Pleural effusion Obeidah Masoudi MD FCCP American Board

Pleural effusion Obeidah Masoudi MD, FCCP American Board Pulmonary, Critical Care & Sleep Medicine Brown University.

• The pleura is the serous membrane that covers the lung parenchyma, the mediastinum, the diaphragm , and the rib cage. Divided into the visceral and the parietal pleura, both meet at the root of the lung, the pulmonary hilum forming the pulmonary ligament.
 Clear")
0. 1 to 0. 2 ml/kg Low protein(1. 0 to 1. 5 g/dl) Clear <1. 500 nucleated cells/micl (2%PMN, 0%Eios, 10%lymp, 70% macroph, mesothelial, and monocytes) • PH>7. 6 • •
. • Visceral")
• Parietal Pleura is supplied by the systemic circulation( intercostal vessels). • Visceral pleura is supplied by the bronchial circulation.

• Formation of the pleural fluid is a function of the parietal pleura , through the mesothelial junctions. • Resorption is a function of parietal pleura through stomata, lymphatic lacune, lymphatic ducts , lymphatic and mediastinal lymph nodes.

• Exudate results from pleural and lung inflammation or impaired lymphatic drainage of the pleural space. • Transudate is due to imbalance in the hydrostatic and oncotic pressure.

Light criteria Exudate ; • P/S protein ratio >0. 5 • P/S LDH ratio >0. 6 (PF LDH >45% of the upper limit of normal of serum LDH , a plural fluid protein >2. 9 g/d. L, or a PF cholesterol >45 mg/d. L had a diagnostic accuracy equivalent to light’s criteria and does not require a serum test)

transudative • • Congestive heart failure Hepatic hydrothorax Atelectasis Nephrotic syndrome Hypoalbuminemia Peritoneal dialysis urinothorax

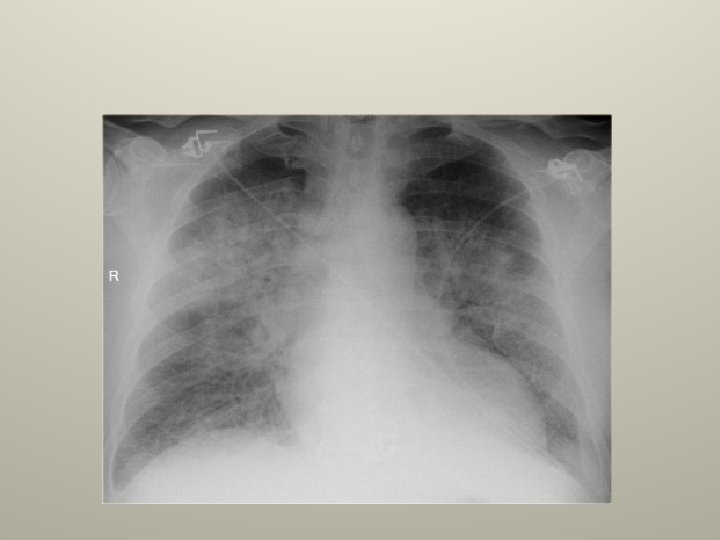
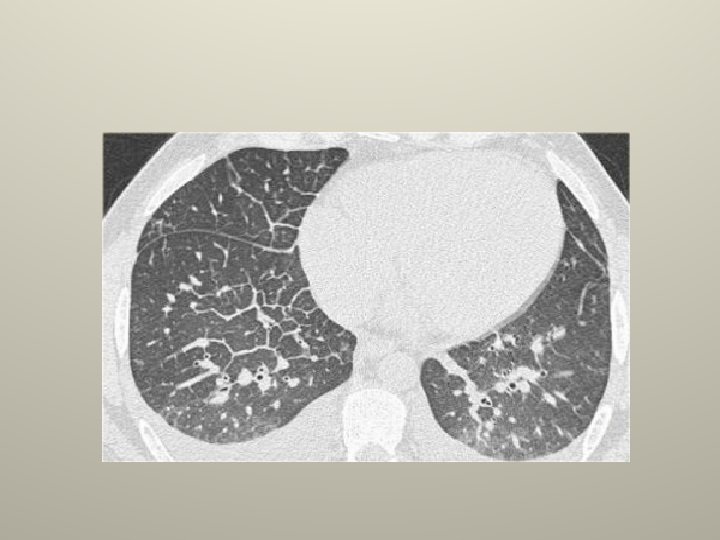
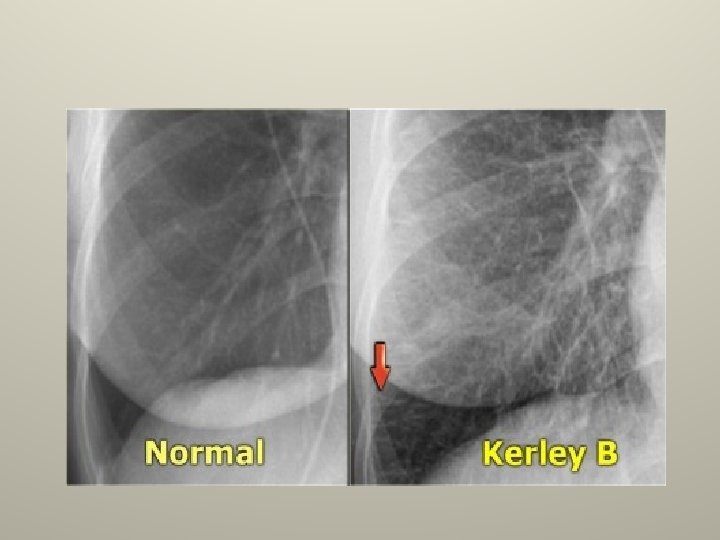
Congestive heart failure • The most common transudate. • Associated with pulmonary venous hypertension (PCWP>24). • Bilateral R>L, isolated Rt 8%, isolated Lt 4%. • Cardiomegaly, interstitial edema, kerley B lines on a CXR. • Treat heart failure , pleurodesis for refractarory effusions, bilateral pleurodesis is probably contraindicated.

