Pneumoconiosis Prof DR Waqar Al Kubaisy 1 Pneumoconiosis

Pneumoconiosis Prof DR. Waqar Al – Kubaisy 1

Pneumoconiosis contents • Definitions • Pathogenesis • Types • Individual diseases – Silicosis – Asbestosis – Anthracosis • Preventive measures Part 2 2
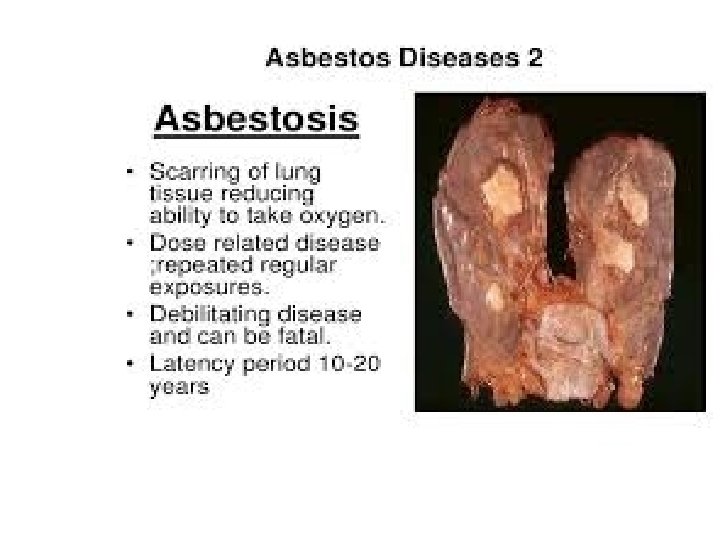

• Asbestosis: ASBESTOSIS Asbestos fibers is diffuse interstitial pulmonary fibrosis that occurs secondary to the inhalation of asbestos fibbers. • It is considered separately from other asbestos-related diseases, such as benign pleural effusion , , malignant mesothelioma, and bronchogenic carcinoma Asbestos is the commercial name given to certain types of fibrous materials. They are silicates combined magnesium Formed of fibrous magnesium silicate. Asbestos is a natural mineral that can cause serious health problems, like malignant mesothelioma, . Exposure most often occurs in the workplace, but can happen to anyone who comes into contact with asbestos in homes, buildings and various products. 4 physical properties

