland urethra penis epididymis testis seminiferous tubule Fig. 16. 3 a, p. 292

Animation: Route Sperm Travel CLICK TO PLAY

How Sperm Form l Diploid spermatogonia undergo mitosis >>> primary spermatocytes, which undergo meiosis I >>> haploid secondary spermatocytes, which undergo meiosis II >>> haploid spermatids >>> mature sperm (spermatozoa).
 primary spermatocyte secondary early late spermatocyte")
mitosis meiosis II lumen Sertoli cell spermatogonium (diploid) primary spermatocyte secondary early late spermatocyte spermatids spermatid immature sperm (haploid) c Part of the lumen of one seminiferous tubule Fig. 16. 3 c, p. 293

Animation: Spermatogenesis CLICK TO PLAY

How Sperm Form l l Sertoli cells lining the seminiferous tubules provide nourishment and chemical signals to the developing sperm. Each sperm has a head (containing DNA and the caplike acrosome), midpiece (mitochondria), and tail (microtubules of the flagellum). Figure 16. 3 d

How Sperm Form Hormones control sperm formation. Ø l Testosterone, produced by Leydig cells located between the lobes in the testes, promotes the formation and function of reproductive organs, formation of secondary sexual traits, and stimulates sexual behavior.

wall of seminiferous tubule © 2007 Thomson Higher Education Leydig cells between tubules Fig. 16. 3 b, p. 292
, released from the anterior pituitary")
How Sperm Form l l l Luteinizing hormone (LH), released from the anterior pituitary under influence from Gn. RH from the hypothalamus, stimulates testosterone production. Gn. RH also causes the pituitary to release FSH (follicle stimulating hormone), which stimulates the production of sperm (spermatogenesis), beginning at puberty. Negative feedback loops regulate the release of these hormones.

Animation: Hormonal Control of Sperm Production CLICK TO PLAY

a Level of testosterone in blood decreases, the hypothalamus secretes Gn. RH, a releasing hormone. (+) (—) Hypothalamus f Elevated level of testosterone in blood inhibits secretion of Gn. RH. (—) f High sperm count induces (—) sertoli cells to secrete inhibin, which inhibits secretion of Gn. RH and LH. Anterior pituitary b Gn. RH stimulates secretion of LH, FSH from anterior lobe of pituitary. (+) Testis c LH prompts Leydig cells In tests to produce and release testosterone. d Sertoli cells bind FSH and testosterone, and function in spermato genesis at puberty. e Testosterone is used to stimulate formation and development of sperm Fig. 16. 4, p. 293

Section 3 The Female Reproductive System

The Female Reproductive System The ovaries are the primary reproductive organs of females Ø l Ovaries release sexual hormones and produce eggs. • • Ovarian hormones influence the development of female secondary sexual traits. The immature egg (oocyte) is released from the ovary >>> oviduct (fallopian tube, where fertilization may occur) >>> uterus (where a baby can grow and develop). Figure 16. 21

ovary uterus oviduct vagina bladder Fig. 16. 5 a, p. 294
 and")
The Female Reproductive System l l The uterus consists of smooth muscle (myometrium) and an inner lining called the endometrium; the lower part of the uterus is the cervix, which extends into the vagina, which in turn leads to the body surface. The external genitals (vulva) include organs for sexual stimulation. • • Labia majora are outer folds of skin; labia minora lie within the major folds. The clitoris, an organ developmentally analogous to the penis, is sensitive to stimulation.

The Female Reproductive System l In females, the urethra is separate and is not involved in reproduction.

Animation: Female Reproductive System CLICK TO PLAY

oviduct uterus ovary myometrium urinary bladder endometrium opening of cervix urethra clitoris labium minor labium major vagina anus Fig. 16. 5 b, p. 295

The Female Reproductive System During the menstrual cycle, an oocyte is released from an ovary. Ø l Female humans have a menstrual cycle of about 28 days. • • During the cycle, an oocyte matures and is released from the ovary. The endometrium will be primed by hormones to receive an embryo if fertilization occurs; if there is no fertilization, the lining is shed during menstruation.

