Polycystic Ovary Syndrome The Spectrum of Evaluation and










 • Testosterone-total and free •")
















 • Combination")





")



 OGTT: • Total cholesterol: •")

- Slides: 44
Polycystic Ovary Syndrome: The Spectrum of Evaluation and Management in the College Health Setting Martha Dannenbaum, MD, FACOG Gladys Gibbs, MD, MS, FACOG Meghan Windham, RD, LD, MPH Joe Dannenbaum, MS, ATC, CSCS
Disclosures • We have NO actual or potential conflict of interest in relation to this educational activity or presentation.
Objectives • 1. Identify the characteristics of PCOS. • 2. Identify the types of testing options available. • 3. Describe the non-pharmacologic management of PCOS. • 4. Describe the pharmacologic management of PCOS.
History and Basic Science
Polycystic Ovary Syndrome History • Multicystic ovaries first described in the mid 1800 s • Irving F. Stein, MD and Michael L. Leventhal, MD-first described the symptom complex of amenorrhea, hirsutism and enlarged ovaries in 1935“Stein-Leventhal Syndrome” • Ovarian wedge resection improved menstrual pattern and pregnancy rates • While the pathophysiology that leads to the polycystic ovary is difficult to define, it is clear that it develops when a chronic anovulatory state exists for a sufficient length of time • There are many causes of anovulation; therefore there are many causes of polycystic ovaries. • PCOS affects about 8 -10% of women of reproductive age
