Platelet role in Hemostasis Peyman Eshghi Prof of







: • tortuous invaginations of the as an internal")



 isoprostenoid Vasodilation")


: • Membrane")


 • Gray platelet syndrome (GPS)")


 on platelets inhibit")
 • 3 families:")




 is liberated from the sn-2 position of membrane")

















- Slides: 56
Platelet role in Hemostasis Peyman Eshghi Prof. of Pediatric Hematology &Oncology Pediatric Congenital Hematologic Disorder Research Center Mofid Children Hospital , Shahid Beheshti University of Medical Sciences Iranian Society of Thrombosis and Hemostasis (IRSTH) P_eshghi@sbmu. ac. ir Tehran 7 -96
History • From Nothing particle in 1881: "piastrine" in Italian ; "blutpliittchen“ in German and "petites plaques" in French publications To • The most important particle –platelet- in 2017 : Hemostasis; fibrinolysis ; thrombosis ; vascular remodeling; vascular tone ; wound repair; participation in cardiovascular disease, stroke, and even cancer; etc……
PLATELET MORPHOLOGY AND SUBCELLULAR ORGANIZATION
• Small, disc-shaped cellular fragments: 1. 5 µm in diameter and 0. 5 to 1 µm in thickness; and 6 -10 f. L in volume: • 150, 000 to 300, 000/µL • Proplatelets are Not a simple cytoplasmic fragmentation of megakaryocytes BUT are assembled and packaged at the ends of long cytoplasmic extensions of differentiated megakaryocytes after migration from the proliferative osteoblastic niche to the capillary-rich vascular niche of BM : • Size is regulated by non-muscle myosin heavy chain IIA (MYHIIA) and the cell surface glycoprotein Ib (GPlb) • Younger Platelets are larger and contain more m-RNA than older
http: //www. platelet-research. org/1/function_morpho. htm#
• Inner zone structure • Of the two types of granules found in the platelet cytoplasm, the majority are of the alpha type • Glycogen is for energy storage
• Moving outward from the organelle zone, we come to the solgel zone • Single rigid, but dynamic microtubule approximately 100 µm in length that is coiled about 8 to 12 times around the equatorial plane of the cell : maintains the circulating discoid shape • Secondary system of microfilaments which, during the contractile phase, maintains internal organization and secretion.
• Open Canalicular system (OCS): • tortuous invaginations of the as an internal reservoir of plasma membrane • extend lamellipods and filopods to increase the surface area of exposed plasma membrane by more than 400%. • conduit for the rapid expulsion of alpha (mostly located inner ) and dense granule contents • Dense tubular system (DTS): • remnant of the smooth endoplasmic reticulum(dense granules) • dispersed throughout the cytoplasm • Site of Arachidonic acid metabolism • harbor high concentrations of calcium, as Sarcoplasmic/endoplasmic reticulum Ca 2+ ATPase 2 b(SERCA 2 -b) • Ca can be released by platelet agonists : ADP, Thrombin (via binding to the platelet thrombin receptor PAR 1)
• Exterior coat or glycocalyx as a “plasmatic atmosphere” contains : • plasma proteins, • glycoprotein binding sites (receptors) and • carbohydrate molecules related to the complement, coagulation, and fibrinolytic systems
Discoid Platelet Early dendritic Platelet Early spread Platelet
ANTITHROMBOTIC COMPONENTS OF THE VESSEL WALL
COX-1 heparinlike glycosa minoglyc ans TXA 2 platelet Gs protein-coupled receptor (GPCR) isoprostenoid Vasodilation AMP ADP Vaconstriction protein kinase A Inhibit platelet adhesion and aggregation and impeding platelet-mediated recruitment of leukocytes during the inflammatory response
Subendothelial matrix: platelet adhesion and activation
