Postoperative complications associated with sinus floor elevation sinusitis
 2012. 06. 05")








 : 3")
 sinusitis only")









 1. Systemic antibiotic therapy.")

 <8명/198 명에서 graft infectin 나타남> 1. CT taking->consulte to")








- Slides: 33
Postoperative complications associated with sinus floor elevation (sinusitis, sinus graft infection) 2012. 06. 05 R 3 김혜미 KHU PERIO
Maxillary sinusitis introduction Sinus graft infection Conclusion CONTENS KHU PERIO
Complications associated with sinus floor elevation 1, 5 Operative complications Immediate postoperative complications Late postoperative complications üExcessive bleeding üSinus membrane perforation üInfection of the graft üSinus infections üAcute sinusitis üImplant failure üFlap dehiscence üOroantral fistula formation üChronic sinusitis üCyst formation üFormation of inadequate graft volume of implant placement Major postoperative complications after sinus elevation surgery are relatively uncommon. but if it happened, appropriate treatment is mandatory. KHU PERIO
The incidence of postoperative complications Timmenga et al. 1997 • Transient maxillary sinusitis : 4%, • Cronic maxillary sinusitis : 1. 3% Schwarz-Arad, Herberg, and Dolev (9) • Graft-induced sinusitis by perporation <1% (1/80) Manor, Mardinger, Bietlitum et al. (5) • The incidence of acute and chronic sinusitis <5% Urban, Nagursky, Church et al. (12) • Sinus graft infection : 4% (8/198명) The incidence of deveopment of maxillary sinusitis after an augmentation of the sinus floor : 0~20% (4), 0~27% (3), 3% (11) Graft infection : 2~5. 6% (1), 2~7% (13) KHU PERIO
Maxillary sinusitis introduction Maxillary Sinusitis • nondontogenic origin • odontogenic origin Sinusitis after sinus augmentation • symptoms • etiology • treatment CONTENS KHU PERIO
acute maxillary sinusitis : nonodontogenic source 1, 10, 15 Decongestants • systemic : Pseudoephedrine hydrochloride 30 mg*6 hours • localcases : 85~95% are viral origin, antibiotic therapy is not Oxymetazoline HCl (0. 05%) : 1 spray*12 H or indicated initially Phenylephrine HCl (0. 125, 1. 0 %)of: 2 -3 Symptoms (tissue edema, obstruction thespray ostia)*12 H Saline nasal mist humidified air Acute sinusitis Chronic sinusitis 4 wks 12 wks Subacute sinusitis Recurrent sinusitis KHU PERIO
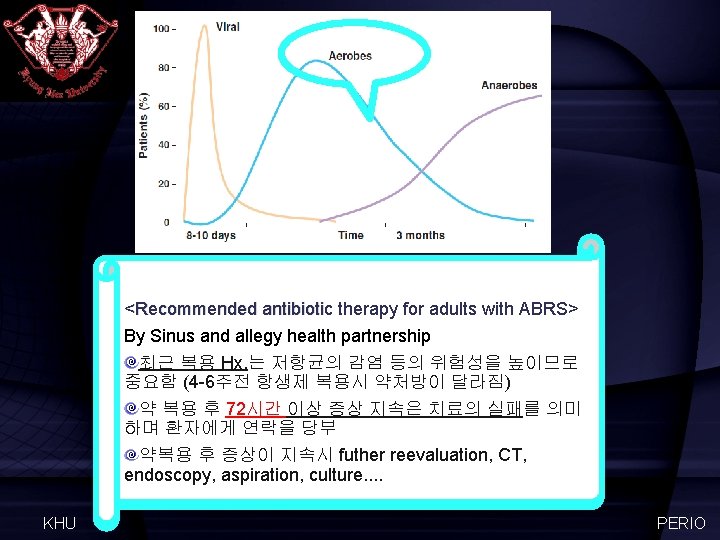
Recommended antibiotic therapy for adults with ABRS 2 2. 72시간 후 회복X 1. 약 처방 3. Alternatie antimicrobial 최근 복용 Hx. 유. 무 therapy Or reevaluation 1. First choice : Fluoroquiolone or 고용량의 augmentin KHU PERIO
Acute maxillary sinusitie : odontogenic source 7 치성 상악동염의 이환율은 10~12%<Maloney PL, Doku HC, 1968>, 38%ü<Abrahams JJ, Glassberg Rm, 1996> 상악동 안의 fluid가 1/3 이상 찬 경우!! Sinusitis of dental etiology is of particular interest because the pathophysiology, microbiology, and treatment differ from sinusitis caused by other conditions An anaerobic bacteria ↑ Periodontal üFluid가 1/3이상 + Mucosal disease thickening with a periapical abscess A projection premolar or molar tooth root that has periodontal disease Oroantral fistula üMucosal thickening이 심할 경우!! KHU 치성 상악동염 을 의심할 것!! PERIO
Maxillary sinusitis introduction Maxillary Sinusitis • nondontogenic origin • odontogenic origin Sinusitis after sinus augmentation • symptoms • etiology • treatment CONTENS KHU PERIO
maxillary sinusitis after sinus augmentation-symptoms A typical triad of symptoms (4, 5) : 3 -12 weeks after (14) • Nasal congestion or obstruction • Pathologic secretion • Headache + Pain or tenderness in the region of the sinus, in combination with mucopuluent rhinorrhea (10) 1 or more of the major factors KHU PERIO
