Postpartum hemorrhage Postpartum hemorrhage Blood loss 500 ml

Postpartum hemorrhage

Postpartum hemorrhage • Blood loss • > 500 ml for vaginal delivery • >1000 ml for caesarean section (Pritchard et al, 1962) (WHO) • After completion of the third stage of labor • Inaccurate estimated blood loss, underreporting Michael A Belfort, MBBCH, MD, Ph. D, FRCSC, FRCOG. Overview of postpartum hemorrhage.
 • Need for")
Postpartum hemorrhage • >10% change in hematocrit (Combs et al, 1991) • Need for blood transfusion (Combs et al, 1991) • Excessive bleeding that makes the patient symptomatic • Potential to produce hemodynamic instability (>10% of total blood volume) Michael A Belfort, MBBCH, MD, Ph. D, FRCSC, FRCOG. Overview of postpartum hemorrhage.

Symptom related to blood loss with postpartum hemorrhage

Postpartum hemorrhage • Primary PPH – 4– 6% of pregnancies – Occurring within first 24 hours of delivery • Secondary PPH – Occurring between 24 hours and 6– 12 weeks postpartum Michael A Belfort, MBBCH, MD, Ph. D, FRCSC, FRCOG. Overview of postpartum hemorrhage ACOG Practice Bulletin No. 76: Postpartum Hemorrhage. Obstet 5 Gynecol. 2006 ; 108(4): 1039 -47

80% or more of cases 6
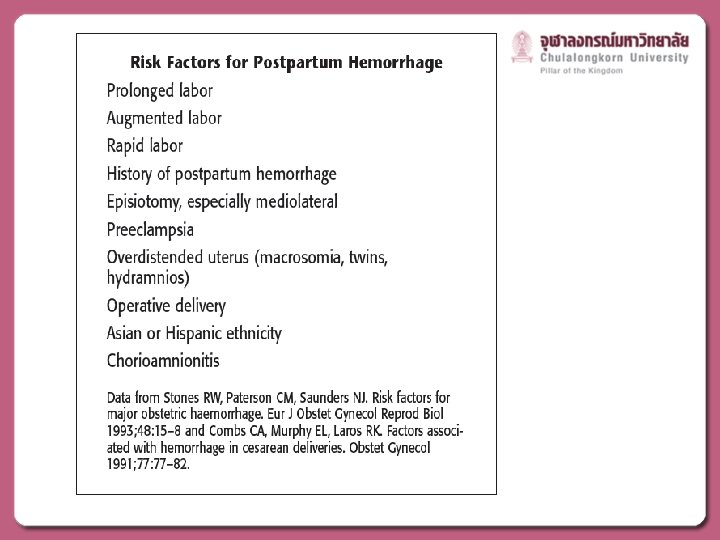

Etiology of PPH • • • Overdistension of uterus Uterine muscle exhaustion Intra-amniotic infection Anatomic distortion of uterus Uterine-relaxing medications Bladder distension • Lacerations of the cervix, vagina, perineum • Extensions, lacerations at cesarean section • Uterine rupture • Uterine inversion 8 • Retained products of conception • Retained blood clots Tone Trauma Tissue • Hereditary coagulopathies or Throm liver disease bin • Acquired in pregnancy • HEELP syndrome • DFIU • Amniotic fluid embolus SOGC clinical practice guideline : Active management of the third stage of labour: prevention and treatment of postpartum hemorrhage. JOCG. 2009; 235: 980 -93.