1. Tethering: • VWF interacts with a high-affinity, platelet-specific multisubunit receptor known as the GPIb/V/IX complex 1 3 3 2. Initial signaling to the cell interior: • GPIb acts through membrane-proximal Src family kinases • Immunoreceptor Tyrosine-based Activation Motif (ITAM) 3. Integrin-mediated adhesion, • ἀ2β 1 integrin binds to exposed collagen fibrils • ἀ6β 1 integrin receptor engages laminin. 4. GPVI activation: • Cytoskeletally directed cell spreading • Inside-out Signal transduction • Granule secretion via OCS 4 2 2 Phosphopholipase Cy 2 3
Platelet Granules and Their Contents • ALPHA GRANULES (40 -80 per cell): • Membrane proteins enriched in the granule membrane: • P selectin, TLT-l, CD 40 ligand (which is cleaved after exposure on the platelet surface to release soluble CD 40 L), and. tissue factor(TF) • Membrane proteins present at similar concentrations as they are in the plasma membrane: • GPIIb-IIIa, GPlb, PECAM-l, and perhaps many others • Granule contents: • Synthesized by megakaryocytes: • Thrombospondin, VWF, platelet factor 4, β -thromboglobulin, PDGF • Endocytosed from plasma or origin not determined: • Albumin, fibrinogen, fibronectin, Ig. G, Gas 6 , coagulation factor V, and many chemokines and growth factors, including RANTES, b. FGF, EGF, TGF β, and VEGF • DENSE GRANULES (4 -8 - pr cell) • Vasoconstrictors: ADP, ATP, 5'-HT, Ca 2+, polyphosphate, serotonin • LYSOSOMES • Acid hydrolases, elastase, cathepsins, and other degradative enzymes
• Exposed P-selectin : the most diagnostic of an activated platelet serves to recruit leukocytes to the site of injury, one of a number of important links between thrombosis and inflammation. • VWF, Fibrinogen: support platelet-platelet interactions; • chemokines and growth factors, including RANTES, b. FGF, EGF, TGF β, and VEGF : promote cell migration and wound healing and maintain vascular integrity. • Autocrine factors [such as growth arrest specific gene 6 (Gas 6) and CD 40 L]which are released and rebind platelet receptors to help amplify platelet responsiveness.
• Platelet factor-4: • binds with high affinity to heparin. • Its major physiologic role appears to be neutralization of heparin-like molecules on the endothelial surface of blood vessels, thereby inhibiting local antithrombin III activity and promoting coagulation. • As a strong chemoattractant for neutrophils, fibroblasts and monocytes: has a role in inflammation and wound repair. • HIT • Malaria
Inherited disorders of platelet granules: Storage pool disorders (SPD) • Gray platelet syndrome (GPS) : • Platelet alpha granules, or at least their contents, are severely reduced • Mild bleeding • Dense granule defects: • platelets lack dense granules or their contents especially ADP which play physiologically important role in hemostasis: • Mild to moderate bleeding associated with other problems: • Immunodeficiency: Chediak-Higashi • Albinism: Hermansky-Pudlak
Acquired dysfunction of platelet granules: synthesis and secretion • Drug: such as (nonsteroidal anti-inflammatory drugs), dipyridamole, clofibrate, and dextrans • Foods and supplements: (Vitamin E, caffeine, , ginger, fish oil, ethanol, garlic and onions) • Uremia • Cirrhosis • Leukemia • Plasma protein abnormalities • Myeloproliferative disorders • Cardiopulmonary Bypass
AMPLIFICATION PATHWAYS INVOLVED IN PLATELET RECRUITMENT
Ga inhibitory protein-coupled receptors/Ligands Ticlopidine and Clopidogrel • Gai protein-coupled receptors(GPCR) on platelets inhibit adenylate cyclase and lower cyclic adenosine monophosphate (c. AMP) levels. • the ability of the SERCA 2 b calcium pump to sequester cytosolic calcium ions is impaired • More available cytosole Ca 2+ allowing calcium-mediated activation events to occur more readily. • Ticlopidine and Clopidogrel: antagonize the activity of P 2 Y 12
