Point Prevalence Survey of Hospital Acquired Infections Antimicrobial

Point Prevalence Survey of Hospital. Acquired Infections & Antimicrobial Use in Ireland PPS Data Collector Training April 2017 Background & Introduction to PPS Presentation 1

What is a PPS? • A prevalence survey provides data at one particular point in time ‘snapshot’ • Prevalence = numerator / denominator • Numerator = number of patients on the ward who have an active HAI at the time of the survey • Denominator = All eligible patients present on the ward at 8 am on the day of the survey for that ward

What is a PPS? • PPS team visits a ward at 11 am on 10/5/17 • 29 patients present on the ward at 8 am • The PPS team decides that 26 patients are eligible for inclusion in the PPS: – Two have since been transferred to other wards – One has been discharged home

What is a PPS? • After completing the PPS for the ward: • 9 patients receiving systemic antimicrobials • Prevalence of antimicrobial use = 9/26 x 100 = 34. 6% • 4 patients met case definitions for active HAI • HAI prevalence on the ward = 4/26 x 100 = 15. 3%
 participated")
Hospital Infection Society 2006 PPS: Ireland • • • 44 acute hospitals (88%) participated in 2006 PPS 7, 541 patients surveyed 369 patients with HCAI prevalence = 4. 9% Systemic antibiotic use prevalence = 34. 2%
 •")
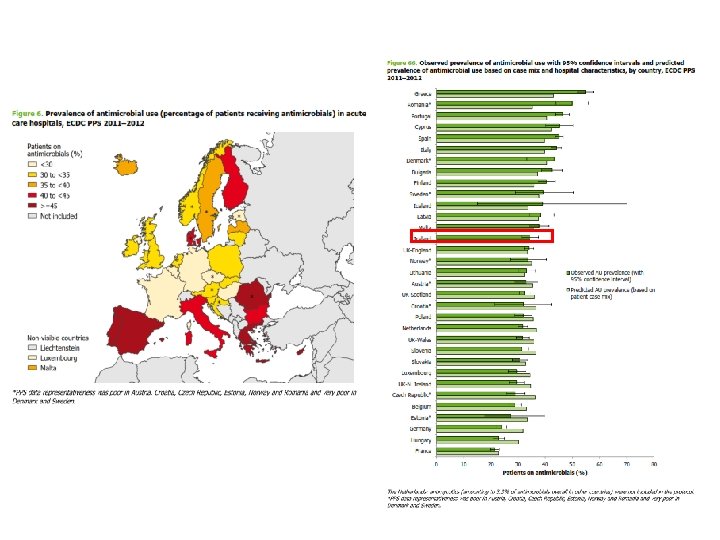
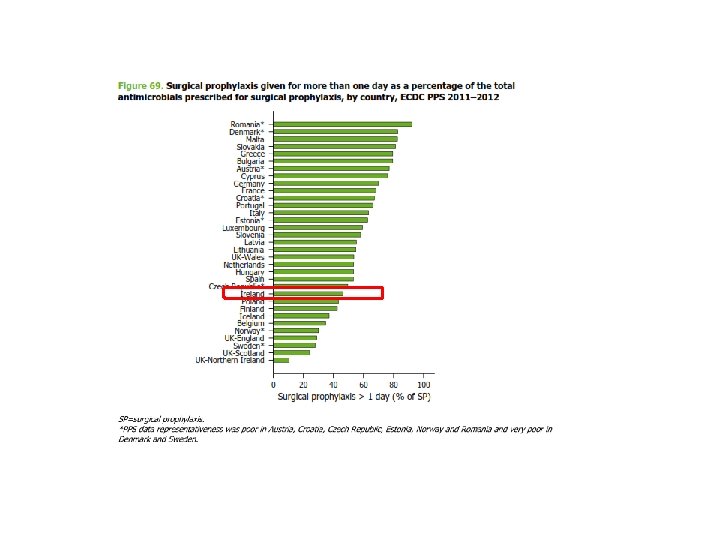
ECDC 2012 PPS: Ireland • 50 acute hospitals (42 public & 8 private) • 9, 030 patients • 501 active HAI (5. 2%): • • • SSI – 18% Pneumonia – 17% UTI – 15% BSI – 13% & of those, 42% were vascular catheter related CDI – 6% • 4, 532 antimicrobial prescriptions (34%): • • • 63% IV 78% treatment of infection 11% surgical antimicrobial prophylaxis, of which 47% >24 hrs 8% medical prophylaxis Documented indication in 83%

http: //www. hpsc. ie/AZ/Microbiology. Antimicrobial. Resistance/Infection. Controland. HAI/Surveillance/Hospital. Point. Prevalence. Surveys/2012/PPS 2012 Reportsfor. Ireland/

What are the changes in PPS 2017 protocol?

What’s been happening in Ireland since 2012?