The Female Reproductive System l Menstruation has several phases. • • • The menstrual phase is the phase where shedding of the endometrium occurs. During the proliferative phase, new endometrium is formed; the end of the phase coincides with ovulation (release of an egg). The final phase, the progestational phase, sees the formation of the corpus luteum, which secretes progesterone and estrogen, the two hormones that prime the endometrium for pregnancy.
 occurs during puberty (generally")
The Female Reproductive System l l The first menstruation (menarche) occurs during puberty (generally between the ages of 10 16); the last marks menopause (late 40 s or early 50 s). Endometriosis is a painful condition where endometrial tissue spreads and grows outside of the uterus; this can lead to infertility.

Section 4 The Ovarian Cycle: Oocytes Develop

The Ovarian Cycle: Oocytes Develop In the ovarian cycle, hormones guide the steps leading to ovulation. Ø l At birth about 2 million primary oocytes (immature eggs) are present and arrested in meiosis I; all but about 300 are later absorbed, the rest to complete meiosis, generally one at a time, during each ovarian cycle. • • The follicle consists of a layer of granulosa cells surrounding the primary oocyte. At the start of the cycle, coordinated efforts by Gn. RH, FSH, and LH stimulate the follicle to grow; a zona pellucida forms around the follicle.

The Ovarian Cycle: Oocytes Develop • • l Estrogen is secreted and the follicle becomes a secondary or Graafian follicle. Several hours before being released, the oocyte completes meiosis I to form two cells. One of the two cells is large and is called the secondary oocyte, the other cell is smaller and is called the first polar body. • • The secondary oocyte is haploid and begins meiosis II; meiosis II will be arrested in preparation for fertilization. The first polar body may divide again; it also is haploid.

The Ovarian Cycle: Oocytes Develop l At about midcycle, there is a surge of LH that causes ovulation—the release of the secondary oocyte following rupture of the follicle wall. • • Once released, the secondary oocyte enters an oviduct; long, ciliated projects from the oviduct called fimbriae sweep the oocyte into the channel. If fertilization occurs, it usually occurs in the oviduct; fertilization allows for the completion of meiosis II, at which point the oocyte is a mature ovum (egg).

The Ovarian Cycle: Oocytes Develop The ovarian cycle dovetails with the menstrual cycle. Ø l l l Estrogens released during the first half of the menstrual cycle stimulate growth of the endometrium; at ovulation the estrogens stimulate the cervix to secrete mucus for the sperm to swim through. After ovulation, granulosa cells differentiate into the corpus luteum; this structure persists for about 12 days following ovulation, secreting progesterone that inhibits further FSH and LH secretion. If fertilization does not occur, the corpus luteum degenerates, progesterone and estrogen levels fall, and FSH and LH are again secreted to begin another cycle.

Animation: Ovarian Function CLICK TO PLAY

a A primordial follicle. Inside, meiosis I has been arrested in the primary oocyte. b A zona pellucida starts forming around the oocyte. primordial (“first”) follicle c A fluid filled cavity (antrum) starts forming in the follicle. ovary d Mature follicle Meiosis I is over. The secondary oocyte and first polar body are now formed. first polar body secondary oocyte g The corpus luteum breaks down when the woman doesn't get pregnant. f A corpus luteum forms from remnants of the ruptured follicle e Ovulation. The mature follicle ruptures, releasing the secondary oocyte and first polar body. Fig. 16. 6, p. 296

Animation: Hormones and the Menstrual Cycle CLICK TO PLAY
 c Blood level of estrogen rises, will stimulate a surge in LH")
hypothalamus (+) c Blood level of estrogen rises, will stimulate a surge in LH secretion (-) pituitary (+) a Gn. RH prods anterior lobe cells to secrete FSH and LH b In ovary, FSH and LH promote follicle growth and oocyte maturation, estrogen production, priming of endometrium, other reproductive events © 2007 Thomson Higher Education (-) f The rise in progesterone, estrogen in blood will inhibit FSH, LH secretion during last phase of cycle d Midcycle surge of LH triggers ovulation, then formation of corpus luteum e Progesterone, estrogen secreted by corpus luteum will maintain the endo metrium if pregnancy occurs Fig. 16. 7, p. 297

Video: Follicular Phase CLICK TO PLAY

Video: Ovulation and Luteal Phase CLICK TO PLAY

Section 5 Visual Summary of the Menstrual and Ovarian Cycles

Animation: Menstrual Cycle Summary CLICK TO PLAY
 and LH (lavender) FSH")
hypothalamus Gn. RH anterior pituitary blood levels of FSH (purple) and LH (lavender) FSH midcycle peak of LH (triggers ovulation) LH LH ovulation growth of follicle endometrium of uterus corpus luteum estrogens progesterone, estrogen ovary menstruation Days of menstrual cycle (28 days average duration) 5 follicular phase 14 luteal phase 28 Fig. 16. 8, p. 298