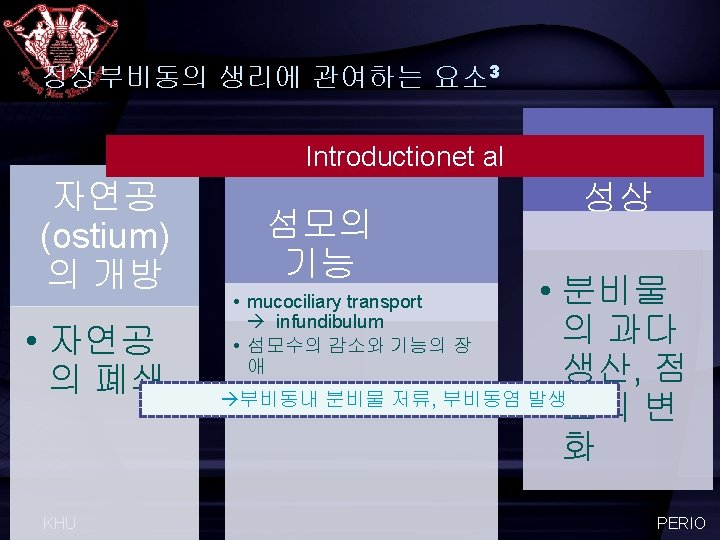
maxillary sinusitis after sinus augmentation-etiology 4 Pre-existing sinus disease Post-surgical complications Transient(acute) sinusitis only developed in patents with a predisposition for sinusitis. sinus drainage did not seem to be compromised in health persons after sinus floor augmentation, nor did accidental perforations of the mucous lining of the maxillary sinus result in sinusitis postsurgically. Sinus augmentation in patients without sinus problems and no radiographic evidence of pathologic disease does not induce a sinusitis attributable to reduced sinus drainage. (4) Large tears can cause sinusitis (3, 9). KHU PERIO
maxillary sinusitis after sinus augmentaiton-etiology 1, 3, 5, 6 Preoperative consideration A previously existing asymtomatic chronic sinus infection Postoperative sinus infections Communication (perporation) Ostial obstruction due to swelling, hematoma, seroma A lack of asepsis during the surgical procedure Bacteria from the oral cavity Bacteria originating from periapical or periodontal infections Intraoperative consideration KHU PERIO
maxillary sinusitis after sinus augmentaiton-treatment 4, 14 Infection may be limited to the maxillary sinus treated with floor elevation and grafing, but in may also diffuse to other paranasal cavities and, in the most severe cases, involve the orbital cavity and the anterior and middle cranial fossae. <Quiney et al. 1990, Tmmenga et al. 2001, Alkan et al. 2008, Li & Wang 2008> It is mandatoy to treat these complications as soon as possibe and following safe and reliable treatment protocol. Following sinus augmentation surgery, post-surgical complications or compromised results tend to be associated with pre-existing sinus disease Proper preoperative evaluation and treatment KHU PERIO
General guidelines for the treatment of transient and chronic maxillary sinusitis after augmentation of the maxillary sinus floor 3 Transient sinusitis • 1. Use of decongestants and antibiotics • 2. Follow-up after 2 weeks • 3. If no recovery, transient sinusitis was possibly evolvedfor into subacute <examples sinusitis aftersinusitis sinus augmentation> needing further treatment 3 • a. Contiunation of decongestants and antiviotics choicefor: tx. sinus irrigation 1. First consevative • b. Maxillary drains Fluoroquiolone • c. CT scanning and consideration of functional Amoxycillin-clavulanate 500/125 * 3 p. o * 2 wks + endoscopic sinus surgery if no recovery 3 daily (오트리빈 or 고용량의 xylomethaxoline 0. 1 % 4 g *within 3 times weeks ) augmentin Chronic sinusitis 2. 증상개선 없어 수술결정 (inferior meatal antrostomy, irrigation)+ culture 하여 약 처방 • Use of decongestants and antibiotics • CT scanning nad functional endoscopic sinus surgery KHU PERIO
General guidelines for the prevention of transient and chronic maxillary sinusitis after augmentation of the maxillary sinus floor 3, 6 The prevention of sinusitis(3) • Preoperative evaluation of sinus clearance-related factors • Postsurgery: a nasal decongestant (xylomethazoline 0. 05%) and topical corticosteroid (dexamethasone 0. 01%) to prevent postsurgery obstruction of the ostium • Perioperative antibiotic prophylaxis (cephradine 1 g*3 P. O, starting 1 hour before surgery and continued for 48 hours after surgery)) Conservative treatment of chronic sinusitis(6) • Decongestant nasal drops (xylomethazoline 0. 1%*tid*7~10 days) • An anti-inflammatory nasal spray (mometasone furoate monohydrate*bid*7~10 day) • In acute symptoms : systemic antibiotic tx. (amoxicillin 1 g*tid*7 days) Surgical therapy KHU • Cysts, ostium stenosis, septum deviation, recurrent chronic sinus infection • 수술 후 6개월 후에 상악동 증강술 시행 PERIO
