POPULATION HEALTH SCORECARD HIMSS MAY 2015 BILL LANGLEY

POPULATION HEALTH SCORECARD HIMSS MAY 2015 BILL LANGLEY

Practice Environment • 100+ PCPs • 20+ separate practice sites • 15 payer contracts with “population” arrangements • No historic internally-derived population quality measures

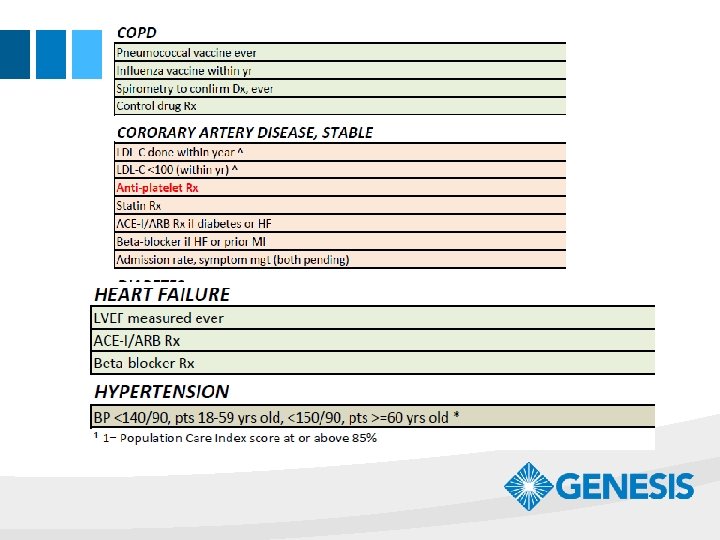
Design Requirements • Timely data and reporting • Comprehensive: diseases, prevention, care delivery • All patients, not only certain payers • Relevant measures, actually reflect quality of care • Easy to understand reports • Believable!
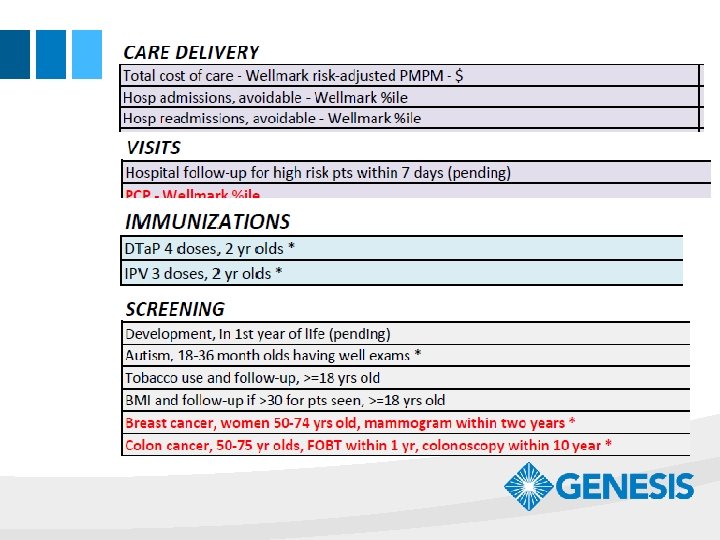

Choose Wisely • Use off-the-shelf measures • NCQA, NQF, AHRQ, ACS, ACC • Cross walk to payers’ measures

Control the Data Stream • Be realistic about pulling data • Probably will require add-on app • May require multiple sources, e. g. state immunization registries • Capture as much data as practical, so scores reflect physician’s true work • Loop back to data input processes and correct staff “bad habits”