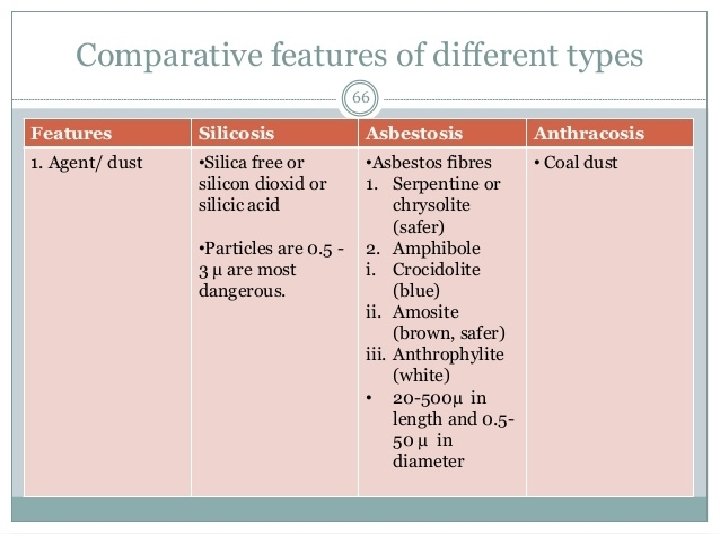
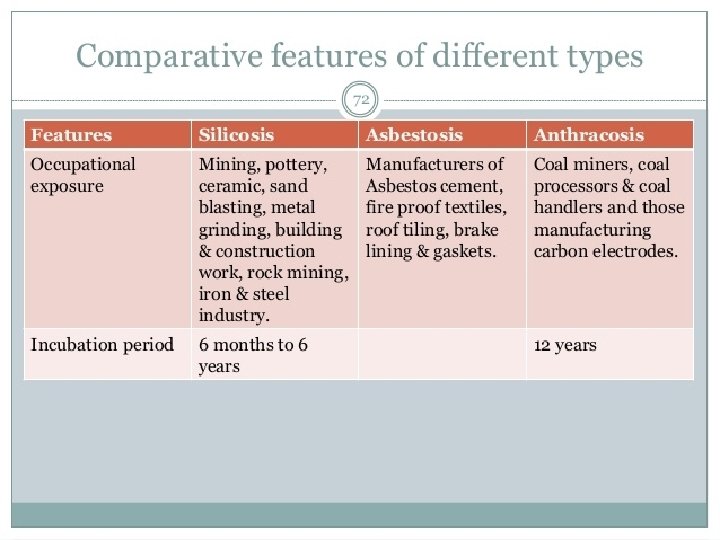
Asbestos fibres are usually from 20 to 500 μ in length and 0. 5 to 50 μ in diameter. - Asbestos Posses - thermal , - noise , resistance, - water and - chemical - flexible and high tensile strength �Uses: v Due to its physical properties, it is used in manufacture of �fire proof textile, �wire insulation, � friction materials (break lining), � roofing and floor products, �ship construction and �paints. Asbestos fibers Asbestos is used Asbestos cement factories – Asbestos textile industry and – Asbestos mining and milling § brake lining ﺑﻄﺎﻧﺔ ﺍﻟﻔﺮﺍﻣﻞ , § gaskets and § several other items.

Significant occupational exposure to asbestos occurs mainly in – Asbestos cement factories – Asbestos textile industry and – Asbestos mining and milling. 6

• Asbestos fibre is classified into 2 large groups q Serpentine: Chrysotile fibers , have curved appearance (white asbestos). v which is hydrated magnesium silicate v 93% of commercial use q Amphibole. : chain silicate with straight line • contains little magnesium. v , 7% of commercial use v This type occurs in different varieties, e. g. • Amosite (brown asbestos), • Crocidolite (blue asbestos), • Chrysolite,

chrysolite and amosite 8

ASBESTOSIS §At risk groups: § plumbers, ، ﺍﻟﺴﺒﺎﻛﻴﻦ §insulation workers، ﻋﻤﺎﻝ ﺍﻟﻌﺰﻝ , §carpenters ﻭ ، ﻟﻨﺠﺎﺭﻳﻦ , and §welders، ﺍﻟﺤﺎﻡ , § Miners and millers of asbestos. v Prevalence increase with length of employment (dose response) v Smokers and x smokers carry greater risk and higher mortality �Types of exposures: 1) Direct: primary → miners and millers Secondary → manufacturing plants 2) Indirect: bystander exposure and household contact 9

ASBESTOSIS § Asbestos enters the body by inhalation, and § fine dust may be deposited in the alveoli. § The fibres are insoluble. § § The dust deposited in the lungs causes pulmonary fibrosis leading to respiratory insufficiency and death; Ø carcinoma of the bronchus; Ø The risk of bronchial cancer is reported to be high if occupational exposure to asbestos is combined with cigarette smoking Ø mesothelioma of the pleura or peritoneum; q Mesothelioma, a rare form of cancer of the pleura and peritoneum, v has been shown to have a strong association with the crocidolite (blue asbestos) variety of asbestos. Mesothelioma

