Pleural Disease Dr Nadya Ben Geweref PLEURA Is

Pleural Disease Dr. Nadya Ben Geweref
 covers the lung (the visceral pleura); and")
PLEURA Is a serous membrane that: (i) covers the lung (the visceral pleura); and (ii) lines the thoracic cavity and mediastinum ( the parietal pleura).
 in pleural space.")
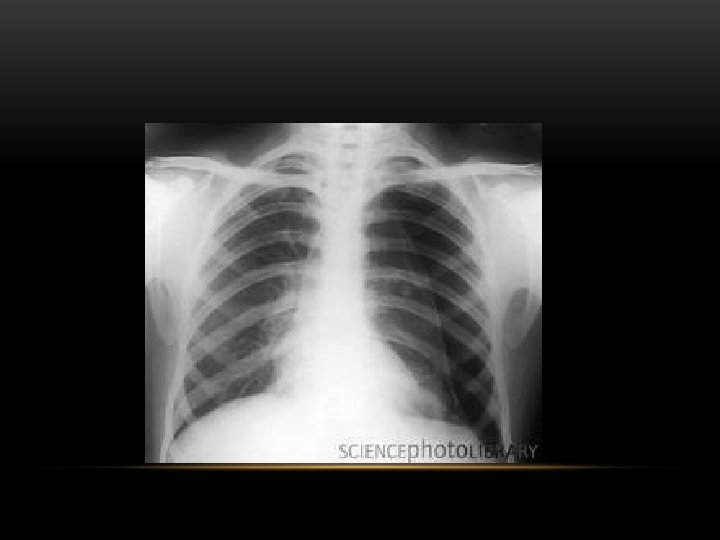
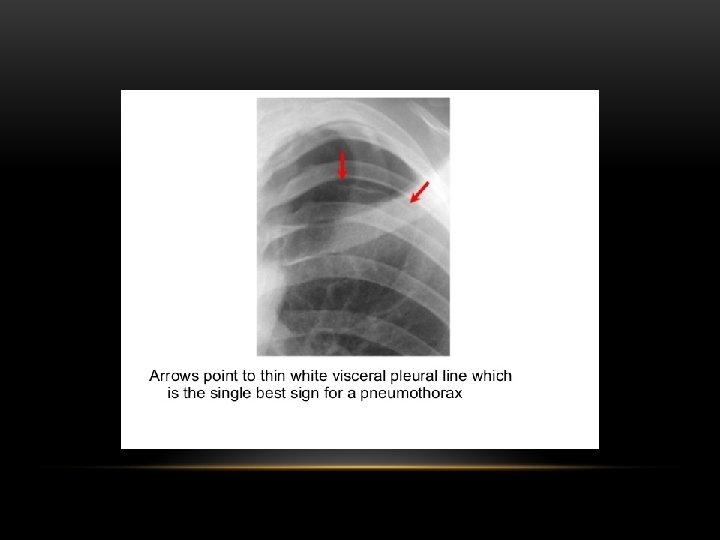
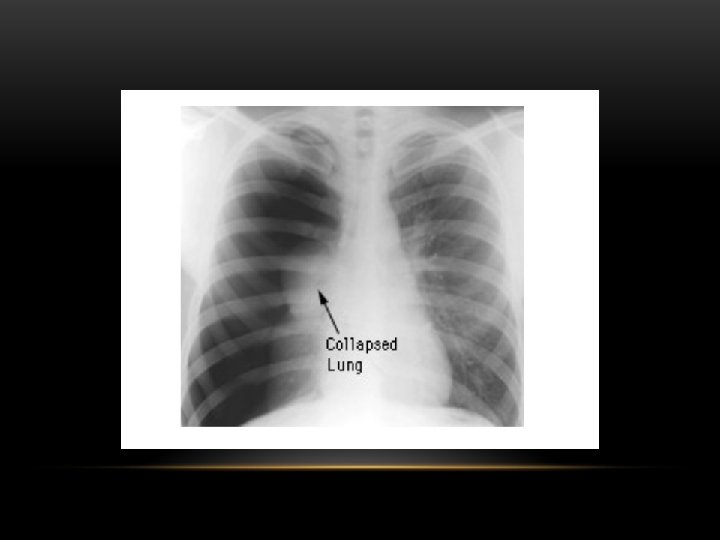
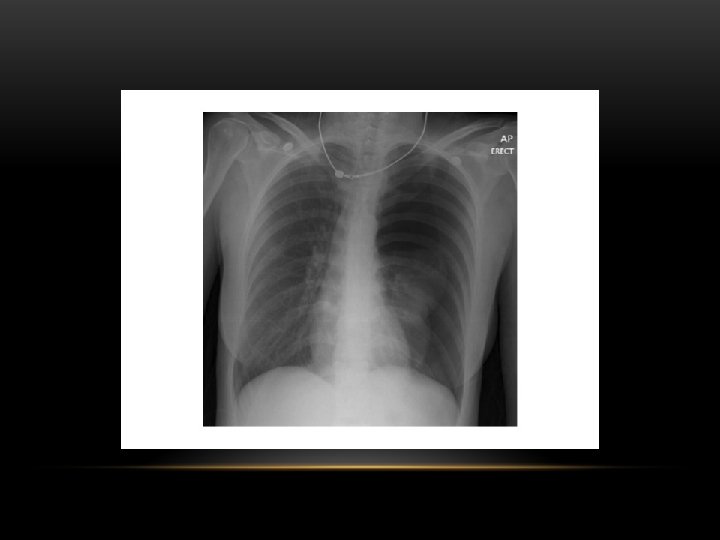
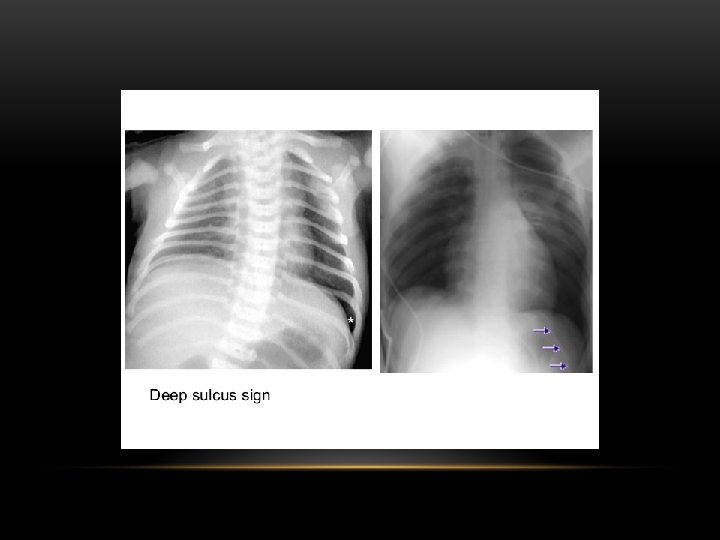
Pneumothorax is air in the pleural space. Radiological criteria: Air (black) in pleural space. No lung markings in pleural space. Recognition of atelectatic lung (lung margin). The lung recoils to a resting state as the negative pressure in the pleura is lost (relaxation atelectasis).