MANAGEMENT

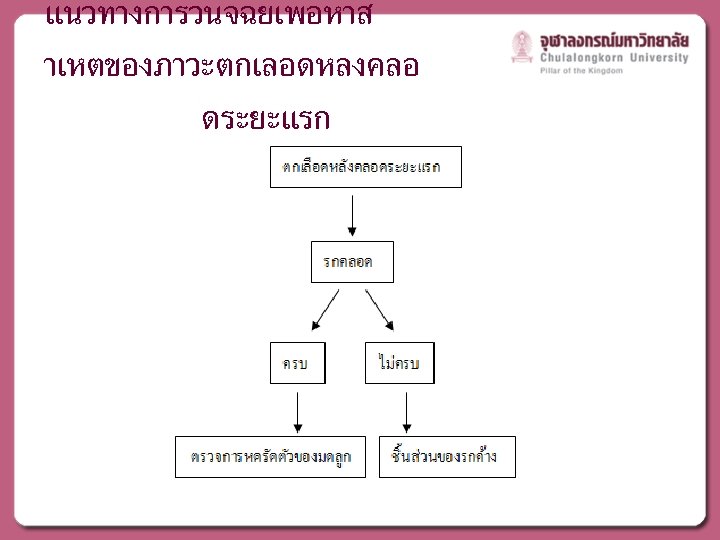
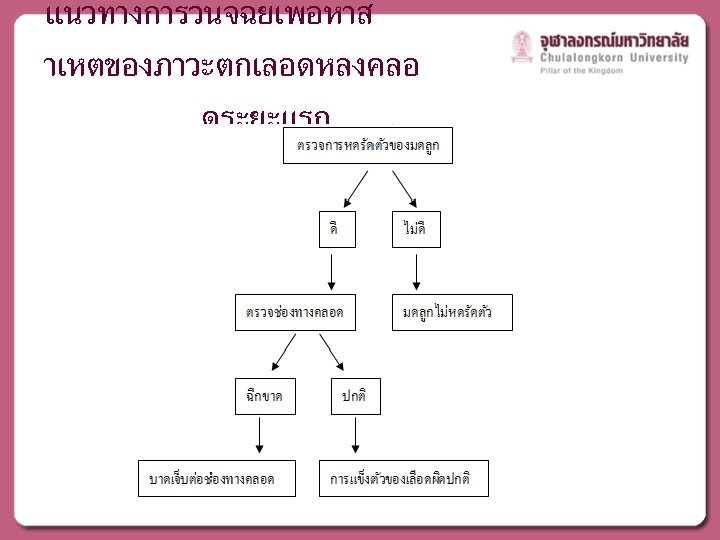
Step 1 Initial Assessment and treatment Resuscitation - Call for help Large bore IV ABC O 2 supplement Vital sign, I/O Foley catheter Assess Etiology Laboratory test - Explore uterus (tone, tissue) - Explore LGT (trauma) - Review Hx (thrombin) - Observed bleeding - CBC - Coagulation - Group and cross Step 2 : Directed Therapy Tone - Massage - Uterotonic Drugs Tissue Trauma Thrombin - Manual removal - Curettage - Correct inversion - Anticoagulation - Replace factor - Repair laceration - Repair hematoma Adapted from : WHO guidelines for the management of postpartum haemorrhage and retained placenta, 2009.

Step 3 : Intractable PPH Get Help - Large bore iv - Anesthesiologist - Lab and ICU Local Control - Manual compression +/- pack uterus +/- uterine tamponade +/- embolization BP & Coagulation - Crystalloid - Blood product Step 4 : Surgery Repair laceration Ligate vessels - Uterine/ ovarian vessel - Internal iliac artery Hysterectomy Step 5 : Post Hysterectomy Bleeding Abdominal packing Angiographic Embolization Adapted from : WHO guidelines for the management of postpartum haemorrhage and retained placenta, 2009.