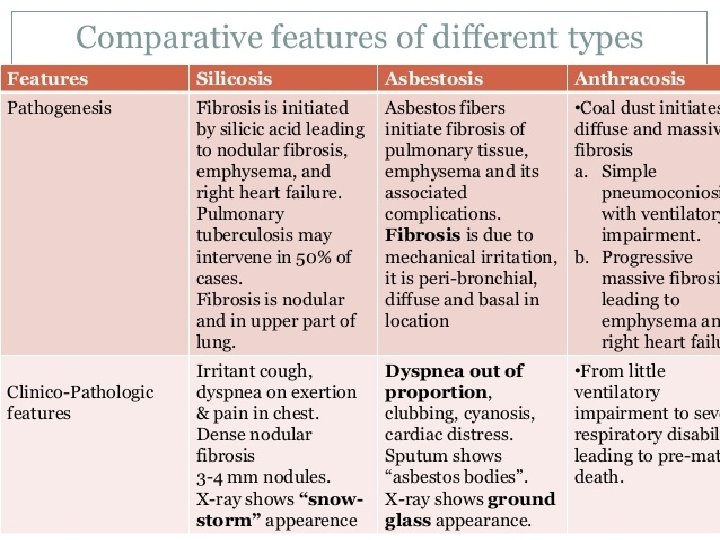
v mesothelioma does not usually appear until after 5 to 10 years of exposure. In Great Britain, an association was reported between mesothelioma and living within 1 km of an asbestos factory v cancer of the gastro-intestinal tract(Cancer larynx ) v The fibrosis in asbestosis is due to mechanical irritation, and is Ø peribronchial, diffuse in character, and basal in location interestitium (peribronchial, diffuse and basal fibrosis). o in contrast to silicosis in which the fibrosis is nodular in character and present in the upper part of the lungs. v The lung architecture is changed leading to honeycomb and intense peribronchial cellular reaction Ø may cause narrowing or obstruction of airway lumen. q Average latency period is 20 -30 years

ASBESTOSIS q Clinically the disease is characterized by Ø Dyspnoea gradually increases with increase in irregular opacities profusion and even after exposure has ceased. Ø Cough &phlegm. Ø Chest pain Ø. Bilateral late inspiratory crepitation on posterior Lung bases v In advanced cases, there may be § Clubbing of fingers, § cardiac distress and § cyanosis. q The sputum shows "asbestos bodies" v which are asbestos fibres coated with fibrin v Lung function change: Restrictive impairment with ↓ lung volumes (FVC, TLC) FEV 1/FVC ratio is usually preserved first second of forced expiration (FEV 1) to the full, forced vital capacity (FVC). X-ray picture: 12

Cont. . . Clinically characterized ASBESTOSIS q X-ray picture: v Bilateral diffuse nodular & or irregular oval opacities Ø predominant in lower lung zones, Ø Densely profuse opacities may obscure cardiac outline and dome of diaphragm (shaggy heart). Ø and “Shaggy heart sign q • At histopathologic analysis, v asbestos bodies, which may consist of a single asbestos fibber surrounded by a segmented protein-iron coat, can be identified in intraalveolar macrophages q Diagnosis: 1 - History of exposure: exposure over (10 -20) years is usually necessary. 2 - Clinical picture: particularly dyspnea and clubbing of fingers. 3 - X-ray picture: irregular basal opacities (ground glass ). 4 - Pulmonary function: restrictive abnormality. 5 - Broncho-alveolar lavage (BAL): Contain Asbestos bodies