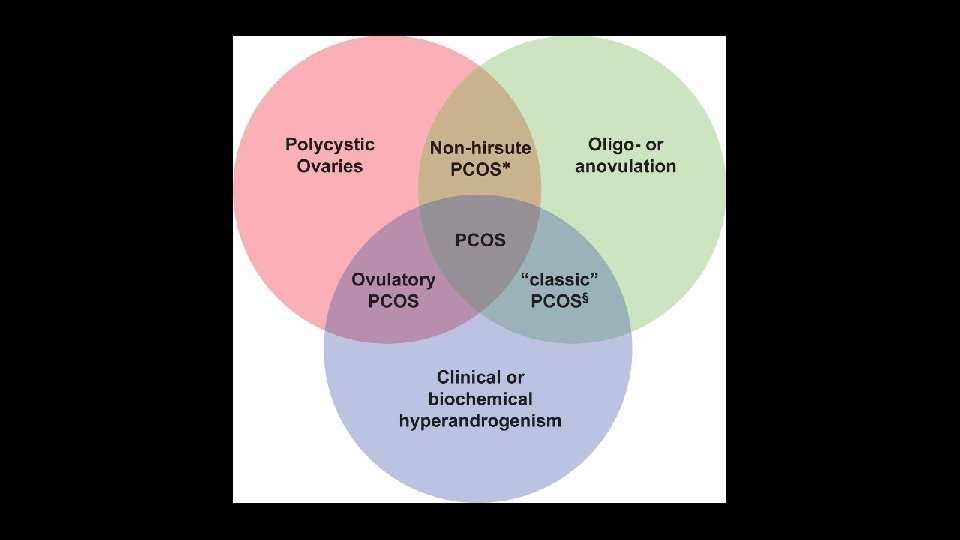
Diagnostic Criteria
Polycystic Ovary Syndrome Basic Science • Fundamental pathophysiologic defect unknown • Familial clustering suggests a genetic component • Endocrine state in women with chronic anovulation is characterized by a “steady state” in which hormone concentrations vary relatively little when compared to normal cycling women. • Increased serum LH concentrations, low normal FSH, increased LH: FSH ratio • Hyperandrogenism is the key feature of PCOS; increased androgens predominantly come from the ovary
“Current perspectives view PCOS as a complex disorder, …. wherein numerous genetic variants and environmental factors interact, combine, and contribute to the pathophysiology”
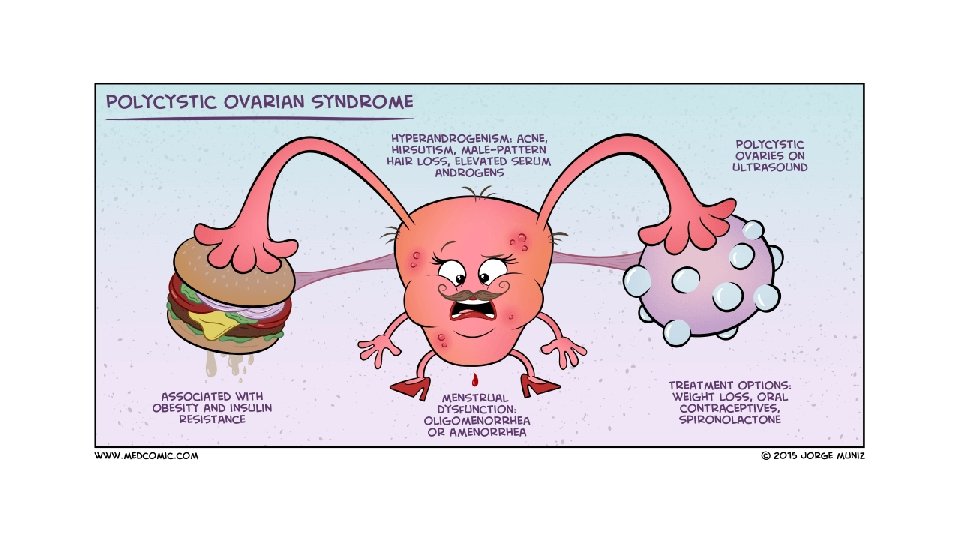
Clinical Manifestations • Oligo-anovulation • Irregular menstrual bleeding/oligomenorrhea • Infertility • Androgen Excess • Acne • Hirsutism • Ovarian Morphology • Obesity • Insulin Resistance/Diabetes Mellitus • Acanthosis Nigricans • Cardiovascular Disease
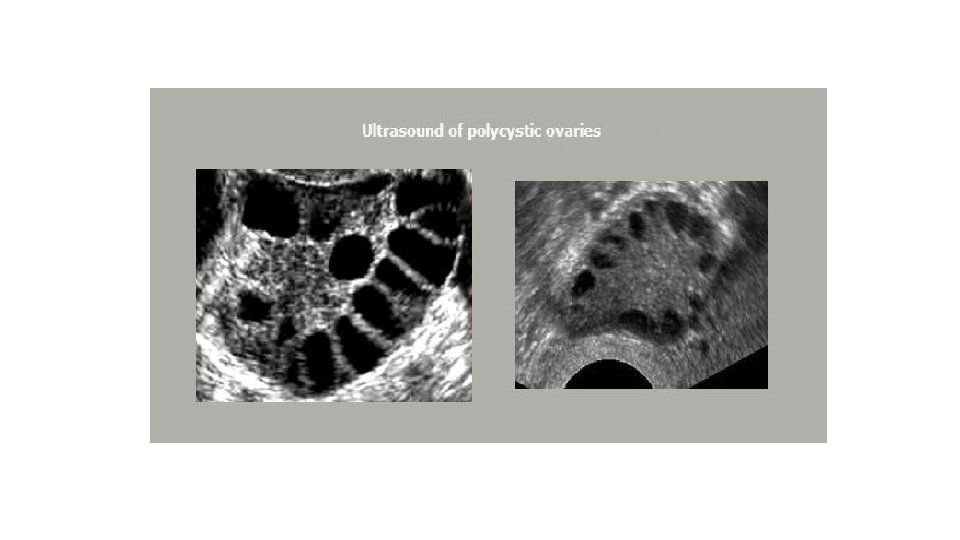
Screening, Evaluation and Diagnosis • History and Physical Exam • • • Irregular periods since menarche Hirsutism (may not be clinically evident) Family history Acne Overweight/obese • Laboratory Studies • Variable benefit, but…. • Radiology • Ultrasound not mandatory, but….