Hepatic hydrothorax • 6% with cirrhosis and clinical ascites develop effusions. • Peritoneal>pleural pressure. • Small to moderate , Rt 70%, Lt 15%, bilateral 15% and massive 5% • Stigmata of cirrhosis with ascites, normal heart size on CXR, radionuclide scan confirmatory. • Rx ascites ; TIPS, VATS to patch diaphragm with pleurodesis, chest tube pleurodesis has low success. (chest tube drainage is contraindicated).

Nephrotic syndrome • 20% of nephrosis pt. • Decrease oncotic pressure +/- increase hydrostatic pressure. • Small bilateral frequently subpulmonic effusions. (cosider PE with pleuritic chest pain, or when effusion is larger on one side, hemorrhagic, or polymorphonuclear predominate ). • Treat underlying disease and prevent volume overload.

Exudates • • • • Parapneumonic effusions. Malignant effusions. Pulmonary embolism. Tuberculous pleurisy. Pancreatic diseases. Rheumatoid pleurisy. Lupus pleuritis. Post cardiac injury syndrome(PCIS). Chylothorax. LAM. Esophageal perforation. Benign asbestos effusion. Trapped lung. • • • Uremic pleural effusion. Yellow nail syndrome. AIDS. Hypothyroidism. Radiation therapy. Drug-induced pleural effusion.

Parapneumonic effusions • Most common exudative effusion , 40 to 57% of pt with bacterial pneumonia develops parapneumonic effusion , only a small percentage have complicated effusion , and only 5% develop empyema. • Uncomplicated • Complicated • Empyema.
 Exudative, (capillary leak) , 0 to 72 hrs 2) Fibrinopurulent")
Parapneumonic effusions Stages; 1) Exudative, (capillary leak) , 0 to 72 hrs 2) Fibrinopurulent ( bacterial invasion) , 3 to 10 days. 3) Organizational ( empyema), >2 weeks.

