Potassium balance and clinical disorders Mohamed Osama Ezwaie

Potassium balance and clinical disorders Mohamed Osama Ezwaie, MD Associate professor of medicine and nephrology

Learning Objectives • • Vital functions of Potassium ion Potassium balance Factors influencing internal and external potassium balance Hypokalemia: ▫ Etiology ▫ Clinical features and diagnostic approach ▫ Therapy • Hyperkalemia: ▫ Etiology ▫ Clinical features and diagnostic approach ▫ Therapy; urgent and non-urgent

Potassium ion vital functions • Normal p. K+: 3. 5 -5. 5 m. Eq/L • Vital functions: ▫ Maintains cell electro-neutrality ▫ Assists in conduction of nerve impulse ▫ Directly affects cardiac and skeletal muscle contraction; repolarization phase of action potential ▫ Plays a major role in acid-base balance

Potassium balance • Major intracellular cation (98% of total K 140 -160 m. Eq/ L) , which is maintained by Na-K ATPase pump, required for maintaining electric potential across cell membrane for neuromuscular activity • Intracellular : extracellular ratio K 49: 1, ( 3. 5 -5. 5 m. Eq/L), small shift from ICF to ECF can result in large increase of seum K, and exert profound effects on the resting membrane potential.

Potassium balance • Normal kidneys excretion varies with intake 10 -400 m. Eq/ day • Daily K balance should be 60 -80 m. Eq/ day • Maintaining potassium homeostasis is made more complex because K continously derived from diet added to ECF more quickly than kidney excretes it • Renal failure patient GFR < 2 O ml/ min ? ?

Distribution of potassium • Clinical estimation of serum K represents only that portion of K in the body ( 2 %), not total body K • Occurrence of hyperkalemia or hypokalemia dose not mean increase or decrease of total body potassium; potassium depletion can occur despite hyperkalemia ( DKA)

Distribution of potassium • Intracellular storage of potassium buffers the ECF potassium concentration until relatively sluggish renal mechanisms excrete K load, usually requires 68 hours. ECF potassium is 56 m. Eq in 70 kg man, compared to total body potassium of 4200 m. Eq
; there")
Routes of K excretion • Fixed routes; ▫ Sweat ( 2 % ); there is 200 ml of sweat per day total K+ losses about 2 m. Eq/ day ▫ Stool ( 10 % ); 10 m. Eq/ day is lost through feces, during diarrhea episodes this route losses increase significantly, and can be increased in chronic renal failure, when it may account for up to 50% of potassium intake

Routes of K excretion • Variable route; ▫ Renal K excretion; major route account for 78% of potassium excretion per day in normal individuals, 60 -80 m. Eq/ day ▫ GFR of 150 L per day, 600 m. Eq of potassium are filtered, only 60 -80 m. Eq on average excreted in urine, so 85% of filtered potassium is reabsorbed

Potassium renal excretion • The kidney is primarily responsible for potassium regulation. In health, the kidney can lower renal excretion to 10 mmol per day or increase excretion to 400 mmol per day depending upon potassium intake. • The majority of the filtered K ( 600 mmol) is reabsorbed in the proximal tubule and loop of Henle. The control of potassium secretion occurs primarily in the principal cells of the cortical collecting tubule (CCT)

Potassium renal excretion • Potassium secretion is dependent on the delivery of sodium and water to the CCT and on the action of the hormone aldosterone. • Aldosterone increases sodium reabsorption from the lumen and promotes potassium secretion into the lumen, restoring electrical neutrality.
 • Increased: ▫ Aldosterone ▫ Increased")
Factors influenced renal K excretion ( external balance) • Increased: ▫ Aldosterone ▫ Increased sodium delivery to distal nephron; �Diuretics �Osmotic diuresis �Saline infusion ▫ Presence of poorly reabsorbed anion ( HCO 3) • Decreased: ▫ Non-anion gap acidemia
 Increase intracellular K; activating pump")
Regulators of K internal balance ( Na/K- ATPase pump) Increase intracellular K; activating pump Decrease intracellular K; inhibiting pump Insulin B 2 adrenergic agonist aldosterone Alpha adrenergic agonist Normal anion gap acidemia