Shift of mediastinum to the opposite side. The mediastinum is held in the middle by balance between pleural pressures. When the negative pressure on the side of the pneumothorax is lost, the mediastinum gets pulled by the normal negative pressure from the opposite side. Progressive shift subsequently could result from a push secondary to tension pneumothorax. Opposite lung gets the entire cardiac output and the vascular markings become prominent.

Tension pneumothorax : is the progressive build-up of air within the pleural space, usually due to a lung laceration which allows air to escape into the pleural space but not to return. Positive pressure ventilation may exacerbate this 'one-way-valve' effect. Progressive build-up of pressure in the pleural space pushes the mediastinum to the opposite hemithorax, and obstructs venous return to the heart. This leads to circulatory instability and may result in traumatic arrest.

Causes of pneumothorax: -Burst small blebs o bullae. -Empyema -Trauma -Certain forms of interstitial pulmonary disease -Pneumocytosis carinii pneumonia -Metastasis (rarely)

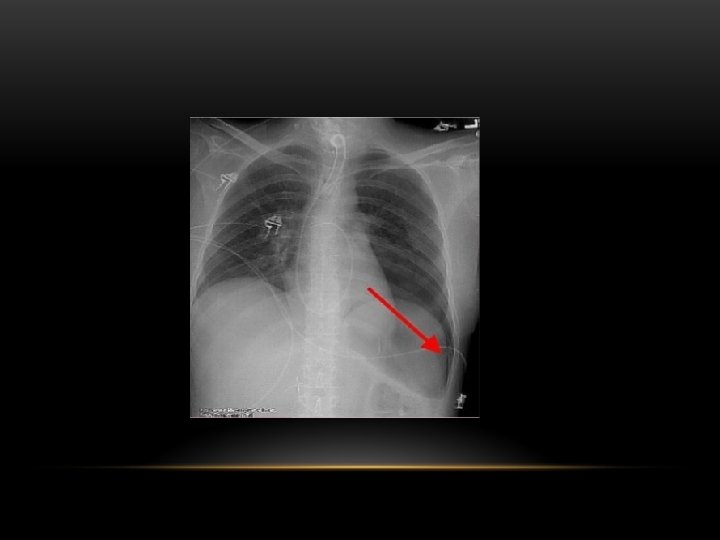
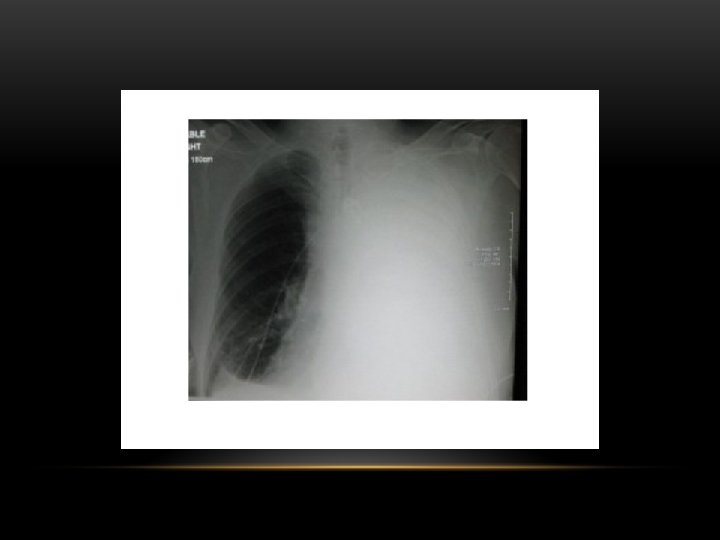
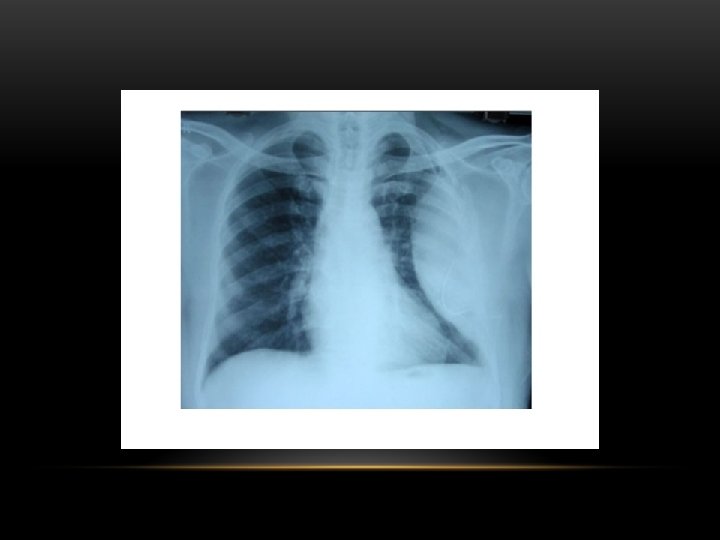
Pneumothorax • No vascular markings on right • No shift of mediastinum to left • Atelectasis right lung • Increased haziness on left: Diversion of entire cardiac output • Small fluid level near costophrenic angle: Hydro pneumothorax

