Polycythemia Vera Bleeding Disorders Dr Megangela Christi Amores

Polycythemia Vera Bleeding Disorders Dr. Meg-angela Christi Amores

Polycythemia Vera • phenotypically normal red cells, granulocytes, and platelets accumulate in the absence of a recognizable physiologic stimulus • 2 per 100, 000 persons, sparing no adult age group and increasing with age

Etiology • Unknown • Genetic mutation • loss of heterozygosity on chromosome 9 p, due to uniparental disomy • leads to homozygosity for the mutant JAK 2 V 617 F • JAK 2 V 617 F is the basis for many of the phenotypic and biochemical characteristics of PV

Clinical features • Spenomegaly – initial presenting sign • first recognized by the incidental discovery of a high hemoglobin or hematocrit • Uncontrolled erythrocytosis causes hyperviscosity : • vertigo, tinnitus, headache, visual disturbances, and transient ischemic attacks • Systolic hypertension • venous or arterial thrombosis

Clinical features • Signs of vascular stasis: • Digital ischemia, easy bruising, epistaxis, acid-peptic disease, or gastrointestinal hemorrhage • Thrombocytosis: • Erythema, burning, and pain in the extremities, a symptom complex known as erythromelalgia – hyperuricemia with secondary gout, uric acid stones, and symptoms due to hypermetabolism can also complicate the disorder

Diagnosis • erythrocytosis in combination with leukocytosis, thrombocytosis, or both • elevated hemoglobin or hematocrit alone, or with thrombocytosis alone, the diagnostic evaluation is more complex • Hemoglobin > 20 , hematocrit > 60% • red cell mass and plasma volume determinations
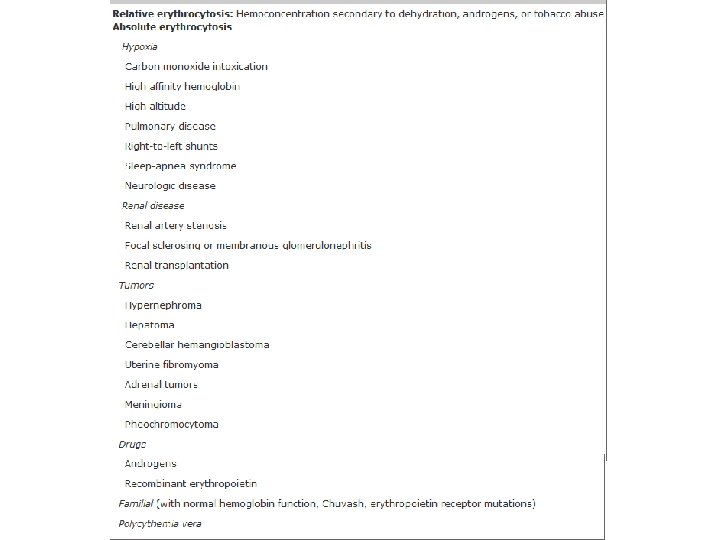

Diagnosis • To differentiate from hypoxia: O 2 saturation

Treatment • Thrombosis due to erythrocytosis is the most significant complication • maintenance of the hemoglobin level at 140 g/L (14 g/d. L; hematocrit <45%) in men and 120 g/L (12 g/d. L; hematocrit <42%) in women is mandatory to avoid thrombotic complications

Treatment • Phlebotomy – initially to reduce hyperviscosity by bringing the red cell mass into the normal range – Periodic phlebotomies thereafter serve to maintain the red cell mass within the normal range and to induce a state of iron deficiency – once an iron-deficient state is achieved, phlebotomy is usually only required at 3 -month intervals

Treatment • Anticoagulants are only indicated when a thrombosis has occurred • For pruritus: • hydroxyurea, interferon (IFN-), and psoralens with ultraviolet light in the A range (PUVA) therapy are other methods of palliation • Chemotherapy: • Hydroxyurea • never indicated to control the red cell mass unless venous access is inadequate

BLEEDING • Bleeding disorders
- Slides: 12