Revised PCHCAI Standards to be published in 2017
 • 2014: National guidelines revised • Transition in laboratory testing")
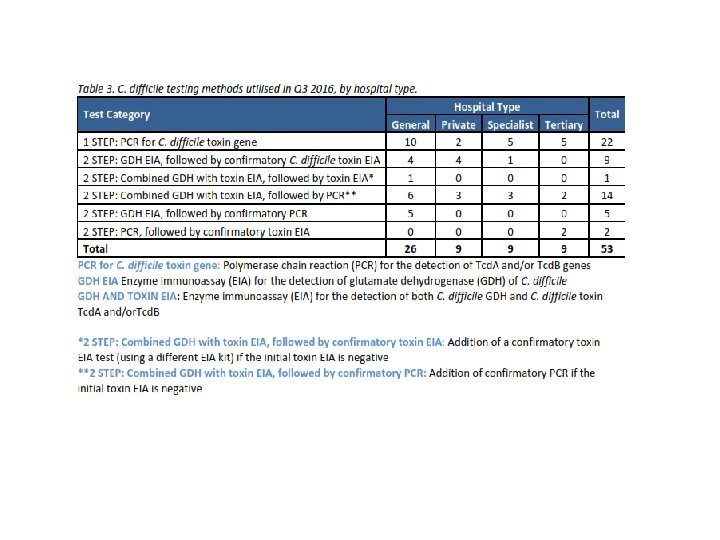
C. difficile infection (CDI) • 2014: National guidelines revised • Transition in laboratory testing protocols • Enhanced CDI surveillance scheme continues, with increase in participating hospitals 44 (2012) to 53 (2016) • National quarterly report issued • Quarterly report issued to each participating hospital

Source: HPSC www. hpsc. ie


S. aureus invasive infection • Captured via EARS-Net – ~99% population coverage – Some microbiology laboratories have suspended participation, due to resource issues • S. aureus BSI via enhanced surveillance scheme – 19 laboratories participated in 2016 – 23% of MRSA BSI & 20% of MSSA BSI deemed device-related Source: HPSC www. hpsc. ie

*2016 data are provisional to the end of Q 3 only (note: data missing from 2 laboratories for Q 3); ‡ 2015 missing data from 3 laboratories for 2 quarters each Source: HPSC www. hpsc. ie


E. faecium *2016 data are provisional to the end of Q 3 only (note: data missing from 2 laboratories for Q 3); ‡ 2015 missing data from 3 laboratories for 2 quarters each VRE, vancomycin-resistant enterococcus; VREfm, vancomycin-resistant E. faecium; VSEfm, vancomycin-susceptible E. faecium Source: HPSC www. hpsc. ie

E. coli

Multi-drug resistant K. pneumoniae • 1, 310 MDRKP cases reported (Q 1 2014 – Q 3 2016) from 87% of acute hospitals • 20% increase in MDRKP reported to Q 3 2016 versus same period 2015 • 2/3 reported in hospitalised patients • 59% required treatment of MDRKP infection

CRE • 15% of MDRKP also carbapenem resistant • 195% increase in carbapenem resistant K. pneumoniae to end Q 3 2016 versus 2015 • CRE outbreaks in acute hospitals & LTCF • From January 2017, MDRKP surveillance replaced by CRE surveillance

+ 90 CPE confirmed Jan – Feb 2017 Data courtesy of Prof M Cormican, CPEARLS

Hospital antimicrobial consumption Source: HPSC www. hpsc. ie

Hospital antimicrobial consumption 2017 PPS will provide you with data on compliance or non-compliance with local restricted use policy Source: HPSC www. hpsc. ie

Source: HPSC www. hpsc. ie

Aims of this PPS • To repeat a PPS of HAI & antimicrobial use across all EU Member States during 2016 -17 using a common protocol • To estimate the total burden of HAI & antimicrobial use within: – – – EU Each Member State Each participating healthcare facility By specialty type By patient type

European PPS: 2011 -12 Estimated on any day in Ireland, 494 patients with HAI & 3, 289 on antimicrobials Estimated in any year, 20, 491 patients in in Ireland with HAI 28

Aims of this PPS • To share the results of the PPS with those who need to know: – – – Local Regional National International EU • To use the data generated within YOUR hospital to help YOU and your colleagues to: – – Identify priority areas for future targeted HAI surveillance Identify interventions to prevent HAI Identify areas for targeting antimicrobial stewardship Support business cases for improved IPC, antimicrobial stewardship, surveillance & microbiology laboratory diagnostic resources

Summary • Last PPS performed in Ireland five years ago • Many interim developments to raise awareness of HAI & need for prudent antimicrobial use • 2017 PPS provides us with the opportunity to see where we are now, to direct our future interventions for ongoing improvement in patient care and staffing levels related to IPC, antimicrobial stewardship, surveillance and microbiology laboratory activities