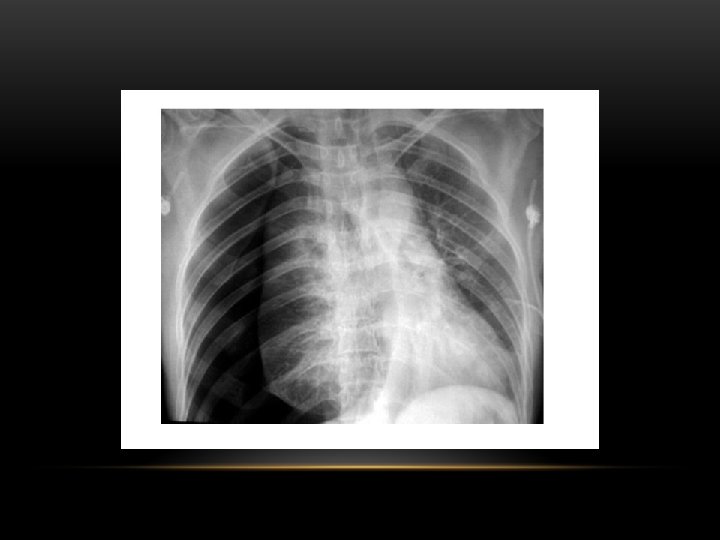
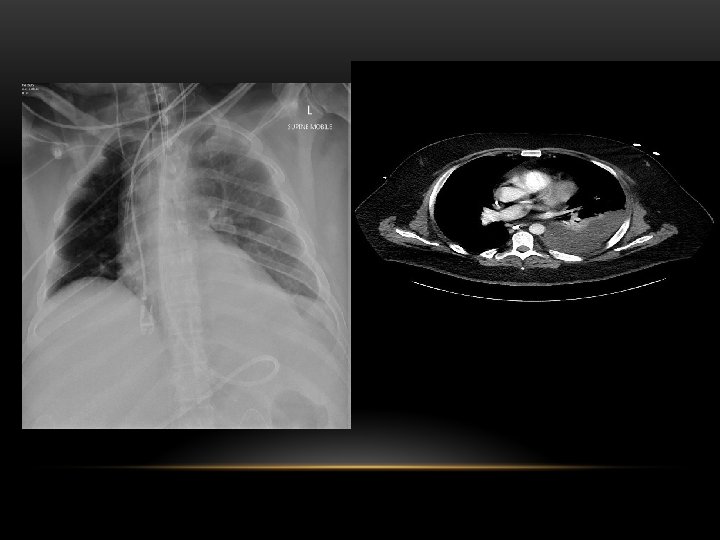
Tension Pneumothorax • No vascular markings on right • Shift of mediastinum to left • Atelectasis right lung • Increased haziness on left: Diversion of entire cardiac output

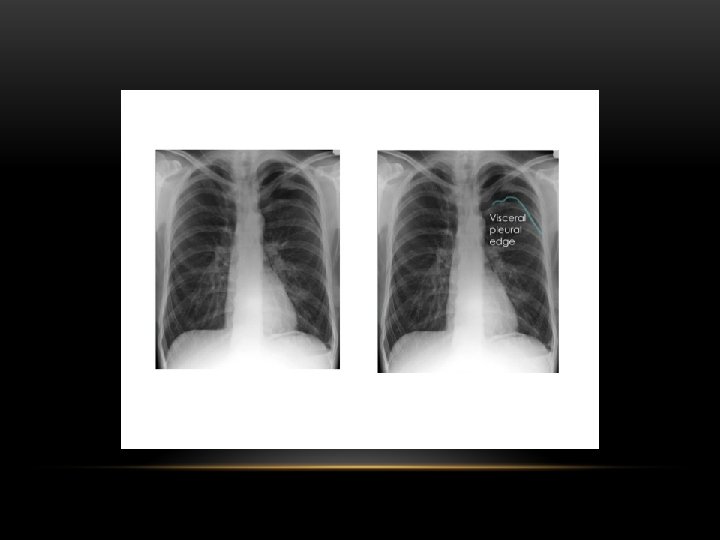
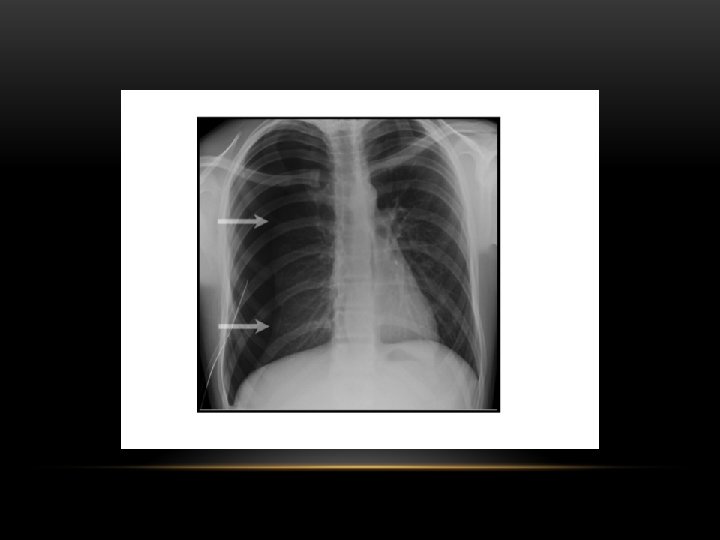
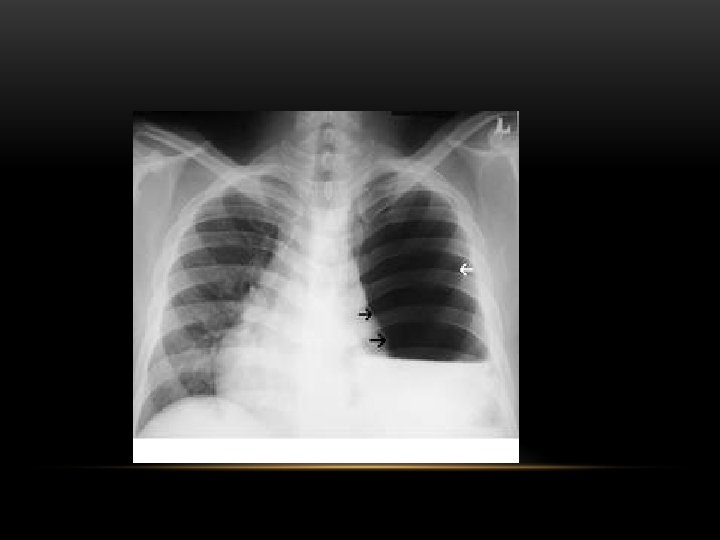
Spontaneous Pneumothorax • Air in pleural space • Lung margin • "Normal lungs": Note the radiolucency of atelectatic lung is the same as the opposite lung