14
: the patient is younger, clinically")
ASBESTOSIS D. D: �Idiopathic pulmonary fibrosis (I. P. F): the patient is younger, clinically and physiological impairment is more sever and progress rapidly. Treatment Strategy: Once established, the disease is progressive even after removal of the worker from contact Ø Stopping additional exposure Ø Careful monitoring to facilitate early diagnosis Ø Smoking cessation Ø Regular influenza and pneumococcal vaccines Ø Disability assessment Ø Pulmonary rehabilitation as needed Ø Aggressive treatment of respiratory infections Ø Health education to patient
 use of safer types of asbestos")
The preventive measures consists of : ASBESTOSIS (1) use of safer types of asbestos (chrysolite and amosite); (2) substitution of other insulants: glass fibre, mineral wool, calcium silicate, plastic foams, etc. ; (3) rigorous dust control; (4) periodic examination of workers; biological monitoring (clinical, X-ray, lung function), and (5) continuing research. Control Measures Of Asbestos • PEL 0. 1 fiber/m. L 3 (TWA 8). (8 -hour total weight average (TWA) § § § • permissible exposure limit (PEL) Switch to alternate material, man-made fibers (MMF) are considered Engineering controls include enclosure, increased ventilation, wet manufacturing. - Use of personal respirators. - Stop tobacco smoking.
: § Constitute 3")
. Man-made vitreous fibers ﺍﻷﻠﻴﺎﻑ ﺍﻟﺰﺟﺎﺟﻴﺔ , MMVF (MM mineral fibers): § Constitute 3 main species: - Glass fibers (glass wool, continuous glass filaments) - Mineral wool (rock wool and slag wool) - Ceramic fiber. § They used as a substitute for asbestos since the latter were banned due to its bad health effects. § They posses high tensile strength, perfect elasticity, thermal and electrical properties and moist and corrosion resistance. § They have a toxic effect on peritoneal and pulmonary macrophages and structure chromosome alteration in mammalian cells. § TWA 8 should keep below 1 fiber /CM 3 as asbestos.
 has carried out studies in Indian")
NIOH (National Institute of Occupational Health, New Delhi) has carried out studies in Indian Asbestos industries. Its observations were • Asbestos Cement Industry: – Study carried out in 4 (Ahmedabad, Hyderabad, Coimbatore and Mumbai) of the total 18 asbestos cement factories in India. – The prevalence of asbestosis in these factories varied from 3% to 5%. – The levels of asbestos fibres were found to be higher than the permissible levels of 2 fibres/ml in two of the factories. Source: www. nioh. org Asbestos Textile Industry: The average levels of air borne asbestos fibres varied from 216 -418 fibres/ ml. The permissible level is 2 fibres/ml. – The prevalence of asbestosis was 9%. This relatively low prevalence of asbestosis despite high environmental levels was attributed to high labour turn over. – Cases of asbestosis were observed in workers having less than 10 years exposure in contrast to the reported average duration of over 20 years. Source: www. nioh. org
 and")
ASBESTOSIS • • Asbestos Mining and Milling: – Done in Cuddapah (Andhra Pradesh) and Devgarh (Rajasthan). – In asbestos mines at both locations, the air borne fibre levels were within permissible limits. – The average fibre levels in milling units varied from 45 fibres/ml to 244 fibres/ml of air. – The overall prevalence of asbestosis in mining and milling units was 3% and 21% respectively. Source: www. nioh. org 19