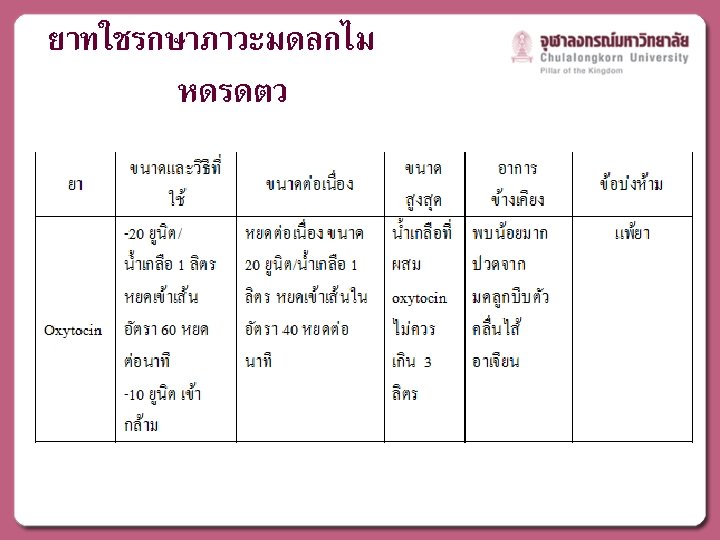
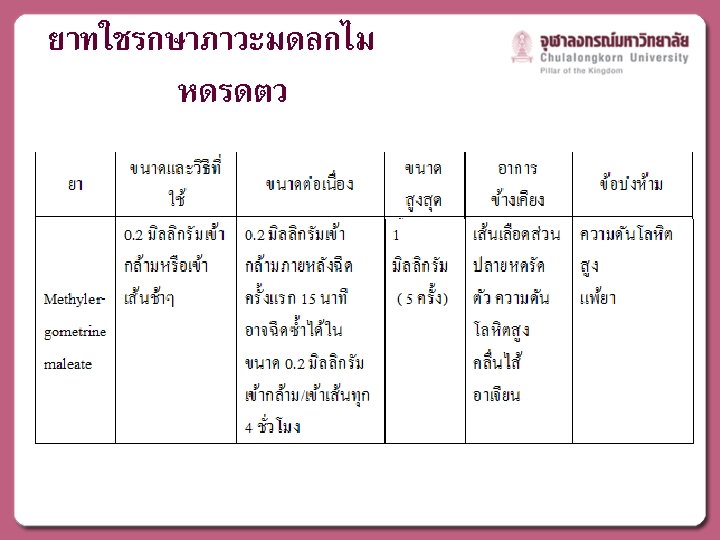
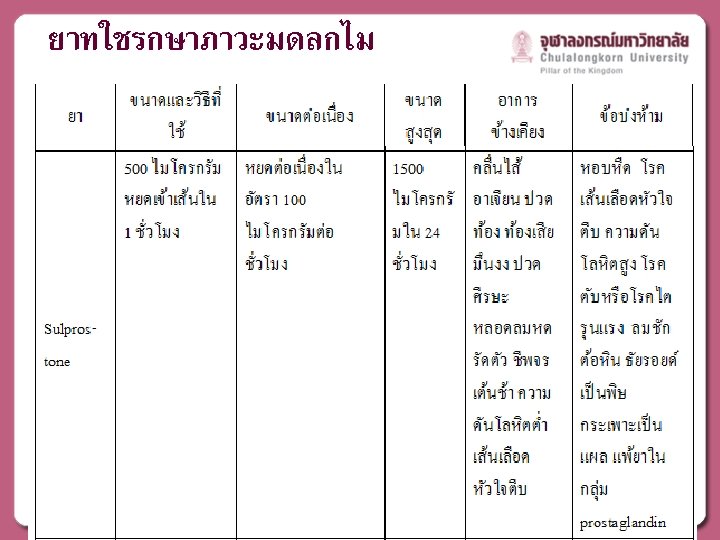
MEDICAL MANAGEMENT
: 1039 -47")
ACOG Practice Bulletin No. 76: Postpartum Hemorrhage. Obstet Gynecol. 2006 ; 108(4): 1039 -47