Lab studies to consider • HCG (based on history) • Testosterone-total and free • FSH/LH • Fasting glucose/insulin • 17 alpha progesterone
Management • Variable based on patient goals and presenting symptoms • All will benefit from lifestyle management
Lifestyle Management-Nutrition
Nutrition Modifications- Insulin Resistance Image from: http: //www. ethoshealth. com. au/announcements/confused-by-diabetes-heres-a-simple-explanation
Image from: http: //www. ethoshealth. com. au/announcements/confused-by-diabetes-heres-a-simple-explanation
Image from: http: //www. ethoshealth. com. au/announcements/confused-by-diabetes-heres-a-simple-explanation
How can my diet help? • The TYPE and TIMING of food can help normalize hormone levels in the body
Types of food • Lean protein • Fish, chicken, low fat cheese, lean ground beef • Healthy fats • Nuts, seeds, nut butter, olives, avocado, flaxseed, olive or canola oil • Trout, halibut, salmon, sardines, or herring (2 x a week) • Vegetables and fruit • Have at least one every time you eat! • High in antioxidants, good sources of fiber and anti-inflammatory • Complex Carbohydrates • Whole grain breads, brown rice, quinoa, oatmeal • Limit added sugars to 25 grams per day • Syrup, glucose, sugar, honey, evaporated cane juice, etc
Timing • Eat consistently- this will help regulate blood sugars • 3 meals a day • 2 snacks- mid-morning, afternoon • No longer than 4 hours between meals
Current Practices- TAMU • Initial nutrition assessment • • • Weight history and background information Evaluate current eating patterns for trends Barriers for making a change/ challenges with compliance Discuss carbohydrate content and specify needs based on individual Address exercise patterns • Follow up visits • Assess weight changes • Further discuss eating patterns and any changes made • Continued collaboration with physicians and counselors
Best Practices- TAMU • Group setting • Sense of belonging • 10 -12 participants • Grocery store tours • Label reading for carbohydrate content • Shopping while on a budget • Cooking Classes • How to modify recipes • Quick and easy meal ideas • Healthy snacking • Interdisciplinary Team • Counseling • Physician • Dietitian/Nutrition • Additional Resources • Use of Bod Pod for concrete thinkers
Lifestyle Management-Exercise
• Exercise and its benefits for underlying conditions of PCOS • Research in the last 10 years • • • Exercise or Physical activity and effects on obesity Exercise or Physical activity and effects on diabetes Exercise or Physical activity and effects on insulin resistance Exercise or Physical activity and effects on metabolic syndrome Exercise or Physical activity and effects on cardiovascular disease • Source: EBSCO/Medline complete 23, 876 articles 16, 762 articles 4, 642 articles 3, 971 articles 7, 139 articles
Exercise-physical activity • We have to get them moving • • • Cardiovascular exercise, resistance exercise, and flexibility Utilize student recreation centers Make it fun!!!!!!! Body weight exercising can be done anywhere and shortens the workout Aquatics: walking, running in the pool, water aerobics Scavenger hunts on campus Dancing Yoga 30 minutes a day is great but get them to start with 5 or 10 minutes
Process of exercise • Once moving again. • Teach proper progressions • Warm-up • Something to get blood flowing, increased HR, increased breathing • Dynamic stretching • Activity • Cool-down (walking, light jogging) Never overlook this step • Stretch • Static stretching
Management: Irregular bleeding • Confirm pregnancy status • Cyclic progesterone (medroxyprogesterone acetate) • Combination Hormonal Contraceptives (pills, patches, rings) • LARC
Audience Questions • True or False? Polycystic ovary syndrome is a leading risk factor for metabolic syndrome, obesity, insulin resistance, and type 2 diabetes mellitus. • The risks associated with Polycystic ovary syndrome can be mitigated through what treatment(s)? A. Weight loss B. Hormonal contraceptives C. Spironolactone D. All of the above • True or False? Treatment of PCOS depends on symptoms and whether the patient is planning a pregnancy.
