POST CS PREGNANCY Problems Scar rupture Adherent placenta

POST CS PREGNANCY

Problems • • Scar rupture Adherent placenta Operative interference Peripartum hysterectomy

Uterine incisions • • Classical Kerr’s incision Kronig’s incision Inverted T shaped


LSCS scar Classical scar Apposition Better apposition Difficult to appose Healing in puerperium Better Imperfect Placental implantation May be over the scar Much more likely Rupture 0. 5 – 2% 4 -8% Tlming of rupture In labour In pregnancy and labour

Dehiscence Separation along the line of the previous scar but peritoneum over the scar intact

Rupture When all muscle layers including the peritoneum involved in the separation

Management options • Trial of labour or scar : VBAC / CS • Elective Caesarean section

Informed consent

Ø Planned repeat caesarean delivery • Maternal morbidity – 3. 6% Ø Trial of labour after caesarean Emergency repeat caesarean delivery • Maternal morbidity – 14. 1% Vaginal birth after caesarean (VBAC) • Maternal morbidity – 2. 4%

Uterine rupture Elective CS 1. 6 / 1000 Spontaneous labour 5. 2 / 1000 Induction with oxytocin 7. 7 / 1000 Induction with prostaglandins 24. 5 / 1000

Prerequisites to attempting VBAC • • • Obstetrician continuously to monitor labour Blood banking services Anesthesiologist, Pediatrician Continuous electronic fetal monitoring Decision to incision interval of < 30 minutes

• Successful trial – Vaginal delivery of a live fetus without scar rupture • Failed trial – When emergency CS is required or there is scar rupture

Previous history • • Type of prior uterine incision Prior indication Prior vaginal delivery Post operative infection

Present pregnancy • • No medical or obstetric complications Average sized baby Vertex presentation No CPD

Contraindications for VBAC • • Previous classical incision Previous two LSCS Previous inverted T-incision Previous extension of uterine incision Malpresentation Suspicion of CPD Medical or Obstetric complications Multiple pregnancies

VBAC • • Spontaneous onset of labour IV line Cross matched blood BP & Pulse every 15 minutes Continuous CTG Progress of labour by partogram Oxytocin is better avoided Epidural analgesia is safe

Signs of scar dehiscence • • • Late deceleration on CTG Persistent maternal tachycardia Suprapubic discomfort or Scar tenderness Vaginal bleeding Blood stained urine

Scar rupture • • Classical 4 – 9% T shaped 4 – 9% Low vertical 1 – 7% Low transverse 0. 2 – 1. 5%

Delivery • • • Cut short second stage Look out for excessive bleeding Routine exploration of scar is not recommended Scar explored – excessive bleeding Postpartum 4 -6 hours in labour room

Successful VBAC • 60 – 80% • Nonrecurring indication – 90% • Recurring indication – 60%

Indications for emergency CS • Unsatisfactory progress of labour • Signs of scar dehiscence • Should be done within 30 minutes of decision

“Removal of a child through an incision in the abdominal wall of an intact uterus”

Elective CS • Can be done at 39 weeks • Advantage - Availability of manpower • Disadvantage - Lower segment may not be well formed - Bleeding may be more • Iatrogenic prematurity

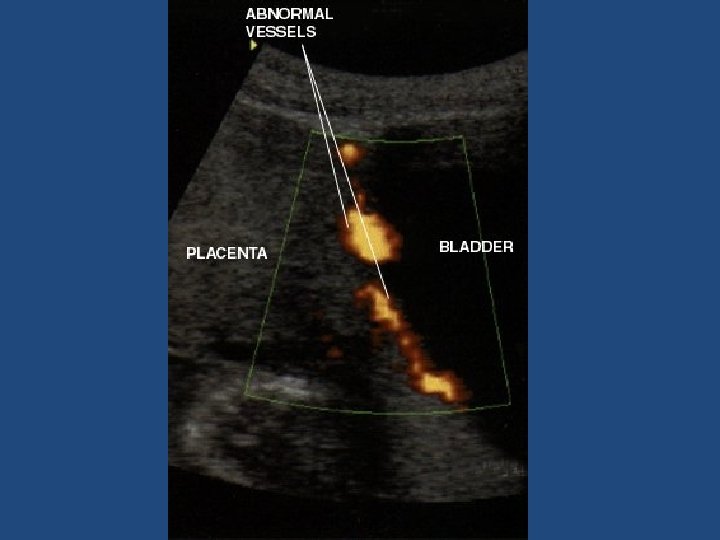
Repeat CS • Adhesions causing difficulty • Injury to bowel or bladder • PPH due to placenta praevia or Adherent placenta • Caesarean Hysterectomy

Ultrasound • Scar thickness 3. 5 mm or more • Placental location • Adherent placenta – absence of sub placental sonolucent zone

Nitabuch layer Zone of fibrinoid degeneration where invading trophoblasts meet the decidua C – Nitabuch layer
- Slides: 28