Most common organism causing empyema • • Anaerobe Staphylococcus. Gram negative aerobes. Pneumococcus.

Complicated effusions CXR/CT; • >40% of the hemithorax. • Intrapleural air fluid level. • Loculations. • thickening or enhancement of pleura on contract CT.

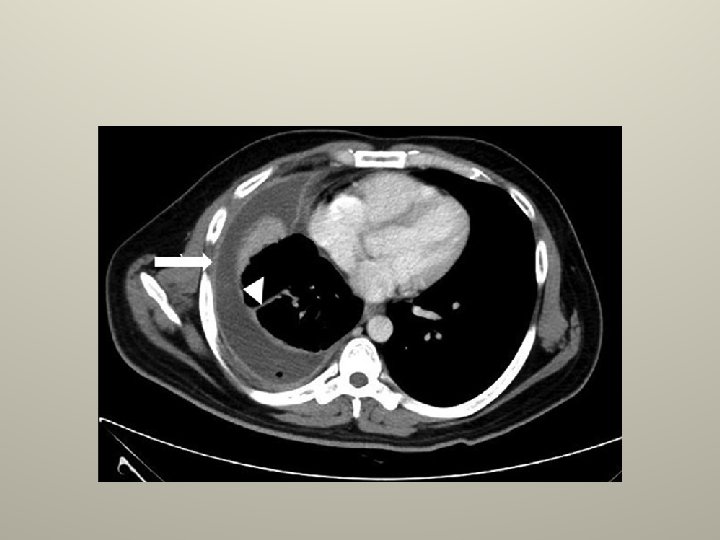

Complicated effusions PF analysis; • Gross pus. • Positive gram stain. • Positive bacterial culture. • Low PH , <7. 3 or <7. 2. • Low glucose. • High LDH.

Complicated effusions Treatment; • Uncomplicated; antibiotics directed at pneumonia. • Complicated; antibiotics and pleural fluid drainage.

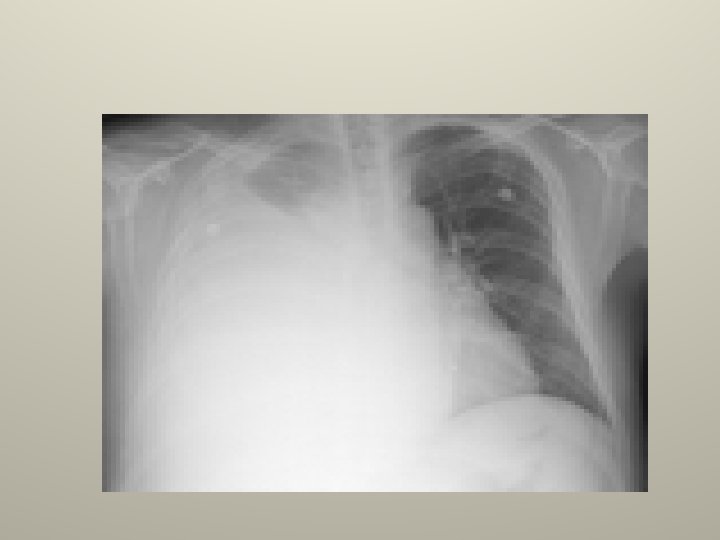
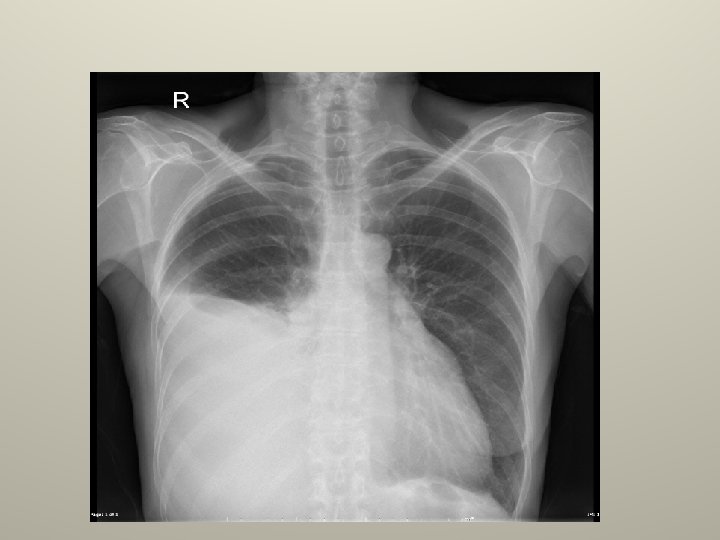
Malignant effusion • Second most common exudate • Lung and breast cancer represent 60% of all malignant effusions. • CXR ; massive effusion , without contralateral mediastinal shift , or bilateral effusion with normal heart size is all suggestive of malignancy.