Maxillary sinusitis introduction Sinus graft infection Diagnosis Etiology Prevention Treatment CONTENS KHU PERIO
Incidence & diagnosis of infected sinus grafts 1, 12 Sinus graft infection is a major but infrequent complication The incidence of deveopment of Graft infection after an augmentation of the sinus floor : 2~5. 6%(1), 2~7%(13), 4. 7%(Jensen SS. & Terheyden H. 2009) • Within 2 weeks • Late infections(1 -2 months) →sometimes time CT image Symptoms KHU • Black hole • Drainage tract • Tenderness • Pain • Recurrent facial swelling • Fistulation, purulent discharge • Popcorn sign + concomitant sinusitis (rare) PERIO
Sinus graft infection pre-existing sinus infection Salivary/bacterial contamination of the graft material, instruments, or membrane Infected simultaneous lateral ridge augmentation procedures Untreated periodontal disease Contamination of the surgical site Adjacent periapical pathology Lapses in the chain of sterility Etiology of infected sinus grafts 1 KHU Extended surgical time PERIO
The breakdown of primary soft-tissue closure Exposure of the barrier membrane Sinus graft infection pre-existing sinus infection Salivary/bacterial contamination of the graft material, instruments, or membrane Infected simultaneous lateral ridge augmentation procedures Untreated periodontal disease Localized endodontic and. Contamination periodontal therapy of the should be completed, & the hopelss teethsite should be surgical extracted. Simultaneous extraction of teeth that penetrate the sinus floor may open a pathway to infection as the sinus graft is immediately connected to the oral cavity through the extracion socket which may or may not be covered by flap release and primary closure. Adjacent periapical pathology Lapses in the chain of sterility Extended surgical time KHU PERIO
Prevention of sinus graft infections 1 Proper case selection. Use proper prophylactic antibiotics. (Augmentin, levofloxacin, moxifloxacin 추천, clindamycin 비추!!) Use chlorhexidine and/or betadine preparation of the mouth and face for surgery. Use sterile draping with an infection control protocol. Keep incision lines distant from window and barrier membrane. Prevent contamination of graft and barrier membrane with saliva. Ensure the sterility of all instruments being used. Keep the surgical time as short as possible. Use postoperative chlorhexidine rinses KHU PERIO
treatment of sinus graft infections Li & Wang, 2008 (11) 1. Systemic antibiotic therapy. 2. If infection persists for more than 4 wk, remove graft and re-graft at later time Urban et al. 2012 (12) KHU 1. CT taking->consulte to an otolaryngologist 2. Surgical intervention + systemic pharmacologic treatment PERIO
treatment of sinus graft infections 1 Treat early when infection suspected. Change the treatment if no response. 1. Reinstitute or change antibiotic therapy. 2. Insert drain with antibiotic therapy. 3. Surgical debridement with thorough flushing with sterile saline. Metronidazole with Augmentin or levaquin Complete debridement? Vs. Core debridement? Simultaneous regrafting? KHU PERIO
Urban et al. 2012 (12) <8명/198 명에서 graft infectin 나타남> 1. CT taking->consulte to an otolaryngologist 2. Surgical intervention + systemic pharmacologic treatment Core deb ridement R egraftin g. X KHU JOMI 2012; 47: 449 -457 PERIO