Cut section of lungs in anthracosis On histopathological examination 20
 / Black lung disease: Ø Accumulation of coal dust")
Anthracosis/ Coal Worker's Pneumoconiosis (CWP) / Black lung disease: Ø Accumulation of coal dust in the lungs and Ø the tissue's reaction to its presence. Ø Associated with coal mining industry Ø Takes one or two decades to cause symptoms Ø The disease is divided into 2 categories: q • Simple CWP and q • Complicated CWP or Progressive Massive Fibrosis (PMF). q Simple Coal Worker's Pneumoconiosis: v Benign disease if no complications. v is associated with little ventilatory impairment Ø exist in the presence of radiological opacities < 1 cm in diameter. Ø This phase may require about 12 years of work exposure for its development Common symptoms 21 WP
")
Cont. …Simple CW P v Ø Ø Common symptoms: cough, expectoration (black in colour) and dyspnea. Slight decrease in FVC and FEV 1/FVC? ? Anthracosis first second of forced expiration (FEV 1) to the full, forced vital capacity (FVC). v Once a background of simple pneumoconiosis has been attained in the coal worker, a progressive massive fibrosis may develop out of it without further exposure to it. v From the epidemiological point of view, the risk of death among coal miners has been nearly twice that of the general population. Coal-miners' pneumoconiosis has been declared a notifiable disease in the Indian Mines Act of 1952, and also compensatable in the Workmen's Compensation (Amendment) Act of 1959 Complicated CWP
. Is diagnosed when")
Anthracosis q. Complicated Coal Worker's Pneumoconiosis or Progressive Massive Fibrosis (PMF). Is diagnosed when large opacity of 1 cm or more in diameter is observed in the CXR Pathologically it is characterized by large masses of black colour fibrous tissue nodular opacity. usually found posteriorly in upper lung zone. Ø Symptoms are similar but more severe Ø Recurrent pulmonary infection Ø The large lesions may cavitate as a result of ischemic necrosis or infection (T. B). Ø PFT (Pulmonary function test) reveals decreased FVC, FEV 1/FVC and increased residual volume. In a study conducted by National Institute of Occupational Health in collaboration with the International Development Research Centre (IDRC), Canada, (5777 underground coal miners and 1236 surface coal miners) –revealed that the prevalence of pneumoconiosis and functional abnormalities of lung in underground coal miners was 2. 84% and 45. 4% respectively, While in the surface coal workers it was 2. 10% and 42. 2% respectively. Source: www. nioh. org

Caplan's syndrome Cont. …Complicated CWP Anthracosis �Special type of PMF associated with rheumatoid disease (rheumatoid pneumoconiosis or Caplan's syndrome) occur and is characterized by typically smooth rounded nodules 0. 5 -5 cm in diameter which appear homogenous and well-defined on chest X ray �Nodules may grow, remain unchanged in size, resolve, or disappear and then reappear. They can cavitate, or calcify �Histologically, they usually have a necrotic center surrounded by a zone of plasma cells and lymphocytes, and often with a peripheral inflammatory zone made of macrophages and neutrophils �Caplan's syndrome presents with cough and shortness of breath in conjunction with features of rheumatoid arthritis, such as painful joints and morning stiffness. �Caplan’s syndrome only occurs in miners (especially those working in anthracite coal-mines), asbestosis, silicosis and other pneumoconioses �There is probably also a genetic predisposition, and smoking is thought to be an aggravating factor.


Preventive measures in Pneumoconiosis q Medical measures q Engineering measures q Other measures q Medical measures: Ø Pre-placement examination Ø Periodical examination Ø Medical and health care services Ø Notification Ø Maintenance and analysis of records Ø Health education and counselling Ø Practicing good personal hygiene Preventive measures v • Practicing good personal hygiene: § Washing hands and face before eating, drinking, going to the toilet, smoking. § Do not eat, drink, smoke, or apply cosmetics in areas where silica is being used. § Wear protective clothes and respiratory protection (Respirators must fit tightly) § Before leaving work, shower and change into clean clothes. § Leave dusty clothes at work. 29

q. Engineering Measures Ø Design of building Ø Conduct air monitoring to measure the workers’ exposure to crystalline silica. Ø Minimize exposures by controlling the creation of airborne particles, for example, use wet drilling, local exhaust ventilation. Ø Personal Protective Equipments: § Provide workers with protective clothes, respiratory protection, and facilities for washing (showers) and changing. § Enclosure / isolation § Environmental monitoring § Prohibit Dry Cutting Promote wet Cutting Preventive measures § Fume extractor system Labeling of products 30

q Other Measures: Ø Legal measures: Ø Measures to minimize dust emissions and exposure to dust. Ø Law compliance mechanisms, including effective workplace inspection systems Ø Cooperation between management and workers and their representatives Ø A mechanism for the collection and analysis of data on occupational diseases Ø Training of health professionals in occupational diseases as majority of medical practitioners lack training in occupational health and consequently lack the skills to diagnose and prevent occupational diseases. 31

Thank you

34

35

36
- Slides: 36