17 RTCOG Guideline October 2011. Management of atonic postpartum hemorrhage

18 RTCOG Guideline October 2011. Management of atonic postpartum hemorrhage


Bimanual uterine compression

Compression of abdominal aorta

TAMPONADE AND SURGICAL MANAGEMENT

Uterine tamponade Temporarily control active PPH due to uterine atony which not responded to medical treatment ACOG Practice Bulletin No. 76: Postpartum Hemorrhage. Obstet Gynecol. 2006 ; 108(4): 1039 -47

Tamponade balloon

Bakri Balloon Tamponade ใสนำได 300 -500 มลลลต

Surgical Management

B-lynch Technique Compression suture

B-lynch Technique Compression suture

Cho technique Compression suture

Uterine artery ligation

Umbrella packing

Uterine artery embolization

BIRTH CANAL LACERATION

Birth canal laceration • Perineal tear • Vaginal tear • Cervical tear

Perineal tear repair • Principle : ensure that first stitch suture inserted above apex of the tear or episiotomy wound • Continous polyglactin/ polyglycolic acid suture on tapercut needle • Obliterated dead space and taking care that sutures not too tightly • If dead spaces cannot be closed securely : Vg packing B-Lynch C et al. A textbook of postpartum hemorrhage: bleeding from the lower genital tract. Sapiens Publishing, 2006.

Vaginal tear repair Ø Superficial tear : similar to perineal tear Ø Deeper tear : • Identified bleeding vessel and ligated it • Any significant dead space or tear too friable to accept suturing >> packing • Repaired should be done under adequate anesthesia B-Lynch C et al. A textbook of postpartum hemorrhage: bleeding from the lower genital tract. Sapiens Publishing, 2006.

Vaginal tear repair Ø Vaginal packing using gauze : common method to achieve temponade Ø Vaginal packing with thrombinsoaked pack : closure of all laceration has not been possible Ø Risk of raw surface will rebleeding when removed packing : using sterile plastic bag inserted with providoneiodine-soaked pack Ø Left packing for 24 -36 hr with retained Foley’s catheter and ATB prophylaxis B-Lynch C et al. A textbook of postpartum hemorrhage: bleeding from the lower genital tract. Sapiens Publishing, 2006.

Cervical tear • Superficial lacerations of the cervix can be seen on close inspection in more than half of all vaginal deliveries. • Most of these are less than 0. 5 cm and seldom require repair (Fahmy, 1991). • Deeper lacerations are less frequent, but even these may be unnoticed. • Due to ascertainment bias, variable incidences are described. Williams Obstetrics, 24 th Edition - Cunningham, Leveno, Bloom et al

Cervical tear • not usually problematic unless – hemorrhage – extend to the upper third of the vagina. • Rarely, the cervix may be entirely or partially avulsed from the vagina —colporrhexis—in the anterior, posterior, or lateral fornices. • sometimes follow – difficult forceps rotations – forceps blades applied over the cervix. Williams Obstetrics, 24 th Edition - Cunningham, Leveno, Bloom et al

Cervical tear • In some women, cervical tears reach into lower uterine segment and involve the uterine artery and its major branches. • They occasionally extend into the peritoneal cavity. • The more severe lacerations usually manifest as external hemorrhage or as a hematoma, however, they may occasionally be unsuspected. Williams Obstetrics, 24 th Edition - Cunningham, Leveno, Bloom et al

Cervical tear Melamed N et al. Intrapartum cervical lacerations: characteristics, risk factors, and effects on subsequent pregnancies. AJOG. 2009 ; 200: 388 e 1 -4.

Cervical tear repair Ø Laparotomy : tear extending above internal os Ø Packing with pressure : small, or non bleeding laceration Ø Cervical tear with active bleeding or longer than 2 cm may be repaired Ø Absorbable suture material

• Gasp edges of most caudal part of laceration with ring forceps B-Lynch C et al. A textbook of postpartum hemorrhage: bleeding from the lower genital tract. Sapiens Publishing, 2006.

• Suture with interrupted or figure of eight stitch • Held with hemostat to bring down into view next part to repair B-Lynch C et al. A textbook of postpartum hemorrhage: bleeding from the lower genital tract. Sapiens Publishing, 2006.