Hypokalemia Mohamed Osama Ezwaie, MD

Hypokalemia; etiology Hypokalemia Drugs: diuretics, gentamicin, amphotericin, carbenoxolone, insulin, laxatives, acetazolamide, fludrocortisone Redistribution ( potassium shift into cells) Insulin adminstration prior to blood withdrwal Alkalemia B 2 – adrenergic stimulation Theophyllin toxicity Hypokalemic periodic paralysis ( familial, or thyrotoxicosis) B 12 therapy Extra-renal losses ( urine potassium < 20 m. Eq/ 24 hours) Diarrhea, vomiting Laxatives Villous adenoma Intestinal obstruction Hypokalemia Renal losses ( urine potassium > 20 m. Eq/ 24 hours) With acidosis Renal tubular acidosis Diabetic ketoacidosis Carbonic anhydrase inhibitors Ureterosigmoidostmy With alkalosis Diuretic therapy Conn’s syndrome Gitelman’s syndrome Bartter’s syndrome

While drugs such as potassium sparing diuretics, ACEIs, ARBs, and NSAID; increase serum potassium

Diagnosis hypokalemia • History; renal or extra-renal losses, diabetes mellitus, thyroid disease, family history, drug history. • O/E; body weight, pulse, HTN, respiratory pattern • Investigations; WBC, ABG, anion gap, urine potassium excretion per 24 hours, TTKG

Laboratory data: 1 - TFT 2 - ABG, FBG, s. Mg+2 3 - Urine K & Cl 4 - PRA & Aldosterone 5 - TTKG Hypokalemia; diagnostic approach
 • The transtubular potassium gradient (TTKG) is a formula")
Transtubular K gradient ( TTKG) • The transtubular potassium gradient (TTKG) is a formula used to assess renal handling of potassium ( aldosterone activity/ effect on late DCT & CCD). • Normally; hyperkalemia stimulates aldosterone release, hypokalemia the reverse TTKG = (urine k/serum k)/(urine osm/serum osm) Multiply by 100 for percentage � In the presence of hyperkalemia the ratio should be > 10 (if <10 means aldosterone deficiency ) � In the presence of hypokalemia the ratio of < 4 (if >4 means hyperaldosteronism)
 Gastrointestinal manifestations (")
Hypokalemia Clinical consequences Neuromuscular manifestations; weakness, fatigue, respiratory muscle dysfunction, rhabdomyolysis) Gastrointestinal manifestations ( constipation, ileus) Nephrogenic diabetes insipidus ECG changes; prominent U wave, T wave fattening cardiac arrhythrmias

Hypokalemia; management • Does the patient have an abnormal venous bicarbonate level indicating a metabolic acidosis or alkalosis? • Consider the degree of potassium deficit and ongoing potassium losses from gastrointestinal tract or kidneys. • Check the serum magnesium level in complicated patients or in those with severe hypokalaemia, as hypokalaemia will not respond to replacement therapy if the patient is hypomagnesaemic.
 and hypo/hypervolaemia •")
Treatment of hypokalemia • Look for evidence of arrhythmias (check ECG) and hypo/hypervolaemia • Oral Kcl replacement preferred to intravenous, unless there is profound hypokalemia ( < 3. 0 m. Eq/ L, or prolongation of PR interval) • Dietary potassium almost coupled to phosphate, rather to chloride, not effective in correcting potassium losses associated with chloride as in diuretic or vomiting states • In case of hypokalemia associated with acidosis, K Hco 3 salt is used to both conditions, as in diarrhea