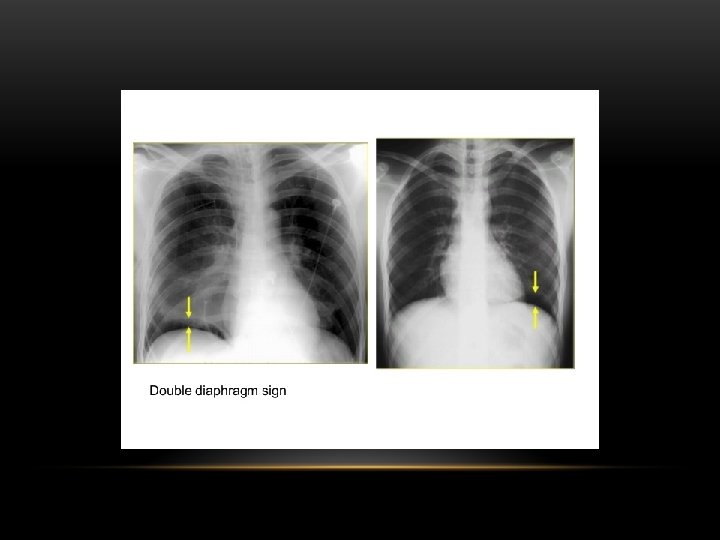
Inspiratory Expiratory

Hydropneumothorax

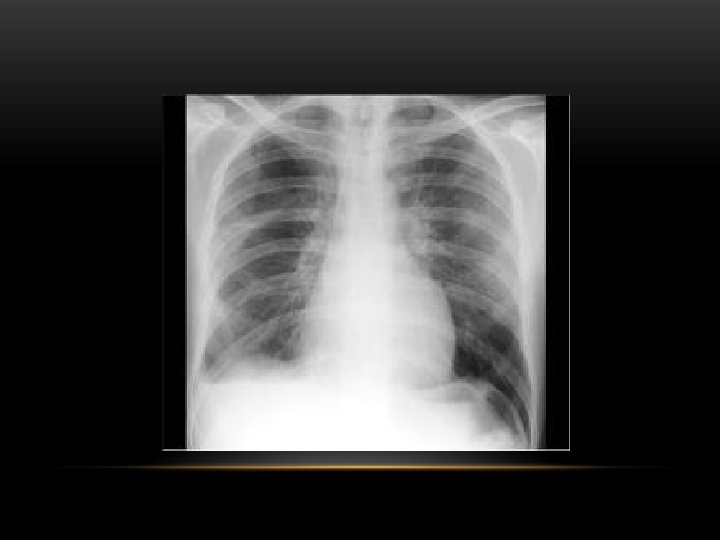
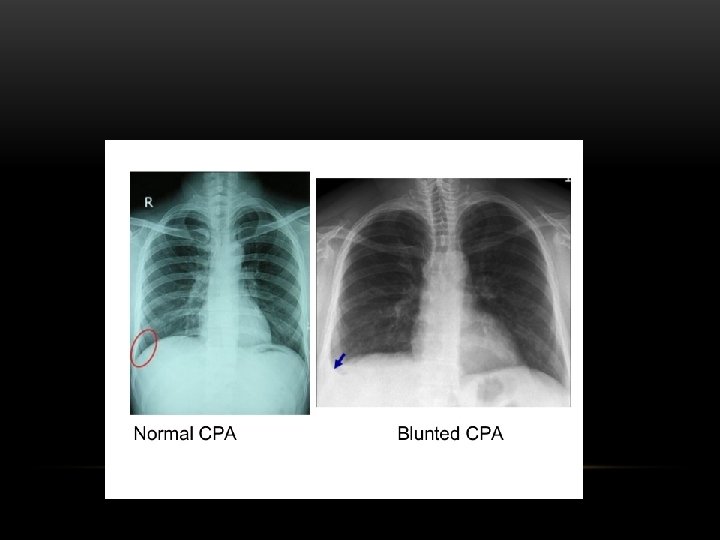
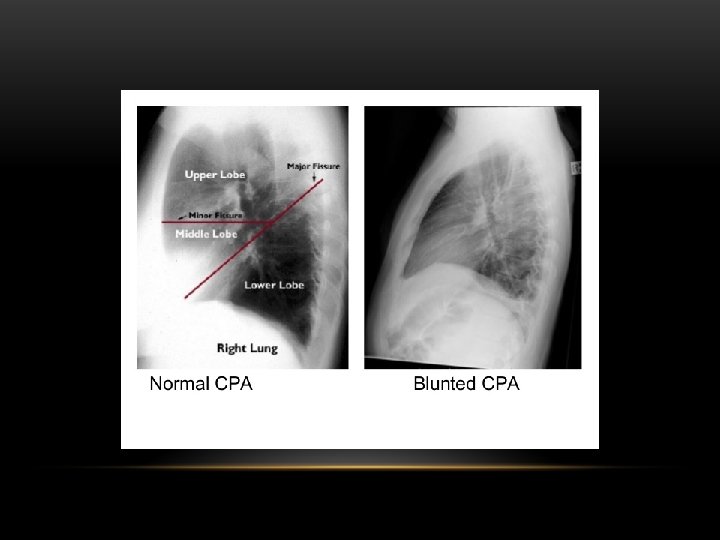
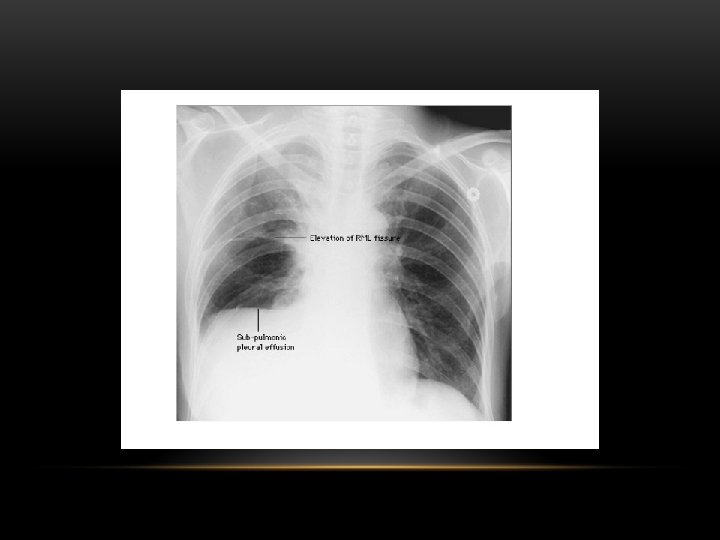
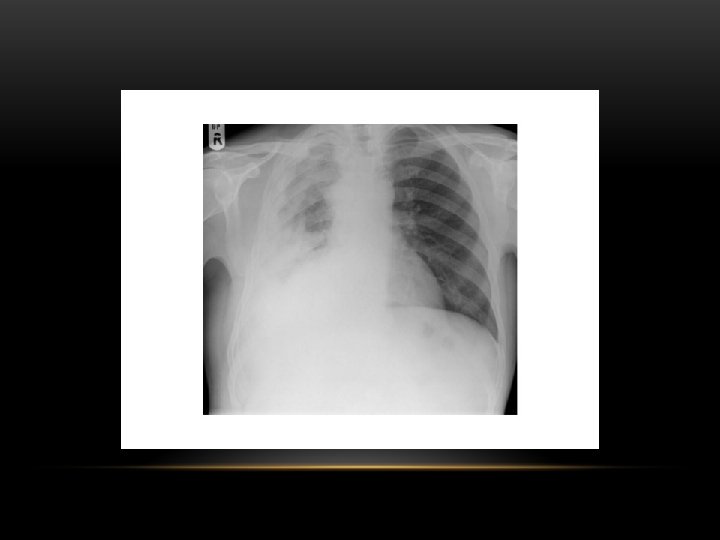
Pleural Effusion Fluid accumulates in the pleural space. Irrespective of the nature of fluid, radiologically they will look similar. Radiological criteria are: Density In dependent portion (Costophrenic angle in PA view). Blunting of costophrenic angle Lack of identifiable diaphragm (silhouette sign principle).

