POSTPARTUM HAEMORRHAGE u With Mother Mortality Ratio of




 Secondary (b/w 24")
 Tone— Tissue— Trauma--Trombin--- .")
 Chorio amnionitis,")

 SYM &SIGNS DEGREE OF SHOCK 5001000 ml(1015%) NORMAL PALPITATION,")
 should be transferred to centres where")
 Active management of 3 rd stage.")




- Slides: 16
POSTPARTUM HAEMORRHAGE
u With Mother Mortality Ratio of 276 per 100, 000 live births, the country has slipped from 147 to 149 th position, says report u Published in Dawn, May 6 th, 2015
POSTPARTUM HAEMORRHAGE u INTRODUCTION: Most commom cause of maternal mortality. In developed counteries----MMR-7 -10/100, 000 livebirths, acc to National statistics, 8% of deaths due to PPH In developing counteries----MMR >1000/100, 000 livebirth, acc to WHO statistics, 25% of deaths due to PPH
PPH u DEFINATION: Blood loss in excess of 500 ml following a vaginal birth or a loss of greater than 1000 ml following c/section. OR Any blood loss that causes a major physiological change (e. g a fall in b. p)
PPH u TYPES: Primary (in 1 st 24 hrs after delivery) Secondary (b/w 24 hrs & 6 -12 weeks postpartum)
PPH u AETIOLOGY: ( 4 Ts) Tone— Tissue— Trauma--Trombin--- .
PPH u RISK FACTORS: Overdistended uterus(multiple pregnancy , polyhydramnios, fetal macrosomia, ) Chorio amnionitis, Prolonged ROM, Prev c/section, APH, Induction of labour , Prolonged labour, Instrumental delivery , Prev H/O PPH , Coagulation disorders.
PPH u PATHOPHYSIOLOGY: al sutures or living ligatures Physiologic
BLOOD BP VOLUME LOSS (Systolic) SYM &SIGNS DEGREE OF SHOCK 5001000 ml(1015%) NORMAL PALPITATION, TACHYCARDIA, DIZZINESS COMPENSATE D 10001500 ml(1525%) SLIGHT FALL 80100 mm. Hg WEAKNESS, TACHYCARDIA, SWEATING MILD 15002000 ml(2535%) MODERATE FALL 7080 mm. Hg RESTLESSNESS, MODERATE PALLOR, OLIGURIA 20003000 ml(3550%) MARKED FALL 5070 mm. Hg COLLAPSE, AIRHUNGER, ANURIA SEVERE
PPH u PREDICTION: Patients with identified risk factors(40%) should be transferred to centres where transfusion facilities & ICU available. Early & prophylactic interventional radiology for high risk. Introduction of strategies for PPH management.
PPH u PREVENTION: Antenatal assesment(anaemia, medical problems, ) Active management of 3 rd stage. (administration of uterotonic drugs, controlled cord traction, uterine massage after delivery of placenta) ACC TO 5 RCT + COCHRANE META ANALYSIS (>6000 WOMEN)----- 60% OF PPH ↓↓ BY ACTIVE MANAGEMENT
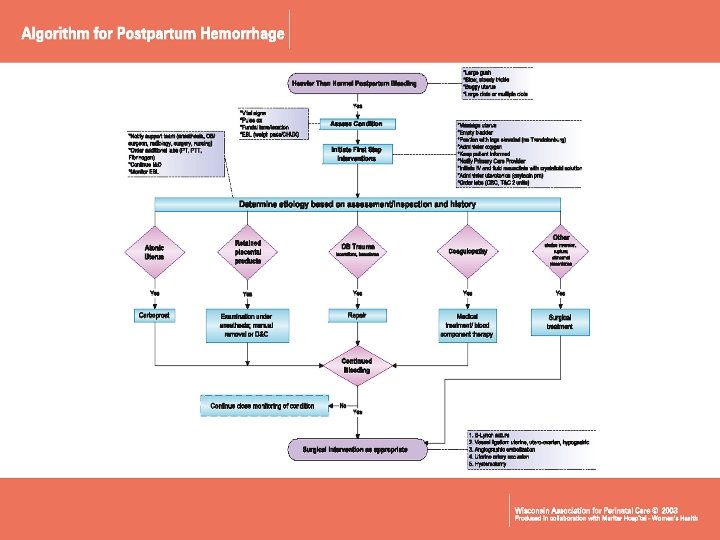
HAEMO STASIS Ø ALGORITHM GENERAL MEDICAL MANAGEMENT H---Ask for help A---Assess and Resuscitate E---Establish aetiolgy, ecbolic , ensure availability of blood M---Massage of uterus O---Oxytocin , prostaglandin Ø SPECIFIC SURGICAL MANAGEMENT ---Shift to operation theatre T---Tissue and trauma to be excluded & proceed to tamponade balloon A---Apply compression sutures ---Systemic pelvic devascularization --Interventional radiology uterine artery embolization S---Sub total and total abdominal hysterectomy S S I-
HAEMOSTASIS HELP: Multidisciplinary approach. u ASSESS: Level of consciousness , vital signs, u Investigations n blood for gp & cross match , fluid replacement(0. 9%N/Saline or Ringer lactate solution) u ESTABLISH: (etiology: 4 Ts) (ecbolics: oxytocin, ergometrine) (ensure availability of blood & blood products). MASSAGE: Uterine massage. u OXYTOCIN: OXYTOCIN, 10 units i/v bolus or 40 units u in 500 ml of 0. 9%N/Saline. ERGOMETRINE , PROSTAGLANDIN E 1 & E 2
HAEMOSTASIS u SHIFT: Theatre , anti shock garment, bimanual compression. TISSUE&TRAUMA : to be excluded n proceed to uterine u APPLY COMPRESSION SUTURES: u SYSTEMIC PELVIC DEVASCULARIZATION: u INTERVENTIONAL RADIOLOGY(Uterine artery embolization) Arterial embolisation under fluoroscopic u packing or tamponade with balloon(foley s catheter, other catheters) technique. B –Lynch suture Uterine , ovarian, internal iliac artery ligation. (40 -100% success rate) but expertise , hemodynamically stable pt required. guidance , prophylactic role in adherent placenta is there. u SUBTOTAL /TOTAL HYSTERECTOMY:
CONCLUSIONS u u IDENTIFICATION OF RISK FACTORS DURING ANTENATAL & LABOUR. PROMPT RESUSCITATION & RESTORATION OF BLOOD. MULTIDISCIPLINARY TEAM APPROACH. TREATMENT MEASURES IN STEP WISE(HAEMOSTASIS) RESULTED IN DECREASE IN MATERNAL MORBIDITY & MORTALITY DUE TO PPH