Case Study #1: • 21 year old female student visits the health center reporting increasingly irregular menstrual periods and new dark hair growth on her upper lip, chin and the inner aspect of her thighs. She is not sexually active currently, but has been in the past with her last intercourse 8 months ago. Her last 2 “normal” periods were 4 and 6 months ago. She experienced menarche at age 13, with initial irregular cycles every 2 -3 months. She had mild to moderate facial acne as a teenager, which was treated successfully with minocycline. In high school, she was a cheerleader and ran cross-country on the varsity track team. During this time, she would occasionally have regular cyclic periods. Since coming to college, she no longer engages in sports other than occasional visits to the campus rec center. She is a student worker (16 -20 hours per week) and is a Junior Accounting major with a 3. 6 GPA. She is 5’ 6” and weighs 165 pounds (BMI 26. 6) , having gained 25 pounds since her freshman year.
Management: Hirsutism • Cosmetic • Plucking, waxing, shaving, threading • Electrolysis • Laser • Medical • • • Hormonal contraceptives Spironolactone (aldosterone antagonists) Finasteride (5 alpha-reductase inhibitors)-*off label use* Flutamide Insulin sensitizers (Metformin) Glucocorticoids
Management: Infertility The great majority of women with PCOS will be able to get pregnant and have a baby with fertility treatment. • Address Overweight/Obese • Ovulation Induction • Clomiphene Citrate • Aromatase inhibitors (letrozole)-*off label use* • Injectable Gonadotropins • Advanced Reproductive Technology • Artificial Insemination • In-vitro Fertilization • Look for other reasons for inability to conceive if these methods do not achieve pregnancy. • 40% of couples will have more than one factor impacting fertility
Case Study #2: • 28 year old female doctoral student visits the health center to discuss infertility. She has been married for 4 years and not using contraception for 18 months. Her husband is also a doctoral student and accompanies her to the visit. She reports irregular menses since menarche (age 13) which was treated successfully with oral contraceptives starting at age 15. She continued on OCPs until 18 months ago. Since stopping her OCPs she has only had 3 spontaneous menses. She has also noticed an increase in facial hair and acne. On physical exam she is 5’ 5” and weighs 219 pounds (BMI 36. 4). Her blood pressure is 135/85 mm Hg. She states she has been overweight since childhood and has had intermittent success with diets, always regaining the weight she lost. She does not regularly engage in exercise. Her waist circumference is 46 inches, suggestive of central obesity.
Management: General Health Risks • Address Overweight/Obese • Insulin Resistance • Insulin sensitizers (Metformin) • Cardiovascular • Statins • Mental Health • Screen for and treat depression • Cancer • Long term untreated oligomenorrhea increases endometrial cancer risk • Ovarian cancer
Pregnancy considerations: • Increased incidence of Gestational Diabetes • Increased incidence of Pregnancy Induced Hypertension (PIH) and Preeclampsia • Risks related to obesity • Hypertension • Thromboembolism • Increased maternal mortality • Increased risks of pre-term birth and perinatal mortality, even when controlling for multiple gestation resulting from infertility treatment
The older woman • Normal to Impaired glucose tolerance to Diabetes • Hypertension • Dyslipidemia • “Metabolic Syndrome” • Endometrial Cancer • Ovarian Cancer
Case study #3 • A 46 year old female graduate student, gravida 2, para 2, presents to the health center for a general health visit. She has been working as a high school science teacher and is returning to complete a Masters in Education program. She reports a history of irregular menses since menarche. She reports that she required Clomiphene citrate to achieve pregnancy. Her children, ages 12 and 14, were delivered at full term. Her second pregnancy was complicated by gestational diabetes. She had follow up diabetes testing about 6 months after she delivered and reports everything was normal. She is taking combination oral contraceptives, but because of her age is wanting to discontinue them. She reports she has been seeing her gynecologist annually and states she has always been told everything was fine. Her other personal and family history is negative. On examination, she is 5’ 4” and her weight is 168 pounds (BMI 28. 8). Blood pressure is 134/90. She is noted to have a slight amount of dark hair on her upper lip and around the areola of each breast. Fasting lab results are as follows:
• Fasting Glucose: • 2 hour (75 gm) OGTT: • Total cholesterol: • HDL cholesterol: • LDL cholesterol: • Triglyceride: 96 mg/d. L 162 mg/d. L 218 mg/d. L 39 mg/d. L 163 mg/d. L 166 mg/d. L
Questions?