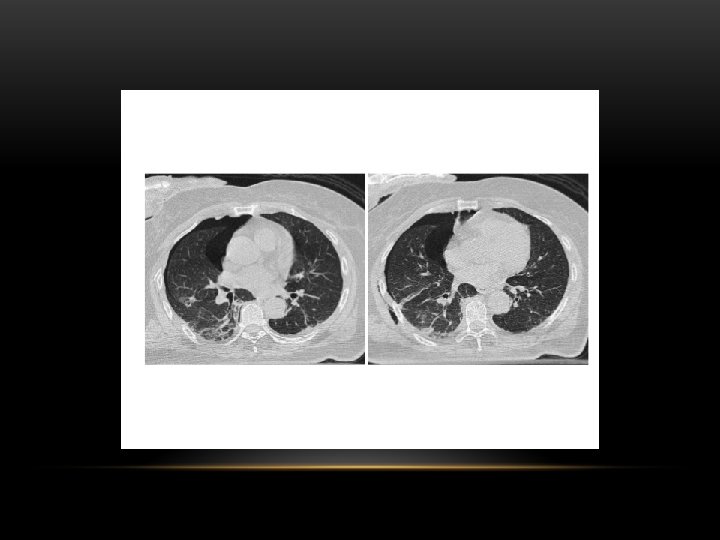
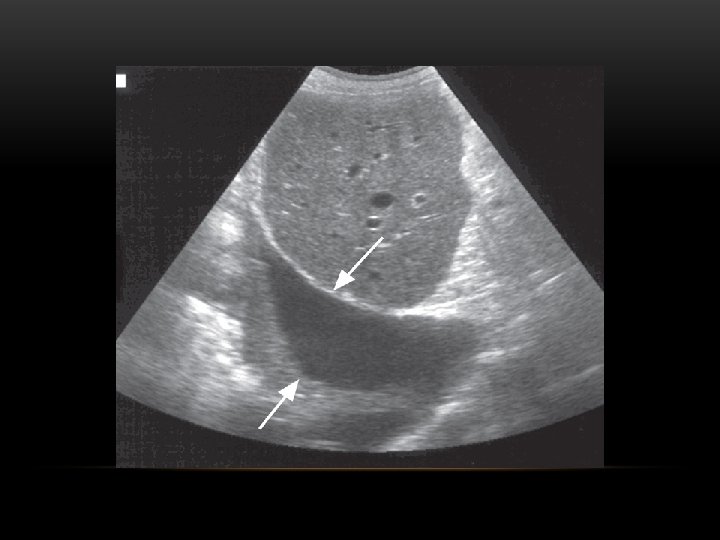
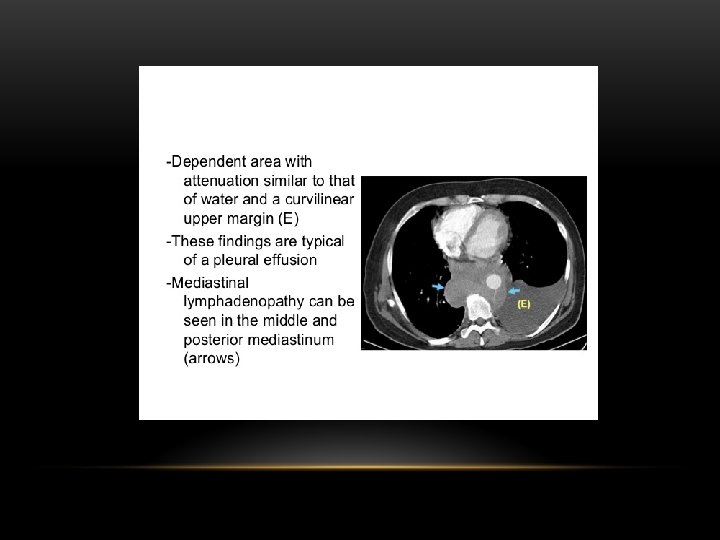
Causes of pleural effusion: -Infection -Subphrenic abscess. -Malignant neoplasm -Cardiac failure -Pulmonary infarction -Collagen vascular disease -Nephrotic syndrom Modalities for pl. effusion diagnosis: -Plain chest x ray. -Ultrasound -Computed tomography


