Post term Pregnancy DEFINITION n n n Postterm

 pregnancy refers to a pregnancy that")










- Slides: 14
Post term Pregnancy
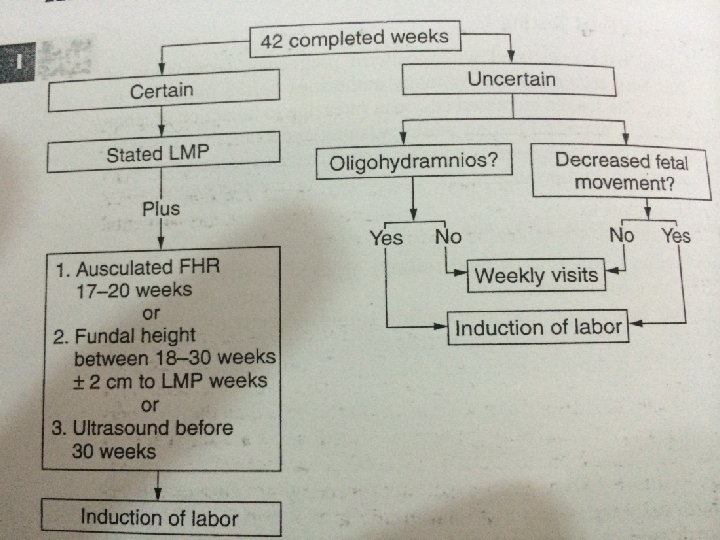
DEFINITION n n n Postterm” (also called prolonged) pregnancy refers to a pregnancy that has extended to or beyond a gestational age of 42. 0 weeks or 294 days from the first day of the last menstrual period Postmature used to describe infant with recognizable C/F indicating a pathologically prolonged pregnancy. We should avoid the term “post dates” pregnancy as it is loosely used and ill-defined
Causes of Postterm pregnancies n n By far, inaccurate dating is the most common etiology. So, get the dating correct! In the absence of inaccurate dating we do not yet understand why some pregnancies carry to 42+ gestational weeks although there is data to suggest genetics and paternity play an active role. Biological-previous prolonged preg. Decreased fetal estrogen production Placental sulfatase deficiency Anencephaly Fetal adrenal hypoplasi
Risk factor for PTP n Primiparup n Prior postterm pregnancy n n More rarely: fetal anencephaly and placental sulfatase deficiency MALE BABY
PHYSILOGICAL CHANGES ASS. WITH POSTTERM GESTATION l PLACENTAL CHANGES : ageing (increased grading on us ) infarcts , calcification AMNIOTIC FLUID CHANGES : Oligohydramnios (diminished fetal urination) presence of meconium l FETAL CHANGES : 45%-Macrosomia 10%-IU malnutrition l
Complication of PTP MATERNAL l Anxiety l Traumatic vaginal delivery-Labor dystocia l Increased CS rate l PPH risk l Assisted delivery l Endometritis l Increased risk for thromboembolic dz
Fetal adverse events 1 -Fetal distress 2 -Fetal trauma brachial plexus injuries, clavicle fracture , shoulder dystoci 3 -Increased perinatal mortality cord compression due to oligohydromias(prolonged and variable FH deceleration); Fetoplacental insufficiency 4 -Fetal growth restriction (IUGR) 5 -Macrosomic infant- risk at postterm gestation increases eight fold, approaching 10 6 -postmaturity syndrome; Triad of long, thin malnourished infant with flaking skin and meconium stained skin (20% of postterm gestations)
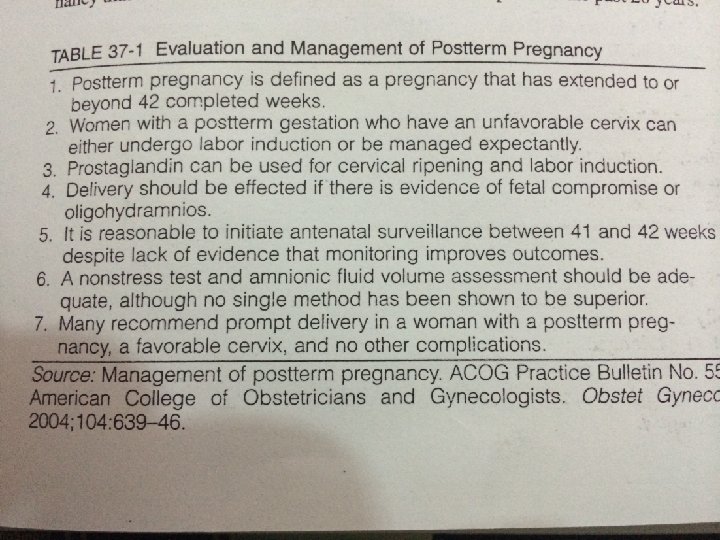
Mangment l Conformation of gestational age in antenatal l Antepartum intervention include elective induction of labor and antepartum fetal testing. monitoring with the goal of detecting early signs of fetal distress and preventing fetal death USG l AFI <5 oligohydramnios Macrosomia Placental grading P/V examination Assess inducibility-BISHOPS score
Post mature infant
INTRAPARTUM MANAGEMENT l Left lateral position l Continuous electronic fetal monitoring l Early ARM in active phase (hastens progress, detects meconium) l LSCS if CPD/macrosomia, fetal distress l Amnioinfusion (750 -1000 ml NS/RL) –If meconium stained liquor, variable deccelerations l Paediatrician called at delivery
Identification of patients that need delivery Ripe cervix Oligohydramnios Macrosomia Abnormal NST/BPP/CST Meconium stained liquor Unripe cx Normal fluid Normal NST/CST Normal fetal size DELIVERY Cervical assessment, NST, AFI Weekly at 40 & 41 wks Twice wkly thereafter Ripe cx Oligo Abn NST 42 WKS DELIVERY