Popliteal vessel injury Supparerk Prichayudh M D the

")





")









 • Save time • Amputation rate")





 –")


 • In complex extremity vascular injury, Damage control • Heparin-bonded")






 Skeletal / soft-tissue injury Low energy (stab; simple fracture;")



- Slides: 40
Popliteal vessel injury Supparerk Prichayudh, M. D.
• the most limb threatening of peripheral vascular injuries (amputation 14. 5%: NTDB) – The popliteal artery is a true end artery with a tenuous collateral supply. – The popliteal vein provides the bulk of lower leg and foot drainage.
History • 1906 The first use of vein graft to repair a traumatic aneurysm of the popliteal artery • WWI, WWII ligation – Amputation 72. 5% Debakey ME, Simeone FA. Battle Injuries of the Arteries in World War II : An Analysis of 2, 471 Cases. Ann Surg 1946 Apr; 123(4): 534 -79. • Korean / Vietnam Repair – Amputation 32. 4% and 29. 5%, respectively Hughes CW. Arterial repair during the Korean war. Ann Surg 1958 Apr; 147(4): 555 -61. Rich NM. Vascular trauma in Vietnam. J Cardiovasc Surg (Torino)1970 Sep-Oct; 11(5): 368 -77.
Anatomy • Femoral artery becomes popliteal artery out of the adductor hiatus • Popliteal fossa • Divides into – Anterior tibial artery – Tibioperoneal trunk
Popliteal fossa • Medial Pes Ancerinus – Satorius – Gracilis – Semimembranosus, Semitendinosus • Lateral Bicep femoris • Inferior Gastrocnemius
Incidence: popliteal a. injury • • NTDB 0. 1% 19% of all extremity arterial injuries Military 20 -26% Civilian – blunt mechanisms 20% to 75 – 5. 6 per 1000 cases of penetrating – 1. 6 per 1000 cases of blunt Fryburg, Surg Clin N Am, 2002
Diagnosis • PE • • • Deformity, wounds Bleeding, hematoma Pulses Signs of ischemia Neurological examination Posterior knee dislocation – Popliteal a. injury up to 25%
Hard vs. Soft signs of Vascular injury Hard signs Soft signs Active arterial (pulsatile) Minor bleeding Pulseless/ ischemia Injury in proximity to major vessel Expanding pulsatile hematoma Bruit or thrill Small to moderate size hematoma Associated nerve injury Operation Mandatory Further W/U
• Ankle Brachial Index – ABI < 0. 90 = 87% sensitive, 97% specific for arterial injury – In absence of hard signs, can substitute this for screening arteriography Lynch K, Johansen K, Ann Surgery, 1991. • Arterial Pressure Index – Injured limb SBP/ Uninjured limb SBP – < 0. 9 specificity 97%, sensitivity 95% – > 0. 9 NPV 99% Levy BA, Zlowodzki MP, Graves M, Cole PA. Screening for extermity arterial injury with the arterial pressure index. Am J Emerg Med 2005 Sep; 23(5): 689 -95.
Indications for angiography • Hemodynamic stability • Uncertain diagnosis – Soft signs – PVD • Unclear location – Multiple wounds, fractures – Shot gun wounds – GSW parallel to an artery
Non invasive studies • Doppler US – sensitivity 50% • CT Angiography – Sens 95 -100%, Spec 87% – Limitations: • difficulty differentiating spasm from occlusion • artifact from high attenuation structures like bullet fragments or other foreign matter Rieger M, et al. A, Traumatic arterial injuries of the extremities: initial evaluation with MDCT angiography. Am J Roentgenol 2006 Mar; 186(3): 656 -64. Peng PD, et al. , Brundage SI. CT angiography effectively evaluates extremity vascular trauma. Am Surg 2008 Feb; 74(2): 103 -7. Fishman EK, et al. Multidetector CT and three-dimensional CT angiography for suspected vascular trauma of the extremities. Radiographics 2008 May-Jun; 28(3): 653 -65; discussion 65 -6.
General Principle of management ABCs Active bleeding, limb threatening ischemia OR Stable, good limb viability may investigate Non-operative management non-occlusive lesion in asymptomatic patient • Pre-operative management • • – Prophylactic antibiotic – Single dose heparin iv if no C/I • Do not reperfuse dead limb! amputation
Operative management • Supine • Prep both legs for possible SVG harvesting • The leg is supported at the knee in slight flexion, hip abducted & external rotated. • Early fasciotomy (at the beginning of the operation) if needed
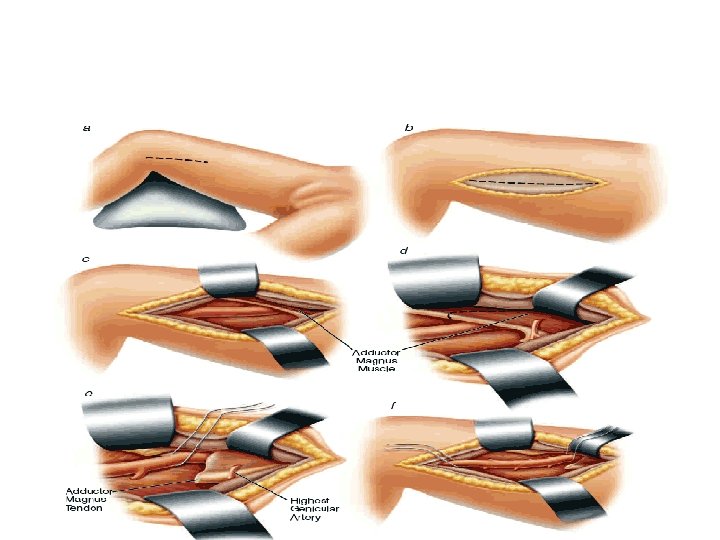
Exposure of proximal PA • Medial approach – anterior border of sartorius • Incise fascia lata • Identify groove between vastus medialis and satorius m. • Retract sartorius posteriorly to expose NV bundle • Retract vastus medialis anteriorly
Exposure of distal PA • Medial approach – a medial longitudinal incision placed 1 cm posterior to the distal femur and proximal tibia • Detach medial head of Gastrocnemius from Tibia and tract posteriorly
• May retract or cut Semimembranosus, Semitendinosus tendon to gain more exposure proximally Snyder, Surg Clin N Am. 1988