Treatment of hypokalemia • Infusion of Kcl should not exceed 10 m. Eq/ hour, risk of acute hyperkalemia and phlebitis. If higher rates needed to be given through CV line, with cardiac monitoring • Avoid glucose containing solutions ( insulin release) to prevent further shift of potassium into cells • Magnesium deficiency should be corrected if refractory hypokalemia
 it may be")
Hypokalemia; Emergency treatment • If hypokalaemia is severe (<3. 0 mmol/L) it may be associated with muscle weakness leading to ventilatory failure or cardiac arrhythmias. • Intravenous replacement is appropriate in this setting • Never give ampoules of KCl directly without diluting • For patient safety max. potassium replacement should not exceed 100 m. Eq/ day, or even lower if there is oliguria, or renal dysfunction

Hyperkalemia Mohamed Osama Ezwaie, MD
 Marked leuckocytosis ( >100000/ mm), sever thrombocytosis, hemolysis, tumor lysis syndrome,")
Hyperkalemia Spurious (pseudohyperkalemia) Marked leuckocytosis ( >100000/ mm), sever thrombocytosis, hemolysis, tumor lysis syndrome, rhabdomyolysis Redistribution ( potassium shift out cells) Acidemia Hyperkalemic periodic paralysis B 2 adrenergic blockers miscellaneous Renal failure Aldosterone deficiency Drugs; ACEI, ARBS, cyclosporine, Spironolactone

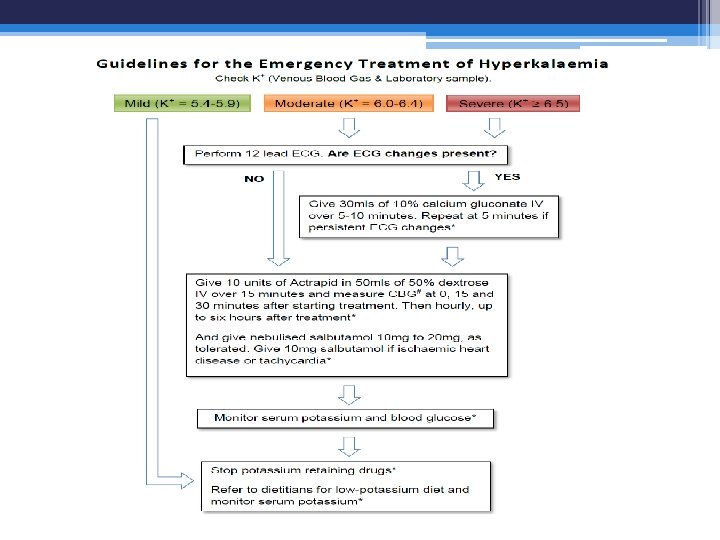
Mild: 5. 5 -6. 0 Moderate: 6. 0 -6. 5 Sever: >6. 5

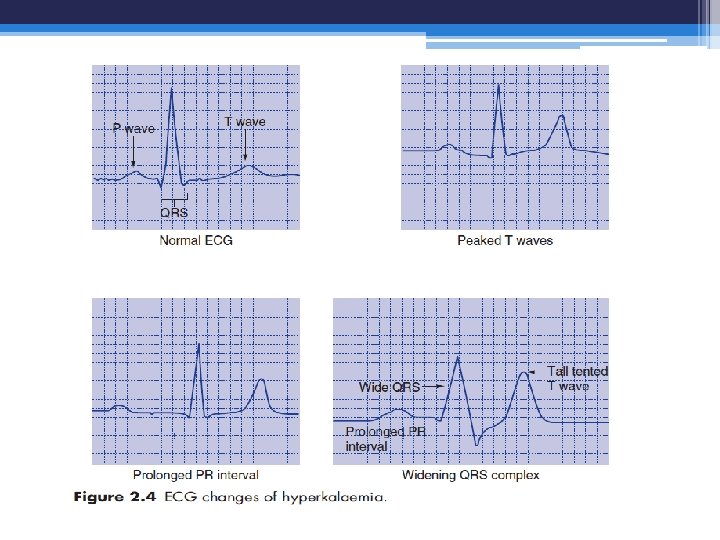
Hyperkalemia Clinical consequences Usually occur when potassium conc. > 6. 5 m. Eq/ L, Neuromuscular; weakness, ascending paralysis, and respiratory failure progressive ECG changes; peaked T Wave, fattened P wave, prologned PR interval, idioventricular rhythm, and widened QRS complex, and deep S wave, followed by ventricular fibrittation. These cardiac changes may occur suddenly without warning