13 Septic theory : the presence of air bubbles within the graft confirms anaerobic bacterial activity 0. 5% metronidazole solution (3 ml는 상악동거상 후 세 척, 2 ml는 골이식재와 섞 음) 76. 8% homogeneous 23. 2% significantly homogeneous Postoperative edema X. . . KHU Implant dentistry 2008; 157(3): 257 -263 PERIO
Cyst formation 9 KHU PERIO
Maxillary sinusitis introduction Sinus graft infection Conclusion CONTENS KHU PERIO
perforation Sinus graft infections sinusitis Sinus membrane KHU PERIO
Sinusitis, sinus infection Time After 2 wks, 3 -12 wks Sinus graft infection Within 2 wks Ct image Symptoms Nasal congestion, obstruction fistulation Treatment 1. Conservative tx. (augmentin + 1. Conservative tx. (metronidazole+augmentin) 2. Drainage 3. Surgical debridement decongestant). Water’s view 2. Reevaluation, ct taking, refer KHU PERIO
reference 1. 2. 3. 4. 5. 6. 7. 8. KHU Stephen S. And Wallace. Dental Implant Complications: Etiology, Prevention, and Treatment. Chapter 16. Complication in lateral window sinus elevation surgery Sinus and allergy health partnership. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngology–Head and Neck Surgery 2004; 130(1): 1 -45 Timmenga et al. Maxillary sinusitis after augmentation of the maxillary sinus floor: A report of 2 cases. J Oral Maxillofac Surg 2001; 59: 200 -204 Timmenga, Raghoebar, Boering et al. Maxillary sinus function aftersinus lifts for the insertion of dental implants. J Oral Maxillofac Surg 1997; 55: 936 -939. Manor, Mardinger, Bietlitum et al. Late signs and symptoms of maxillary sinusitis after sinus augmentation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010; 110: e 1 -e 4 Beaumont, Zafiropoulos, Rohmann , and Tatakis. Prevalence fo maxillary sinus disease and abnormalities in patients scheduledfor sinus lift procedures. J Peridontol 2005; 76: 461 -467. Bomeli, Branstetter, Ferguson. Frequency of a dental source for acute maxillary sinusiis. Laryngoscope; 2009: 580 -584 Lopatin, Sysolyatin and Melnikov. Chronic maxillary sinusitis of dental origin: Is external surgical approach mandatory? Laryngoscope 2002; 112: 1056 -1059 PERIO
9. 10. 11. 12. 13. 14. 15. 16. KHU Schwartz-Arad, Ran Herzberg, and Dolev. The prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. J periodontol 2004; 75: 511 -516 Kretzschmar, Salem et al. Rhinisinusitis: Review from a dental perspective. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003; 96: 128 -35 Li and Wang. Common implant-related advanced bone grafting complications: Classification, Etiology, and management. Implant Dent 2008; 17: 389 -401 Urban, Nagursky, Church et al. Incidence, Diagnosis, and treatment of sinus graft infection after sinus floor elevation: A clinical study. Int J Oral Maxillofac Implants 2012; 27: 449 -457 Joseph Choukroun, Alain Simonpieri, Marco Del Corso et al. Controlling Systematic Perioperative Anaerobic Contamination During Sinus-Lift Procedures by Using Metronidazole: An Innovative Approach. Implant Dent 2008; 17: 257– 270 Chiapasco, Felisati, Zaniboni et al. The treatment of sinusitis following maxillary sinus grafting with the association of functional endoscopic sinus surgery (FESS) and an intra-oral approach. Clin. Oral Impl. Res. 2012; 1 -7 Itzhak Brook. Sinusitis. Periodontology 2000; 49: 126 -139 Marple, Rberts, jennifer et al. Azithromycin extended release vs amoxicillin/clavulante: symptom resolution in acute sinusitis. American J of Otolaryngology-Head and Neak Medicine and Surgery 2010; 31: 1 -8 PERIO
KHU PERIO