Principle of repair • Proximal & distal control • Identify injury • Resect the injured segment • Thrombectomy with a Fogarty catheter obtain good inflow and back-bleeding before the repair.
Intraoperative angiogram • Identify injury (limb threatening ischemia) • Save time • Amputation rate compared to formal angiogram (0% v. s. 30%) Callcut RA, et al. Impact of intraoperative arteriography on limb salvage for traumatic popliteal artery injury. J Trauma. 2009 Aug; 67(2): 252 -7. • Completion angiogram detect unsuspected problems requiring intervention in 8% Pasch AR, Bishara RA, Lim LT, et al: Optimal limb salvage in penetrating civilian vascular trauma. J Vasc Surg 3: 189– 195, 1986
Repair • Primary repair defect < 1 -2 cm • Graft (59 -84%) – Reverse SVG – PTFE
Vein graft • Pros – Better patency for anastomosis across knee joint Fryburg, Surg Clin N Am, 2002 • Cons – Time consuming – Donor site morbidity PTFE • Pros – Time saving – Same infection rate Feliciano DV, et al. Five-year experience with PTFE grafts in vascular wounds. J Trauma. 1985 Jan; 25(1): 71 -82. – Good patency Jaggers RC, et al. Injury to popliteal vessels. Arch Surg. 1982 May; 117(5): 657 -61. • Cons – Higher failure rate in popliteal a. (80%) • Martin LC, Mc. Kenney MG, et al. Management of lower extremity arterial trauma. J Trauma. 1994 Oct; 37(4): 591 -8.
Temporary intravascular shunt (TIVS) • In complex extremity vascular injury, Damage control • Heparin-bonded shunts – Argyle – Sundt • Self-constructed shunt - Inahara
Venous injury • Should be repaired in stable patient if technically feasible – – Lateral venorrhaphy, EEA Complex repair (PTFE, SVG) Patency 75% Before arterial repair Management and short-term patency of lower extremity venous injuries with various repairs. Parry NG, Feliciano DV, et al. Am J Surg. 2003 Dec; 186(6): 631 -5. • Limb threatening ischemia Shunt a. repair v. • Ligation is safe alternative esp. in unstable patients, complex injuries. – 86% free of edema at D/C Yelon, et al. J Trauma 1992 – DVT 78%, no significant sequelae of CVI Kurtoglu, et al. Am Surg 2007 – Long term anticoagulation?
Combined vascular and orthopedic injury • Restore perfusion 1 st ! • Definitive repair – stable, minimally displaced Fx • TIVS – complex, displaced Fx – TIVS Bone manipulation definitive repair – avoid major stress on vascular anastomosis
Early fasciotomy • • • Extremity swelling Severe distal musculoskeletal injury Prolonged shock Delayed restoration of flow (>4 -6 hr) Combined arterial-venous injuries Ligation of popliteal or multiple shank veins Snyder, Surg Clin N Am. 1988
4 compartment fasciotomy Asensio JA, Trunkey DD Current therapy of trauma and surgical critical care. Philadelphia: Mosby Elsevier; 2007.
Bypass exclusion • 2 separated incisions • Intercondylar tunnel of SVG • Simple, avoid massive dissection • Limited exposure to popliteal v. , bleeding from the injured vessels • Long term result? Exclusion and bypass--a new approach to popliteal artery injuries. Scott BG, Hirshberg A. J Trauma. 2004 Oct; 57(4): 913 -4
Amputation: when? • Non-viable or non-savagable limb –Irreversible limb ischemia –Extremely mangled limbs: MESS > 7 high amputation rate • 100% (Johansen 1990) • 45% (Callcut 2009) Callcut RA. J Trauma. 2009 Aug; 67(2): 252 -7. • Safe life before limbs!!! –Amputation can be life saving in life threatening extremity bleeding • Functional outcome consideration
Mangled Extremity Severity Score (MESS) Skeletal / soft-tissue injury Low energy (stab; simple fracture; pistol gunshot wound): 1 Medium energy (open or multiple fractures, dislocation): 2 High energy (high speed MVA or rifle GSW): 3 Very high energy (high speed trauma + gross contamination): 4 Limb ischemia No ischemia: 0* Pulse reduced or absent but perfusion normal: 1* Pulseless; paresthesias, diminished capillary refill: 2 * Cool, paralyzed, insensate, numb: 3* Shock Systolic BP always > 90 mm Hg: 0 Hypotensive transiently: 1 Persistent hypotension: 2 Age (years) < 30: 0 30 -50: 1 > 50: 2 * Score doubled for ischemia > 6 hours from Johansen et. al. 1990
Factors associated with amputation • • • Extensive soft-tissue injuries Associated skeletal trauma Knee dislocations Prolonged ischemic times Nerve injury High extremity AIS 1)Yahya et al. ANZ J Surg, 2005 2) NTDB J Vasc Surg. 2006 Jul; 44(1): 94 -100
Amputation rate 0 -44%
Conclusions: popliteal vessel injuries • The most limb threatening • Early Dx – Hard signs – Angiography Intraoperative • Early fasciotomy • Early repair – Good exposure – Good technique