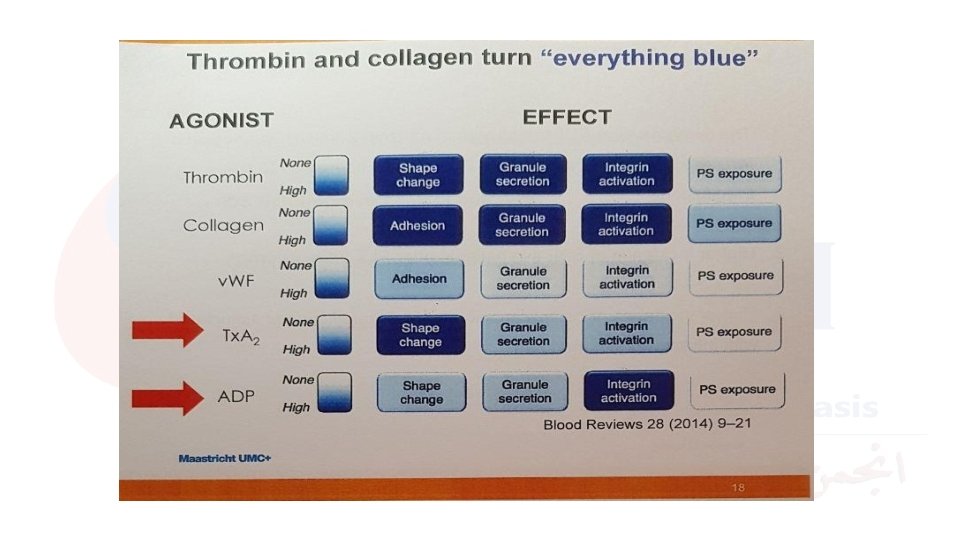
Other Agonist receptors in signal amplification Immunoreceptor Tyrosine-based Activation Motif (ITAM) • 3 families: • Gq-coupled GPCRs: P 2 Y 12; PARI and PAR 4, TXA 2 R, 5 HTR • Integrins: α 1 bΒ 3, α 6Β 1, α 1Β 1 • Receptor tyrosine kinases (RTKs). • Each activates either the β and γ isoform of phospholipase C (PLC). • The sum total of PLC-generated products serves to determine the activation state of the platelet, its ability to respond to vascular injury, and its participation in thrombus growth. α 1 bΒ 3 α 6Β 1 α 1Β 1
• Platelet responses to thrombin are primarily mediated through G-protein -coupled protease-activated receptors (GPCRs OR PARs). • Thrombin mediates platelet activation via two PARs: PAR-1 and PAR-4. • PAR-1 is the major human platelet receptor, exhibiting 10– 100 -times higher affinity for thrombin when compared with PAR-4
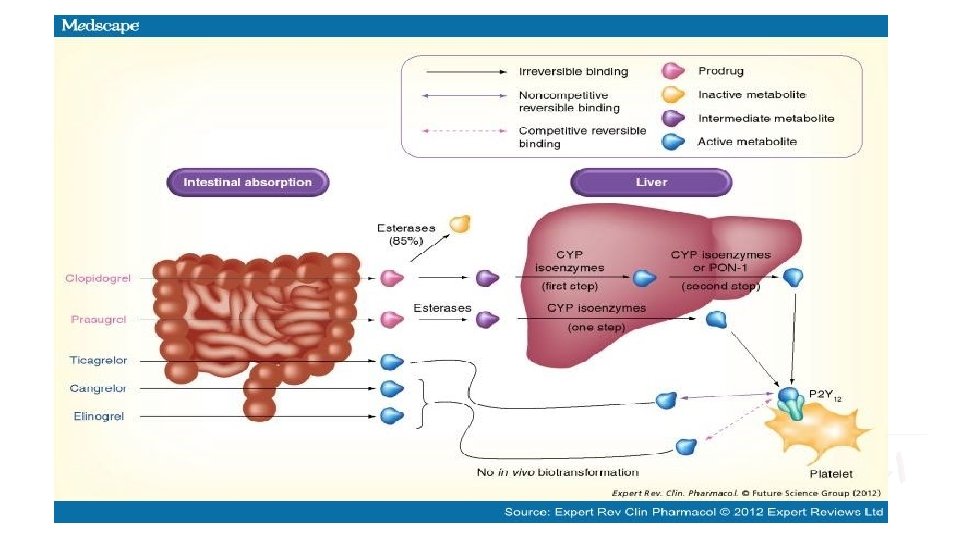
Anti-aggregants http: //www. medscape. com/viewarticle/764760_6 ?
GPIIb/IIIa complex Antagonists • Since fibrinogen binding to the activated receptor GPIIb/IIIa constitutes the final common pathway of platelet aggregation, GPIIb/IIIa antagonists inhibit platelet aggregation independently of the type of platelet agonist Integrin activation by PLCs
• Abciximab : • is a noncompetitive irreversible inhibitor of GPIIb/IIIa. • crossreacts with other integrins on the surface of various cell types • Induces immune response as a humanized chimeric Fab fragment of the monoclonal mouse antibody 7 E 3. • Eptifibatide and Tirofiban: • are low-molecular-weight competitive and reversible GPIIb/IIIa antagonists that • act specifically on the αIIb-subunit of GPIIb/IIIa • cannot induce immune response • Owing to their short plasma half-lives, continuous infusion is needed for sustained platelet inhibition.
Cyclooxygenase-1 Inhibitors • Arachidonic acid (AA) is liberated from the sn-2 position of membrane phospholipids by cytosolic PLA 2. AA is then converted to the unstable intermediates prostaglandin G 2/H 2. • • COX-1: Cyclooxygenase-1; HOX: Hydroperoxidase; PGG 2: Prostaglandin G 2; PGH 2: Prostaglandin H 2; PGI 2: Prostaglandin I 2; PLA 2: Phospholipase A 2; Tx. A 2: Thromboxane A 2.
• Aspirin: • Irreversible activity for the remaining lifespan of the platelet, namely 7– 10 days. • up to 30% of circulating platelets (new PLTs)may show normal Tx. A 2 production after aspirin discontinued for 48 h • in low doses aspirin does not affect the action of endothelial cell COX-1 and therefore does not reduce the production of PGI 2, which has many beneficial effects including potent antiplatelet effects. • low aspirin dose (75 mg/day) could be the treatment of choice for maintenance therapy in all patients following ACS • Aspirin resistance may be seen in 5 -65% of patients: • • • high plasmatic activities of kallikrein low compliance, interference with NSAIDs and protein glycation occurring in Type 2 diabetes mellitus. Increased platelet turnover COX-2 enzyme in inflammatory cells single-nucleotide polymorphisms within PTGS 1 and biochemical resistance (Less than 1% ) • Triflusal • reduces the incidence of intracranial and gastrointestinal hemorrhage • well tolerated in patients with aspirin-induced asthma
Phosphodiesterase Inhibitors • Dipyridamole and cilostazol are inhibitors of PDE, an enzyme that catalyzes the hydrolysis of the cyclic nucleotides c. AMP and c. GMP.