Malignant effusion PF analysis; • Serous to bloody • 5% transudate • May be exudate by LDH only • Low PH and glucose associated with poor survival Diagnosis; • Cytology 45 to 90% • Pleural biopsy 40 to 50% • Thoracoscopy 95 to 100%

Malignant effusion Treatment; • For advanced disease with fluid acidosis and contralateral shift; chemical pleurodesis with talc poudrage or slurry , or doxycycline.

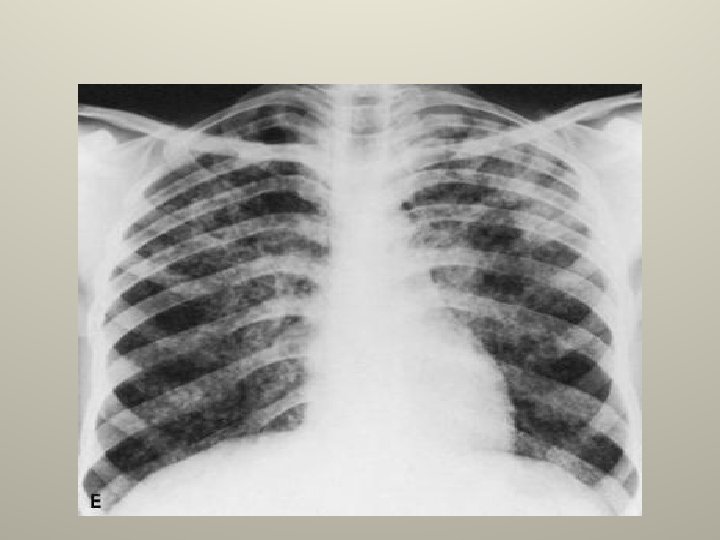
Tuberculous pleurisy • The common form of extra pulmonary tuberculosis. • CXR ; unilateral small to moderate , at times massive, more on the right side, underlying parenchymal infiltrate is seen in 33% on a CXR.



Tuberculous pleurisy PF analysis • Always exudative. • Serous , maybe serosanguinos, never frankly bloody. • Total protein >5 gm/dl. • 90% have more than 60% lymphocytes. • Eosinophilia and >5% mesothelial cells make TB unlikely. • Glucose < 60 mgldl and PH almost never above 7. 4 (in 20% 0 F PT <7. 3).

Tuberculouss pleuriy Diagnosis; • Pleural fluid AFB smear < 5% • Pleural fluid culture 13 -70% • Pleural Bx culture 55 -80% • Pleural Bx histology 66 -85% • PPD 50%+ve initiallly. • ADA adenosine deaminase >70 <40 • Interferon-Gamma>140 Pglml • PCR; S&P 81% and 100%

Tuberculouss pleuriy Treatment; • anti. TB drugs for 6 months(effusion clears in 4 6 weeks) • Steroids can increase rate of resolution • Undiagnosed lymphocytic predominant , exudative effusion in pt with +ve PPD must be Rx as TB.

• Thank You
- Slides: 36