Section 6 Sexual Intercourse

Sexual Intercourse Sexual intercourse involves physiological changes in both partners. Ø l l Technical terms for sexual intercourse are coitus and copulation. The male sex act involves an erection, or stiffening of the penis, and ejaculation, the forceful expulsion of semen. • • The tip of the penis (the glans penis) contains sensory receptors activated by friction. In male sexual arousal, the spongy tissue spaces inside the penis become filled with blood to cause an erection.

Sexual Intercourse l l l In female arousal, blood vessels in the genital area dilate, causing engorgement, and glands secrete lubricants. During coitus, mechanical stimulation of the penis causes involuntary contractions that force semen out and into the vagina; a sphincter closes off the male’s bladder to prevent urine from being secreted. Ejaculation in the male and similar contractions in the female are termed orgasm.

Sexual Intercourse can produce a fertilized egg. Ø l l Within 30 minutes after ejaculation, muscle contractions in the uterus move the sperm deeper into the female reproductive tract. Only a few hundred sperm of the millions released will reach the upper portion of the oviduct, which is where union of egg and sperm (fertilization) will take place. Figure 16. 9

Section 7 Controlling Fertility

Controlling Fertility Natural birth control is chancy. Ø l l l The most effective method of birth control is abstinence, but this may be unrealistic. In the rhythm method (also called fertility awareness or sympto-thermal method) there is no intercourse during the days when an egg is capable of being fertilized; the rhythm, however, may be misjudged. Withdrawal before ejaculation would seem to be effective but is not, due to lapses in will power and premature release of fluids.

Controlling Fertility l Douching is similarly ineffective due to the speed with which sperm enter the uterus. Surgical solutions are reliable. Ø l l In a vasectomy the vas deferentia are cut and tied to prevent sperm delivery; in an alternative procedure (Vasclip) a hinged clip is used to close off the vas deferens. In a tubal ligation the oviducts are cut and tied.

severed sections of vas deferens testis ovary a severed oviduct b Fig. 16. 11, p. 300

Controlling Fertility Physical and chemical barriers vary in effectiveness. Ø l l l Spermicidal foam and jelly are toxic to sperm but not reliable unless used in combination with a barrier device. The diaphragm is a circular rubber device that fits over the cervix and prevents entry of sperm into the uterus; the cervical cap is a similar, but smaller, device. The contraceptive sponge is a soft, disposable disk that fits over the cervix and delivers a dose of spermicide.
 is a small plastic or")
Controlling Fertility l l l The intrauterine device (IUD) is a small plastic or metal device that is placed in the uterus to prevent implantation. Condoms (either worn over the penis or placed inside the vagina) prevent sperm deposition in the vagina but must be used with care. The birth control pill contains synthetic female hormones and prevents ovulation when taken faith fully according to directions; Nuva. Ring is a flexible plastic ring that fits in the vagina and releases the same hormones used in birth control pills.

Controlling Fertility l l l A single injection of Depo-Provera prevents ovulation for up to three months; Norplant is an implant of capsules that deliver a hormone to prevent implantation for up to five years. The drug RU 486 (morning-after pill) interferes with hormone function to prevent implantation if taken within 72 hours after intercourse. Future fertility control options include biodegradable implants and male contraceptives that reduce sperm count.
 100% 99. 6%")
EXTREMELY EFFECTIVE Total abstinence Tubal ligation or vasectomy Hormonal implant (Norplant) 100% 99. 6% 99% HIGHLY EFFECTIVE 98% 96% 95% 94% IUD + slow release hormones IUD + spermicide Depo Provera injection IUD alone High quality latex condom + spermicide with nonoxynol 9 Oral contraceptive EFFECTIVE Cervical cap Latex condom alone Diaphragm + spermicide Billings or sympto thermal rhythm method Vaginal sponge + spermicide Foam spermicide MODERATELY EFFECTIVE Spermicide cream, jelly, suppository Rhythm method (daily temperature) Withdrawal Condom (cheap brand) UNRELIABLE Douching Chance (no method) 89% 86% 84% 83% 82% 75% 74% 70% 40% 10% © 2007 Thomson Higher Education Fig. 16. 10, p. 300

Controlling Fertility Abortion is highly controversial. Ø l l Induced or surgical abortion removes or dislodges an implanted embryo or fetus from the womb; more than 1. 5 million abortions are performed in the US each year. During the first trimester (12 weeks), abortions are generally free of complications; late term abortion is highly controversial unless the mother’s life is in danger.