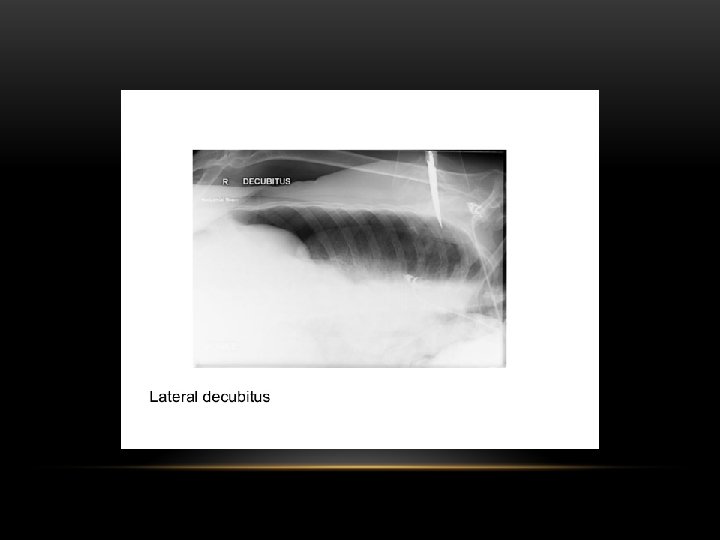
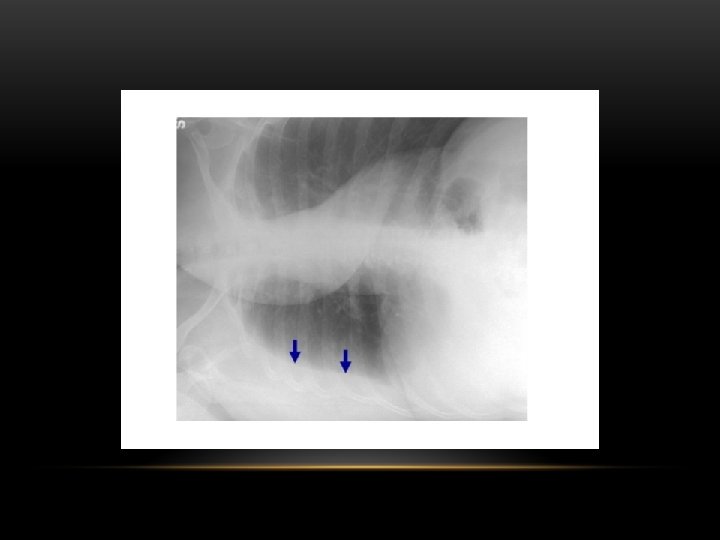
Lateral Decubitus : Most sensitive, may detect as little as 25 m. L