Overview of data to be collected during PPS A 1 – PPS team A 2 – Night nursing & midwifery staff B – PPS team leader C – PPS team assisted by staff caring for patients
")
Ward List (Form A 1)
")
Ward List (Form A 2)
")
Hospital Form (Form B)
")
Hospital Form (Form B)
 There is space on Form C to record up to")
Patient Form (Form C) There is space on Form C to record up to five systemic antimicrobial prescriptions AND up to three different hospital-acquired infections
 Use extension sheet Form C Pages 3 & 4 for")
Patient Form (Form C) Use extension sheet Form C Pages 3 & 4 for HAIs 2 & 3 and antimicrobial prescriptions 3, 4, 5
 • Two pages for vast majority of patients – extension")
Patient Form (Form C) • Two pages for vast majority of patients – extension sheets for patients with ≥ 2 HAI or ≥ 3 antimicrobials • Five sections: – Section 1 – Patient details – Section 2 – Risk factors – Section 3 – Condition of interest – HAI Y/N & Antimicrobial use Y/N – Section 4 – HAI data – Section 5 – Antimicrobial use data Sections 1, 2, 3 completed for EVERY eligible patient 100%
 • Two pages for vast majority of patients – extension")
Patient Form (Form C) • Two pages for vast majority of patients – extension sheets for patients with ≥ 2 HAI or ≥ 3 antimicrobials • Five sections: – Section 1 – Patient details – Section 2 – Risk factors – Section 3 – Condition of interest – HAI Y/N & Antimicrobial use Y/N – Section 4 – HAI data – Section 5 – Antimicrobial use data Sections 1, 2, 3, 4 completed for EVERY eligible patient with an active HAI ~ 5 - 10%
 • Two pages for vast majority of patients – extension")
Patient Form (Form C) • Two pages for vast majority of patients – extension sheets for patients with ≥ 2 HAI or ≥ 3 antimicrobials • Five sections: – Section 1 – Patient details – Section 2 – Risk factors – Section 3 – Condition of interest – HAI Y/N & Antimicrobial use Y/N – Section 4 – HAI data – Section 5 – Antimicrobial use data Sections 1, 2, 3 & 5 completed for EVERY eligible patient receiving systemic antimicrobials ~ 33%

Your hospital. . TOTAL NUMBER OF PAPER FORMS TO BE COMPLETED* 150 ACUTE BEDS DIVIDED INTO 8 WARDS 300 ACUTE BEDS DIVIDED INTO 12 WARDS 600 ACUTE BEDS DIVIDED INTO 22 WARDS Ward Lists (Forms A 1 & A 2) 8 12 22 Hospital Form (Form B) 1 1 1 Patient Forms (Form C) 150 300 600 Form C Section 1, 2, 3 150 300 600 Form C (AMU) Section 1, 2, 3 & 5 50 100 200 Form C (HAI) Section 1, 2, 3, & 4 8 15 30 *Completed paper versions of all Form A 1 s, one Form B & all Form Cs are used to enter your hospital’s PPS data onto secure ‘web-based’ data entry system
")
Patient Form (Form C)
 The answers to 10/12 (83%) questions in Section 1 &")
Patient Form (Form C) The answers to 10/12 (83%) questions in Section 1 & 2 can be directly transcribed from the completed Ward List A 2 For each eligible patient, the PPS team will need to decide: §Admitting consultant’s specialty – prepare and laminate list ahead of PPS & give a copy to each PPS team member §Surgical procedure for patients who have had surgery on this admission §Underlying disease prognosis – review of notes and talk to ward staff
 §‘Patient on antimicrobials’ on Ward List – BUT double check")
Patient Form (Form C) §‘Patient on antimicrobials’ on Ward List – BUT double check medication charts – MP, SP could be missed §Also check Ward List to identify patients who have undergone surgery in the last 24 hours to pick up surgical antimicrobial prophylaxis administered since 8 am yesterday
")
Patient Form (Form C)
")
Patient Form (Form C)

Getting ready to do your PPS 1. PPS team identified and trained 2. PPS team leader has hospital code (same as 2012 code) and webform log-in username and password 3. VPN connection tested for webforms data entry 4. Local PPS dates agreed 5. PPS ward schedule prepared & distributed to wards 6. Ward List A 1 (one per ward) started in consultation with CNM 7. DONM to request ward CNMs ensure their Ward List A 2 completed by 8 am on day of PPS

Getting ready to do your PPS 8. Brief night nursing manager on Ward List A 2, in case of queries 9. Data gathered for Hospital Form B 10. Ward codes, ward specialty, consultant specialty assigned, local antimicrobial restricted list with laminated copy for each data collector 11. Ward list A 2 & Instruction Sheet given to nursing staff on day prior to PPS 12. Sufficient copies of patient forms, protocols available 13. Administrative support identified and trained in form entry 14. Verify PPS data entry on VPN connected PC available

Any Questions? pps 2017@hpsc. ie
- Slides: 51