Laboratory data: 1 - CBC 2 - ABG, FBG, RFT 3 - Urine Kl 4 - PRA & Aldosterone 5 - TTKG Hyperkalemia; diagnostic approach

Therapy of hyperkalemia • Therapy is directed in three ways: ▫ Emergency treatment; to counteract the cardiac effects of hyperkalemia, when advanced ECG changes are present. This is done by calcium gluconate infusion. ▫ Temporizing treatment: to acutely drive potassium into cells glucose plus insulin; B 2 agonists if no ischemic cardiac disease; bicarbonate if acidosis is present. ▫ Chelating therapy; to remove potassium from the body, sodium polystyrene sulfonate or dialysis

Emergency diagnosis and treatement of hyperkalemia • Remember may more than cause of your patient hyperkalemia, and impaired renal potassium excretion usually present • step 1. stop all adminstration of potassium ( oral, entral or I. V) • step 2. obtain stat ECG ( peaked T wave confirm that true hyperkalemia is present), more sever ECG manifestation of hyperkalemia indicate emergency therapy with IV infusion of calcium, to counteract the cardiac effect of hyperkalemia

Emergency diagnosis and treatment of hyperkalemia • Step 3. quickly seek possible hidden source of potassium; hemolysis, GIT hemorrhage, rhabdomyolysis, burns, drugs. • Step 4. temporizing or chelating treatment • Step 5. find underlying cause of hyperkalemia ▫ ▫ Pseudohyperkalemia Is sample hemolysed Is redistribution hyperkalemia present ( H/O) Look for miscellaneous causes; renal failure, addrenal insufficiency

Hyperkalemia; Emergency treatment • Shift potassium into cells by giving insulin and dextrose (10 units fast-acting insulin ( actrapid) and 50 m. L 50% dextrose) over 15 min. • Commence an insulin and dextrose infusion, with monitoring of capillary glucose levels at 1530 minutes intervals

Hyperkalemia; Emergency treatment • If the patient is acidotic and not in pulmonary oedema, consider giving sodium bicarbonate (500 m. L 1. 4%Na. HCO 3 over 1 -2 hours) • Note that 8. 4% Na. HCO 3 is hypertonic and should not be given peripherally • B 2 agonists such as salbutamol will also shift potassium into cells, but may exacerbate cardiac instability and are usually used in children.

Hyperkalemia; non-urgent manangement • Any underlying causes should be diagnosed and treated: ▫ Offending drugs discontinued ▫ Low potassium diet considered (CKD) ▫ Metabolic acidosis • Fludrocortisone may be useful in the setting of hypoaldosteronism.

Hyperkalemia; non-urgent manangement • Increased renal potassium elimination may be achieved by ▫ volume expansion with normal saline ▫ Judicious use of loop diuretics to improve the distal delivery of sodium and water.

Long-term therapy with cation exchange resins should be avoided as there is a risk of forming concretions in the bowel.

Simon Steddon, Neil Ashman. Handbook of nephrology and hypertension, 2 nd edition, 2014, oxford university press. Maxime papadakis, Stephen Mcphee. Current medical diagnosis and treatment. 55 th edition, 2016, Mc. Graw Hill. Brian Walker, Nicki Colledge, et al. Davidson’s principles and practice of medicine. , . 22 nd edition, 2014. Churchill Livingstone Elsevier Parveen Kumar, Michael Clark. Kumar and Clark’s clinical medicine, 8 th edition, 2012. Saunders Elsevier press.
- Slides: 42