pneumonia Dr Bandar ghazal CAP HAP 48 hrs

pneumonia Dr. Bandar ghazal

• CAP • HAP : 48 hrs after admission to hospital. • VAP : 48 hrs after mechanical ventilation. • Community acquired pneumonia : Ranges from mild disease which managed as ambulatory cases to fatal infection. Rates of hospitalization increased with age

• • • Fever Cough Shortness of breath Chest plain In elderly or immunocompromised pt these symptoms maybe mild or absent

• Bacterial and viral • Less commnly fungal and mycobacterium • Risk factors for pathogen causing CAP are listed below

• • Strp pneumoniae. Staphylococcus aureus. • • H. Influenza. Legionellla. Enerobacteriaceae. Moraxella catarrhalis. • Anaerobes. • Mycoplasma • • Viral ( influenza virus , parainfluenza , rhinovirus ) Fungal , mycobacterium

• Streptococcus pneumoniae was considered the leading cause for pneumonia , but incidence decreasing bz of vaccination strategy , accounting for about 15 % of cases of hospitalized pt. • Staph aureus and enterobacteriaceae are rising. • EPIC trial : was done on CAP during hospitalization more identified single or multiple viruses rather than bacteria

• Typical pnuemonia • Atypical pneumonia : Caused by organism not cultured by standard media including virus , legionella , mycoplasma and chlamydia

Diagnostic evaluation • • CBC KFT CRP Chest x-ray • Sputum culture ( value in pseudo , staph)sensitivity about 80% of strp pneumoniae befor starting AB • Blood culture • Nasopharyngeal swab for viral work up. (rapid test , PCR ) • ABG • Pneumococcal antigen urinary test positive in 70 % of cases • Legionella urinary antigen test positive in most pt with legio. pneumophilia serotype 1

• Chest xray : • If x-ray is normal upon presentation , what should I do ?
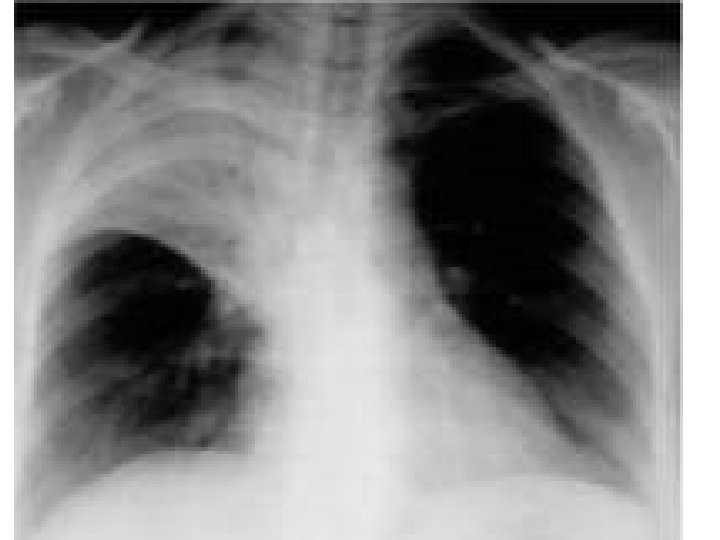



Lobar pneumonia Right lower lobe pneumonia Lung absess , cavitary lesion Interstital infiltrates Streptococcus pneumoniae Oral anaerobes (aspiration ) Alcoholic , stroke , neuro disease Anaerobes Legionella Staph, aurues Mycoplasma Mycobacterium chlamydia Actinomyces Klebsiella. Pleural effusion Strep Staph. aurues Anaerobes

• If chest xray was not diagnostic upon presentation : we should repeat xray after 24 hours • chest ct scan

• If concomitant pleural effusion thicker than 1 cm should go thoracocentesis to exclude empyema requiring drainage.

Management • Clinical judgment is the most important , scoring system was validated to help us in clinical judgment. • CURB 65 • Confusion • BUN > 20 mg / dl • RR >or equal 30 / min • SBP <90 , DBP <60 Age >or equal 65 years One score for each Ambulatory treatment is appropriate for most pt with score 0 -1

• Did the pt receive any antibiotics in last 1 - 3 months ?
 Treatment directed against")
ANTIMICROBIAL THERAPY • Ambulatory pt : ( without significant comorbidities ) Treatment directed against strep. Haemophilus influenzae and atypical bacteria. Mono therapy with doxycycline or macrolides ( azithro , clairtho ) If suspicion of strep. macrolides resistance : B lactam and macrolides or quinolones such as levofloxacin or moxifloxacin.

• Is ciprofloxacin is suitable for pnuemonia ? • Yes • No

• If pt have significant comorbidities : Quinolone Or B -lactam plus macrolides ( high dose amoixicillin ) Second generation cephalosporines (cefuroxime , cefaclor , Doxycycline can replace quinolone and macrolides in case of side effect.

• Pt requiring hospitalization : Parenteral B lactam ( third generation cephalosporine or ampicillin –sulbactam ) Plus macrolide or quinolone Or monotherapy with quinolone

• CAP requiring ICU admisson : Mono therapy with quinolone is contraindicated. Parenteral therapy B lactam and macrolide or quinolone

• MRSA : Pt on dialysis Critically ill pt Preceding influenza infection Drug abuser Gram positive cocci in clusters Failure of convential therapy Pleural based lung nodules Cavitary lesion Vancomycin , linezolid , Can we use daptomycin ? ?

• Pseudomonas aeruginosa : Most cases are HAP , but can occur as CAP Immunocompromised pt Underlying lung disease (cystic fibrosis , bronchiectasis ) Two anti pseudomonal therapy is indicated : B lactam (piperacillin - tazobactam , cefepim , meronem ) And antipseudomonal quinolone (levofloxacin , ciprofloxacin ) or amino glycosides

Duration of therapy • Uncomplicated stable CAP If pt improve in first 3 days , 5 to 7 days course is enough. For MRSA : , enterobacreriaceae , fungal At least 14 days.

• Lack of response to treatment rise suspicion of resistant organism or atypical organism , loculated infection (empyema ) or an infection mimic (tumor , vasculitis , pulmonary embolism ) • Pt with significsant pleural effusion should be conisdered for thoracocentesis

Complications • • CAP has mortality rate of 10 -12 % among hospitalized pt. Localized lung inflammation. Empyema ARDS due to ( Vigorous immune response resulting in acute respiratory distress syndrome ) • • • Delirium Cardiac arrhythmia ( A FIB ) AKI Spread of infection Toxicity related to medications Adrenal insufficiency ( water house friderichsen syndrome )occurring in setting of bacterial infection / septic shock.

• Recent meta analysis found that pt hopitalized for sever CAP , glucocorticoids adminstration was associated with reduced mortality , reduced mechanical ventilation need and shorter duration in hospital. reducing ARDS.
- Slides: 28