Video: Bonus for a Baby CLICK TO PLAY Ø From ABC News, Biology in the Headlines, 2005 DVD.

Section 8 Options for Coping with Infertility

Options for Coping with Infertility Fertility drugs stimulate ovulation. Ø l Some forms of female infertility are due to irregular or absent ovulation; fertility drugs may “correct” the problem. • • l Clomiphene stimulates FSH production by the pituitary gland to trigger ovulation. Human menopausal gonadotropin (h. MG), a purified form of FSH, can also be used. Fertility drugs can result in high risk, multiple child pregnancies. Figure 16. 12

Options for Coping with Infertility Assisted reproductive technologies include artificial insemination and IVF. Ø l Artificial insemination was one of the first assisted reproductive technologies (ARTs). • • In artificial insemination, semen is placed directly in the vagina or uterus by mechanical means at the time of ovulation. In artificial insemination by donor (AID), a sperm bank provides the sperm.
 is “fertilization in glass.")
Options for Coping with Infertility l In vitro fertilization (IVF) is “fertilization in glass. ” • • IVF involves removing oocytes and placing them in a solution with sperm; if fertilization occurs, zygotes are carefully tended until a two to four day old embryo can be transferred to the mother’s uterus. Externally conceived embryos implant successfully in only about 20 percent of the attempts; what to do with unused embryos is controversial. Figure 16. 12

Assisted Reproductive Technologies Figure 16. 13
 uses a")
Options for Coping with Infertility l l l ICSI (intracytoplasmic sperm injection) uses a needle to inject a single sperm into an egg. In GIFT (gamete intrafallopian transfer) a couple’s sperm and oocytes are collected and placed in an oviduct in hopes of achieving fertilization. In ZIFT (zygote intrafallopian transfer), fertilization is achieved in a laboratory dish, followed by transfer of the zygote to an oviduct.

Options for Coping with Infertility l IVF with embryo transfer involves inseminating a fertile female volunteer with sperm from a man whose partner is infertile; resulting embryos are transferred to the infertile woman’s uterus or a surrogate, but because of legal complications, this procedure is uncommon.

Section 9 A Trio of Common Sexually Transmitted Diseases

A Trio of Common Sexually Transmitted Diseases Chlamydial infections and PID are most common in young people. Ø l One of the most common sexually transmitted diseases (STDs) is chlamydia, caused by the bacterium Chlamydia trachomatis. • • Millions of people become infected each year through sexual contact, most of them younger than 25; the organism can also be transmitted to infants at birth. Discharge from the penis or vagina, along with a burning sensation, may accompany infection, but often infection is “silent. ”

A Trio of Common Sexually Transmitted Diseases l Antibiotic treatment can cure chlamydial infections, but approximately 1 million women each year will, without treatment, develop pelvic inflammatory disease (PID). • • This condition is the result of the invasion of the uterus, oviducts, and ovaries by microorganisms that are associated with STDs. Antibiotics are used, but may not be sufficient, in which case surgery is required. Figure 16. 14 a

A Trio of Common Sexually Transmitted Diseases Gonorrhea may initially have no symptoms. Ø l l The bacterium Neisseria gonorrhoeae causes gonorrhea, an infection of the epithelium of the genital tract, rectum, eye, and throat. Treatment is with antibiotics but new resistant strains are becoming troublesome. Figure 16. 14 b

A Trio of Common Sexually Transmitted Diseases l It is difficult to assess the numbers of cases because the initial stages are so uneventful that the carrier may be unaware of the infection; however, as many as 10 million unreported cases may occur every year in the US. • • Males will experience pus issuing from the penis and painful urination. Females are often asymptomatic or have very mild symptoms until after the bacteria have spread to the oviducts.

