Postnatal treatment and longterm outcomes of spina bifida

Postnatal treatment and long-term outcomes of spina bifida. What should we tell parents about current treatments? Ryan Waters Consultant Paediatric Neurosurgeon Wessex Neurological Centre

What do we mean ? ‘Open’ myelomeningocoele

What do we mean? ‘Closed’ defect - meningocoele Other spinal dysraphism
 Chiari II • • • Caudal")
What do we mean? Hydrocephalus – (why? ) Chiari II • • • Caudal displacement of cerebellar tonsils (&vermis) Caudal displacement of pons & medulla ‘kinking’ of the brainstem Tectal ‘beaking’ Aqueduct stenosis

What do we mean?

Why has it happened? Incidence: Worldwide 0. 17 -6. 39/1000 live births (Bowman et al. , Childs Nerv Sys 7, 2009) 0. 3/1000 live births (early 90’s), USA (reduced from 0. 6/1000 in early 80’s) Regional variation: UK slightly higher? (0. 7 -2. 5, Ireland 5 – but data from the 60’s)

Why is it less likely now? Folate supplements Prenatal diagnosis Other factors

Will it happen again? Recurrence risk with one affected child: 1 -2% ? (based on studies from 80’s & 90’s) Two affected children: rises to 10% Parent with spina bifida: 3%?

Will my baby survive? Historically poor outcome • • • Infection Hydrocephalus Brainstem dysfunction Between 1947 -1956: 89% died before the age of 6 months (UK)

Will my baby survive? Chicago; 118 patients, 20 -25 year follow up: (Bowman, Paediatr Neurosurg; 34; 2001) Mortality 24% (15% in first year) • • Hindbrain dysfunction Shunt malfunction

Why have things improved? Surgery • • Antibiotics ‘Selection’? No recent change in closure technique Introduction of ‘reliable’ shunting
 – no criteria which predict outcome 1970’s: Lorber criteria")
Should we treat everyone? (Yes) – no criteria which predict outcome 1970’s: Lorber criteria (for selection) • • Severe hydrocephalus Total paraplegia Kyphosis Additional birth defects Unselected group similar (mortality)

What problems will my child have? ‘Neurosurgical’ • • • Closure of defect Hydrocephalus Chiari II Intellect Ambulation Urinary/Bowel function Musculoskeletal

Three phases of Neurosurgery 1. Initial closure of myelomeningocoele 2. Asssessment and treatment of hydrocephalus (first 6 months) 3. Long-term management (shunt dysfunction, Chiari II, tethered cord, syringomyelia)
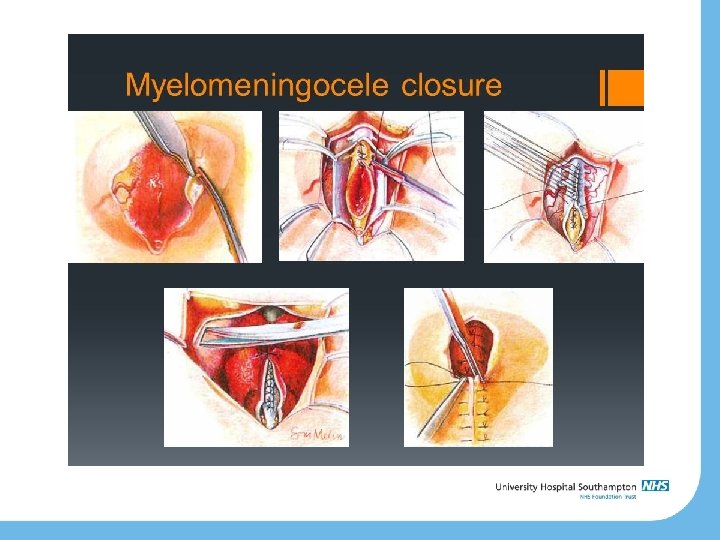

Closure Timing: within 72 hours of birth Keep exposed tissue moist Prophylactic antibiotics Assesment of hydrocephalus – may need shunt May need skin flap

Hydrocephalus May have signs prenatally/time of birth. Overt hydrocephalus at birth 15% (usually due to aqueduct stenosis) Develops days/weeks after birth: • • • Typical features CSF leak from wound Brainstem symptoms (Chiari? , but improve with shunt) – – – Stridor Poor swallow hypotonia

• Signs – Head circumference – Fontanelle – Sutures – Poor feeding/vomiting – Bradycardia/apnoeas – Squint – Sunsetting

Decision to shunt Increasing head circumference Increasing ventricular size on Cr. USS Symptomatic deterioration

VP shunt

Shunt

A shunt is for life…. . . Shunt insertion rate up to 90% (probably less now – 30% at SGH in last 3 years) Likely shunt-dependent Revision rate: • • • 30 -40% in first year 60% within 5 years 5% per year after first year

Valve technology
 Vs Silver Vs ‘Plain’")
Shunt Infection BASICS trial about to publish Catheter study: ‘Bactiseal’(clindamycin/rifampicin) Vs Silver Vs ‘Plain’ Infection rates

Will it affect intellect? 75% have IQ >80 ? effect of hydrocephalus 60% learning difficulties (evidence from 80’s & 90’s) Global cognitive problems Most are independent in ADLs (~80%) Employment - 30% in 1970 s (US), 60% in early 2000 s (Netherlands)

Shunts and intellectual function Effect on/of cortical mantle Stable mild to moderate ventriculomegaly; no effect Shunt infections; ventriculitis IQ 72 shunt/no ventriculitis no shunt IQ 95 IQ 102 (published 1982)

Ambulation

Ambulation 57% of 13 -27 yr olds used wheelchair Wheelchair use increases with age; 13 -17: 52% 18+: 63% (Johnson et al. , Am J Pub Health 2007; 97: 330 -336)

Urinary/Bowel continence Prevention of renal injury ‘Social’ continence Ensure ‘low pressure’ system; CIC, oxybutynin, antibiotic prophylaxis Detrusor/pelvic floor overactivity vs paralysis
 Constipation (Study")
Urinary/Bowel continence Most achieve ‘social’ urinary continence by school age (80 -85%) Constipation (Study of 125 Danish children, 2003) 10% suppositories 28% enemas 20% manual 24% >30 mins Incontinence 14% daily 14% weekly

How should baby arrive? Don’t ask the Neurosurgeon (But if you do: no evidence to clearly support caesarean vs vaginal delivery)

What about this new technique?

MOMS trial Multi-centre US study Open ‘in-utero’ closure vs. traditional closure Safe Improved functional outcome Reduced need for VP shunt

In-utero repair in UK Commissioned service at UCLH/Great Ormond Street Single centre for UK ? Other techniques: fetoscopic repair

Summary Likely to survive Degree of disability related to level and hydrocephalus Treatment of hydrocephalus is improving. . ? Multidisciplinary input

SGH experience 2015 -2017 2015 2 cases 1 shunt at time of repair (2 revisions) 2016 5 cases 1 shunt (6 revisions so far) 2017 3 cases 1 shunt (non-functioning)

Any questions? Mr Aabir Chakraborty Mr Ryan Waters Miss Salima Wahab Mr Nilesh Mundil
- Slides: 37