• Suture to the apex of the laceration • Observed of laceration for a few minutes to ensure secure hemostasis B-Lynch C et al. A textbook of postpartum hemorrhage: bleeding from the lower genital tract. Sapiens Publishing, 2006.

Prevention of PPH • Active management of third stage of labor – Assisted expulsion of placenta – Prevent of decrease blood loss Uterotonic drugs Umbilical cord clamping Controlled cord traction 49 SOGC clinical practice guideline : Active management of the third stage of labour: prevention and treatment of postpartum hemorrhage. JOCG. 2009; 235: 980 -93.

Active management of 3 rd stage of labor The Cochrane Review concluded that active management reduced risks of the following v maternal blood loss v postpartum hemorrhage exceeding 500 m. L v prolonged third stage labor

Active management of 3 rd stage of labor • Active management of third stage of labor for all vaginal births including –routine administration of oxytocin with shoulder delivery –cord traction –uterine massage. (I-A) SOGC Clinical practice guideline. Active management of the third stage of labor : prevention and treatment of postpartum hemorrhage. October 2009.
 IM is")
Active management of 3 rd stage of labor • Oxytocin (10 IU) IM is the preferred medication and route for the prevention of PPH in low-risk vaginal deliveries. (I-A) • Care providers should administer this medication after delivery of the anterior shoulder. (I-A) SOGC Clinical practice guideline. Active management of the third stage of labor : prevention and treatment of postpartum hemorrhage. October 2009.

Active management of 3 rd stage of labor • Intravenous infusion of oxytocin (20 to 40 IU in 1000 m. L, 150 m. L per hour) is an acceptable alternative for AMTSL. (I-B) SOGC Clinical practice guideline. Active management of the third stage of labor : prevention and treatment of postpartum hemorrhage. October 2009.

Active management of 3 rd stage of labor • An IV bolus of oxytocin, 5 to 10 IU (given over 1 to 2 minutes), can be used for PPH prevention after vaginal birth but is not recommended at this time with elective Caesarean section. (II-B) SOGC Clinical practice guideline. Active management of the third stage of labor : prevention and treatment of postpartum hemorrhage. October 2009.

Active management of 3 rd stage of labor • Ergonovine can be used for prevention of PPH but may be considered second choice to oxytocin – greater risk of maternal adverse effects – need for manual removal of a retained placenta. • Ergonovine is contraindicated in patients with hypertension. (I-A) SOGC Clinical practice guideline. Active management of the third stage of labor : prevention and treatment of postpartum hemorrhage. October 2009.

Active management of 3 rd stage of labor • Active management of third stage of labor – Carbetocin : long-acting oxytocin 56 • 100 mcg IV bolus over 1 minute should be used instead of continuous oxytocin infusion in elective caesarean section to decrease the need for therapeutic uterotonic (I-B) • 100 mcg IM decreases the need for uterine massage for women compared with continuous infusion of oxytocin in woman who delivering vaginally with 1 risk factor for PPH (I-B) SOGC clinical practice guideline : Active management of the third stage of labour: prevention and treatment of postpartum hemorrhage. JOCG. 2009; 235: 980 -93.

Active management of 3 rd stage of labor • Late cord clamping (performed after 1 to 3 minutes after birth) is recommended for all births while initiating simultaneous essential newborn care. • Early cord clamping (<1 minute after birth) is not recommended unless the neonate is asphyxiated and needs to be moved immediately for resuscitation. WHO recommendations for the prevention and treatment of postpartum haemorrhage 2012
 is")
Active management of 3 rd stage of labor • Oxytocin (IV or IM) is the recommended uterotonic drug for the prevention of PPH in caesarean section. (Strong recommendation, moderate-quality evidence) WHO recommendations for the prevention and treatment of postpartum haemorrhage 2012

Thank you

Late PPH
- Slides: 60