A Trio of Common Sexually Transmitted Diseases Syphilis affects a wide range of organs. Ø l l Each year, an estimated 12 million new cases of syphilis caused by the bacterium Treponema pallidum are diagnosed in the US. Treatment is with penicillin during the early stages. Figure 16. 15 b

A Trio of Common Sexually Transmitted Diseases l The disease produces long term infection, which can be divided into three stages: • • • In the primary stage, a chancre teeming with bacteria is visible at the site of exposure. A couple of months later, during the secondary stage, lesions develop in the mucous membranes, eyes, bones, and central nervous system. The tertiary stage begins from 5 to 20 years after infection and results in lesions in the skin and internal organs, including the liver, bones, and aorta. Figure 16. 15 a

Section 10 The Human Immunodeficiency Virus and AIDS Figures 16. 17 and 16. 20

Video: AIDS Conference in Brazil CLICK TO PLAY Ø From ABC News, Environmental Science in the Headlines, 2005 DVD.

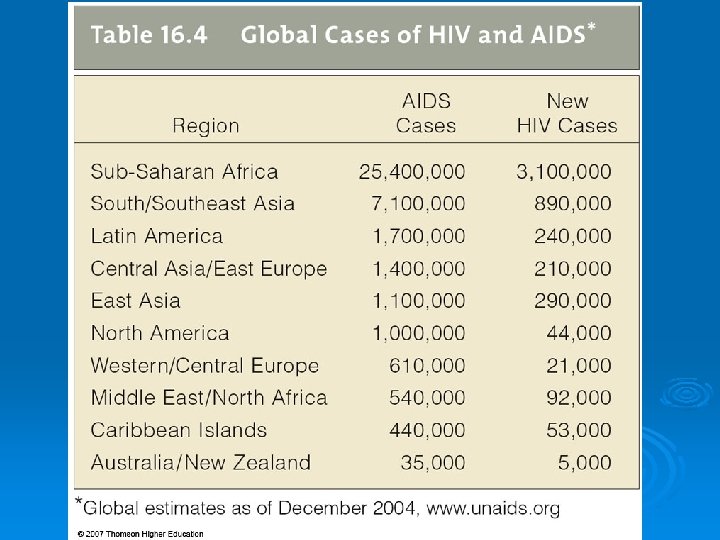
The Human Immunodeficiency Virus and AIDS is a group of diseases caused by the human immunodeficiency virus (HIV), which cripples the immune system. Ø l l l Signs of AIDS are a depressed immune system, presence of HIV, and one or more “indicator diseases. ” Worldwide infections number between 34 and 46 million people. Almost half of HIV infected adults worldwide are women; young adults are also at high risk in the US and elsewhere. Figure 16. 16

The Human Immunodeficiency Virus and AIDS HIV is transmitted by body fluids— especially blood and semen. Ø l l l Blood can be transmitted through cuts; abrasions; objects such as toothbrushes; needles used for drugs, ear piercing, and tattoos; and medical equipment. The most common mode of transfer is sex with an infected partner; pre existing STDs can increase the chances of HIV transmission. HIV is also transmitted from mother to child during pregnancy, birth, and during breast feeding.

The Human Immunodeficiency Virus and AIDS HIV infection begins a titanic struggle. Ø l HIV is a retrovirus. It has RNA as its genetic material surrounded by some protein and a lipid envelope; the genetic material is accompanied by reverse transcriptase. • • • Inside a host cell, viral RNA is transcribed into DNA, which becomes integrated into the host cell’s DNA where it remains. HIV can only infect cells with specific surface markers; macrophages, dendritic cells, and helper T cells all have this marker. Later, the DNA will be transcribed to make more viral particles.

The Human Immunodeficiency Virus and AIDS l Once a person is infected, HIV particles begin to circulate in the blood. • • • Initial symptoms may appear like the flu, and at this point the immune system controls HIV by producing antibodies and T cells against the virus and infected cells. As the disease progresses, 2 billion helper T cells become infected, with the resulting production of 100 million to 1 billion virus particles per day; eventually more and more virus is produced and fewer helper T cells remain to fight infection. Increased symptoms of disease and vulnerability to more and more infections as the immune system fails are hallmarks of AIDS.