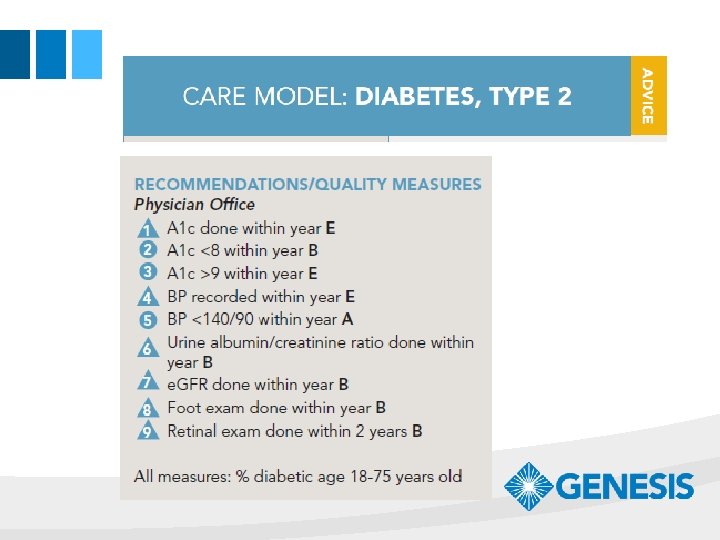
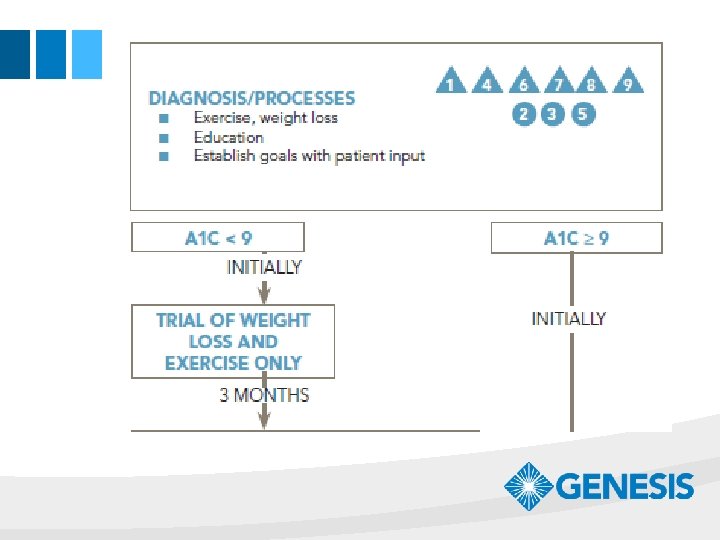
Connect Measures • Disease burden of the population • Care guidelines in use • Pull lists of patients (“Registries”)

Quality Control • No second chance with physicians • Test the accuracy of your measures by sampling actual patient records • Test again!

Life Cycle of a Measure • • • Reporting only Active Updated Retiring Archived

Evolve to Transparency • Start with masked provider identity • Wait for spontaneous requests to go “transparent” • Transparent provider identities will accelerate performance improvement • But don’t rush the process

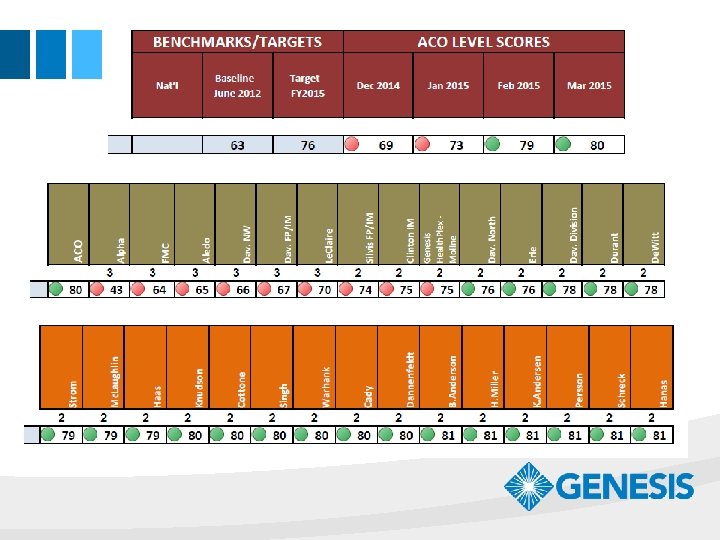
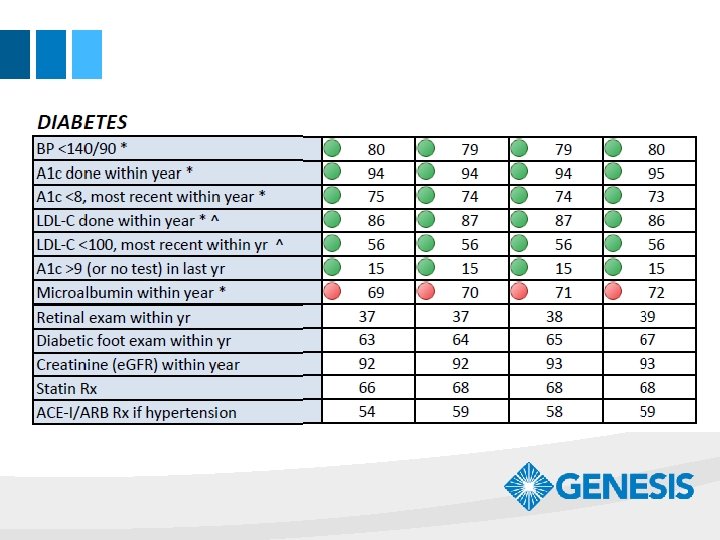
Does Measurement Drive Improvement? • Current Genesis quality scores are markedly higher than the baseline in 2012 • Physicians are competitive • Staff is too!

DIABETES IMMUNIZATIONS

THANKS!
- Slides: 18