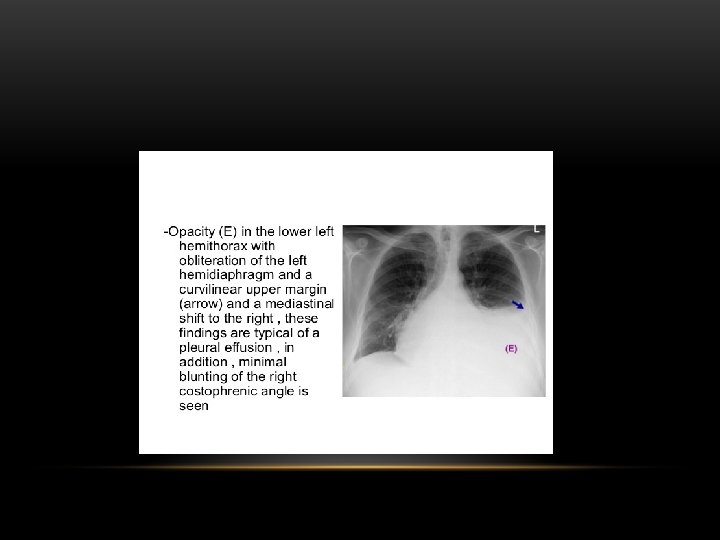


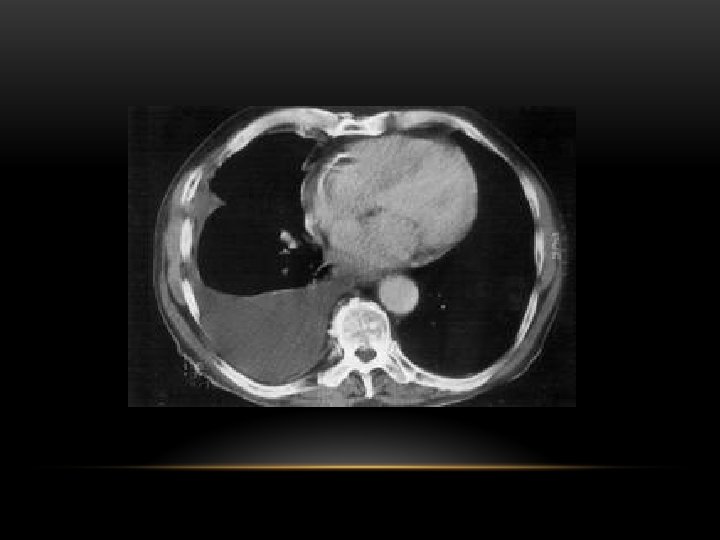
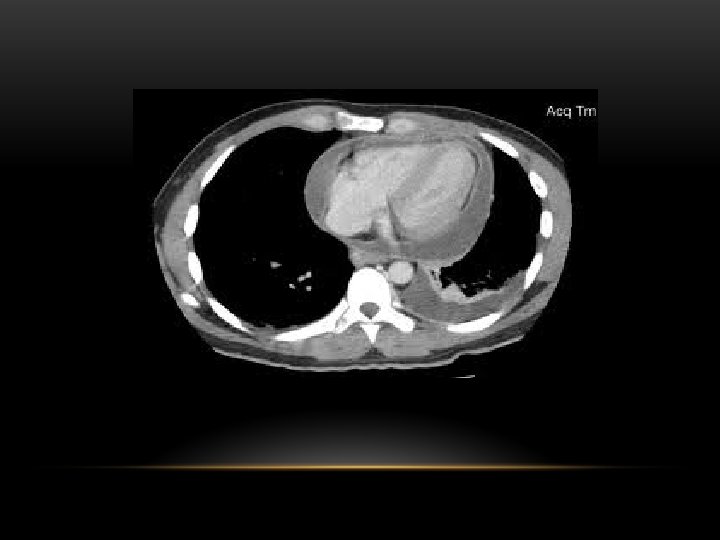
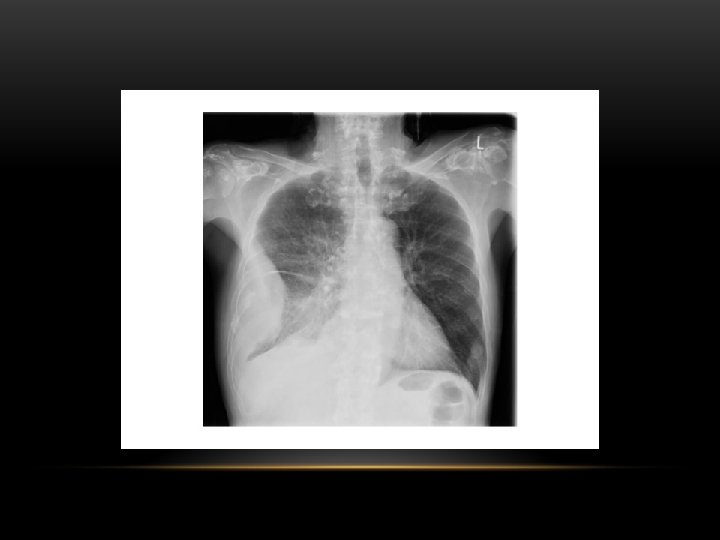
Pleural Effusion • Homogenous density • Loss of cardiophrenic angle • Loss of diaphragmatic and right cardiac silhouette

Supine projection erect projection

Hemothorax


CT scan of left empyema with pleural enhancement

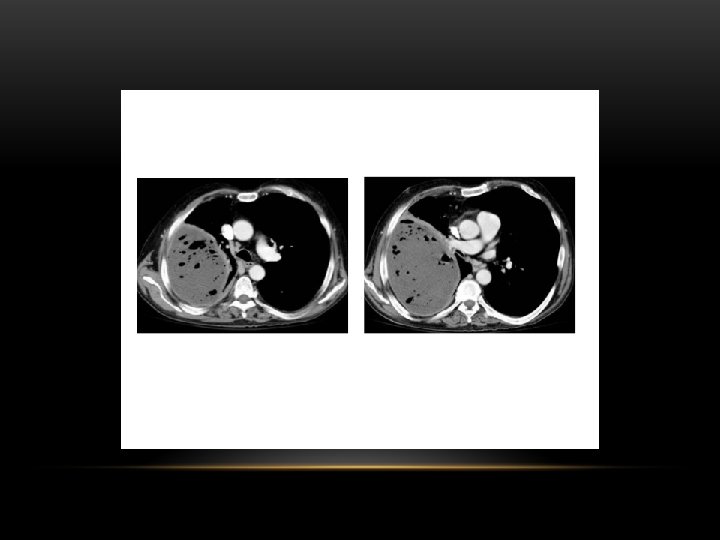

loculated pleural effusion


Pleural Fibrosis Diffuse haziness Apical cap thickening Blunting of costophrenic angle Loss of lung volume

Pleural Fibrosis • Small right hemithorax • Diffuse haziness • Blunted costophrenic angle