Animation: HIV Replication Cycle CLICK TO PLAY

The Human Immunodeficiency Virus and AIDS l A small percent of HIV infected people do not develop the symptoms of illness due to less virulent strains of HIV or some inborn resistance to the virus.
 c The viral DNA becomes integrated into")
viral coat proteins viral enzyme (reverse transcriptase) c The viral DNA becomes integrated into host cell’s DNA. a Viral RNA enters a CD 4 lymphocyte. viral RNA lipid envelope with proteins b Viral DNA forms by reverse transcription of viral RNA. d DNA, including the viral genes, is transcribed. nucleus f Virus particles that bud from the infected cell may attack a new one. viral RNA viral DNA viral proteins e Some transcripts are new viral RNA, others are translated into proteins. Both self -assemble into new virus particles. Fig. 16. 17, p. 307

The Human Immunodeficiency Virus and AIDS What about drugs and vaccines? Ø l There are several drugs currently available, which are typically used in “cocktails. ” • • • Protease inhibitors prevent the assembly of new HIV particles, other drugs inhibit the enzymes HIV needs to replicate itself. The preferred cocktail consists of a protease inhibitor and two anti HIV drugs and is effective for a relatively short time; side effects and drug resistance are both problems. “Entry inhibitors” are another approach to blocking HIV entry into cells.

The Human Immunodeficiency Virus and AIDS l Vaccines work by stimulating the immune system to make antibodies against antigens made by the invading virus. • • • HIV changes rapidly and replicates in the immune system, making immune function less efficient. A single individual may have different genetic forms of HIV. One approach to a vaccine consists of producing a synthetic HIV virus that can stimulate immunity without replicating.

Section 11 A Rogue’s Gallery of Other STDs

A Rogue’s Gallery of Other STDs Genital herpes is a lifelong infection. Ø l Genital herpes follows infection with herpes simplex viruses, which are very contagious. • • Any part of the body that comes in contact with the viral filled sores can be invaded, including mucous membranes in the mouth and on the genitals. Roughly 45 million people have one of the two strains of HSV that cause the disease; type 1 strains infect the lips, tongue, mouth, and eyes, while type 2 strains cause most of the genital infections.

A Rogue’s Gallery of Other STDs l l Symptoms develop within 2 weeks of infection and after the first sores disappear, sporadic reactivation of the virus can produce new, painful sores. There is no cure for herpes infection but antiviral drugs can inhibit viral replication. Figure 16. 18 b

Video: Herpes Replication CLICK TO PLAY

A Rogue’s Gallery of Other STDs Human papillomavirus can cause cancer. Ø l l l Genital warts are painless growths caused by the human papillomavirus (HPV). More than 80 percent of cases of invasive cervical cancer are caused by certain strains of HPV. Women with a history of genital warts may need to have a Pap smear done annually. Figure 16. 18 a

A Rogue’s Gallery of Other STDs Hepatitis can be sexually transmitted. Ø l Hepatitis B virus, like HIV, can be transmitted in blood and body fluids, but it is far more contagious than HIV, and the number of sexually transmitted cases is growing. • • l The virus attacks cells in the liver, causing jaundice; long term infection can lead to cirrhosis or cancer. The only treatment is rest but vaccination is available. Hepatitis C virus is carried in the blood and can reside in the body for years before symptoms appear.

A Rogue’s Gallery of Other STDs Some STDs are caused by parasites. Ø l Pubic lice, or “crabs, ” are small parasites that cling tenaciously to pubic hair and feed on the underlying tissues, causing itching and irritation. Figure 16. 19 a

A Rogue’s Gallery of Other STDs l l Candidiasis, or yeast infections caused by Candida albicans, occurs when conditions inside the vagina change, allowing overgrowth of the yeast; infections can be passed to male partners, but in any case treatment is with over the counter antifungal preparations. Trichomonas vaginalis is a protozoan that can cause severe inflammation of the vagina (trichomoniasis); men can also become infected. Figure 16. 19 b

Section 12 Eight Steps to Safer Sex

Eight Steps to Safer Sex Ø Only individuals who are celibate (do not have sex) or have long term, mutually monogamous relationships are not at risk for STDs.

Eight Steps to Safer Sex Some ways to minimize risk include the following: Ø l l l Use a latex condom, especially paired with a spermicide, and limit yourself to one partner who only has sex with you. A frank discussion of past sexual histories is helpful. Be aware of sores, discharge, or other signs of infection in you and your partner; abstain from sex if you believe you have been exposed to an STD, and seek medical help.

Eight Steps to Safer Sex l l Avoid abusing alcohol or drugs, which impair awareness of actions. If treatment is necessary, complete your treatment and don’t share medications.
- Slides: 104