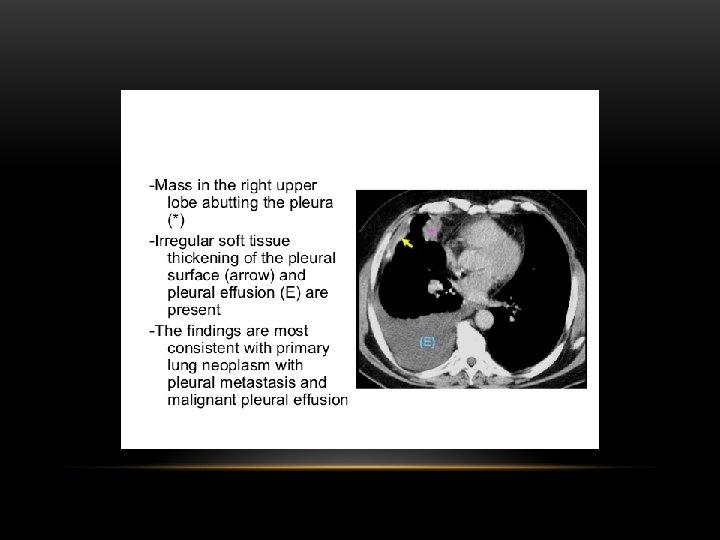
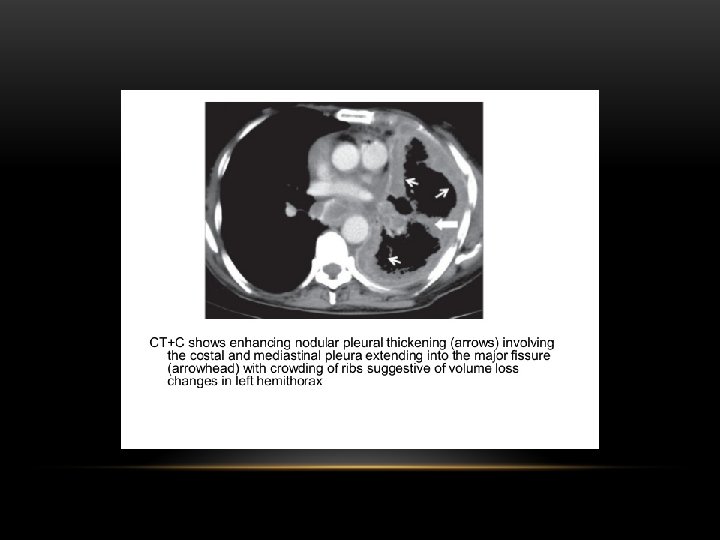
pleural masses Multiple • Pleural metastases. • Asbestos related pleural disease: Look for calcifications. • Malignant mesothelioma. Solitary • Pleural metastases: • Solitary fibrous tumor of the pleura. • Lipoma. • Malignant mesothelioma:

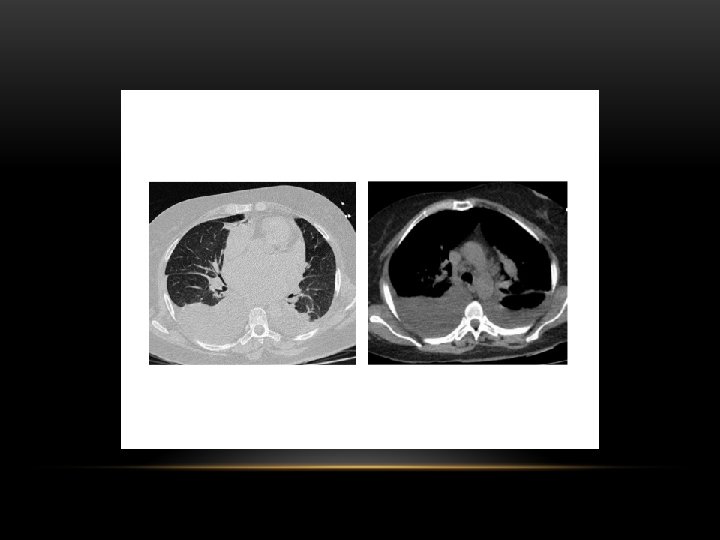
Multiple pulmonary, and pleural metastasis

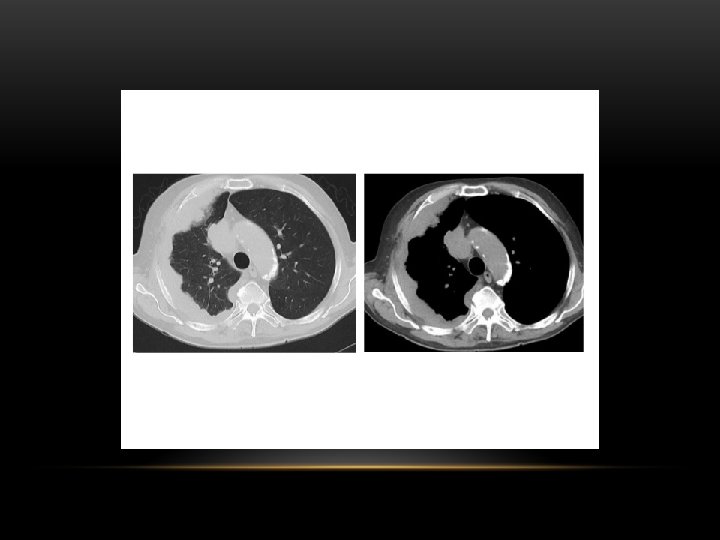
Mesothelioma

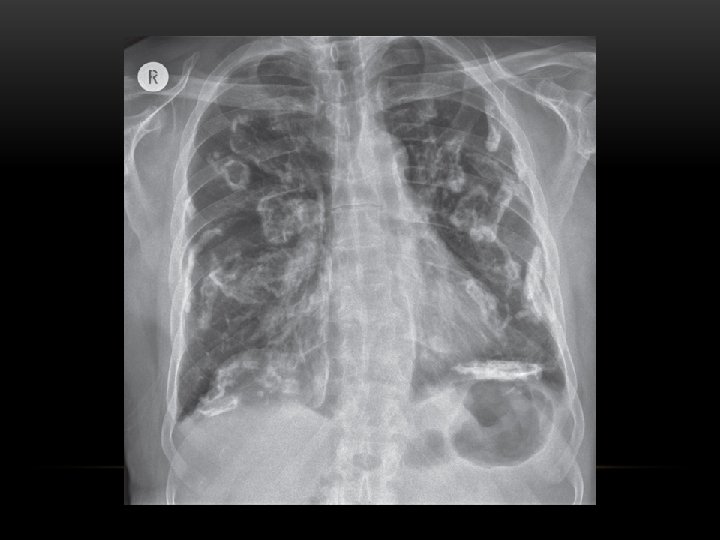
Pleural calcification: Pleural calcification can result from many causes • calcified pleural plaque from asbestos exposure : typically has sparing of costophernic angles • previous haemothorax • previous infection involving the pleura : e. g pyothorax • tuberculous pleuritis

Calcified tuberculous empyema. Axial CT scan of the chest

Pleural calcification occurs in about 50% with asbestos

Thank you
- Slides: 75