P 2 Y 12 Receptor Antagonists • The decrease in c. AMP intracellular levels reduces the rate of phosphorylation of VASP, thus inducing activation of the GPIIb/IIIa receptor and platelet aggregation. • AC: Adenyl cyclase; • PLC: Phospholipase C; • VASP: Vasodilator-stimulated phosphoprotein; • VASP-P: Vasodilator-stimulated phosphoprotein phosphorylation.
• Clopidogrel also exerts anti-inflammatory effects, including a reduction in serum C-reactive protein levels as well as a decrease in platelet leukocyte conjugates, P-selectin and CD 40 L membrane expression, and platelet microparticle formation • the maximum efficacy is observed 4– 5 days after daily administration of 75 mg clopidogrel due to its need for metabolic activation: thus a 600 -mg loading dose is recommended • Clopidogrel resistance or clopidogrel hyporesponsiveness(interindividual variability) in one-third of clopidogrel-treated patients: • ABCB 1 C 3435 TSNP significantly reduces clopidogrel absorption in both the homozygous and heterozygous form. • loss-of function CYP 2 C 19 alleles (*2, *3, *4, *5, *6, *7 and *8), especially the CYP 2 C 19*2 allele, in both heterozygotes and homozygotes • Poor compliance to treatment is an important cause • Obese or diabetic patients • Proton pump inhibitors (PPIs) are protective against gastrointestinal complications; however, may attenuate clopidogrel responsiveness when used concomitantly
• How to overcome probable resistance: • Tailored treatment with clopidogrel in the daily clinical practice based on platelet function test • Genetic testing before starting clopidogrel therapy in high-risk patients • Drug interactions: • concurrent clopidogrel and PPI use appears safe, but coprescription is recommended only for patients at risk for gastrointestinal complications. [45] • Clopidogrel's antiplatelet effectiveness is not influenced by atorvastatin and other lipophilic statines[48] • there is no overall significant difference between each salts of clopidegrol (bisulfates Or besylates)in their antiplatelet effects, safety and clinical benefit of alone or in combination with aspirin http: //www. medscape. com/viewarticle/764760_3(references 42 -56)
Key Issues • The combined use of antiplatelet drugs acting through different mechanisms is important in antithrombotic treatment of patients with cardiovascular disease. • The improvement of our knowledge on the pharmacodynamics of antiplatelet drugs enables the tailoring of the most appropriate antithrombotic therapy to the individual patient and risk situation in daily clinical practice. • It is questionable whether individualized antiplatelet therapy should be based on genetic testing, platelet function testing or both. The results of ongoing largescale outcome studies, are needed before their routine application into clinical practice. • The new P 2 Y 12 antagonists, prasugrel and ticagrelor, are characterized by more potent antiplatelet effects and reduce recurrent ischemic event rates compared with clopidogrel among acute coronary syndrome patients. However, the potential benefits associated in terms of reduction of ischemic events need to be kept in perspective with known bleeding complications. • Novel potent and selective platelet inhibitors exhibit high antithrombotic efficiencies but their clinical efficacy in preventing major adverse cardiovascular events remains to be established.
CELL SURFACE AND CYTOSOLIC PROTEINS THAT LIMIT PLATELET RESPONSES • Regulator of GPCR • Immunoreceptor Tyrosin-based inhibitory motif (ITIM) receptors: • PECAM-1 • CEACAM-1 • G 6 b-B • Protein Kinase B (PKB)
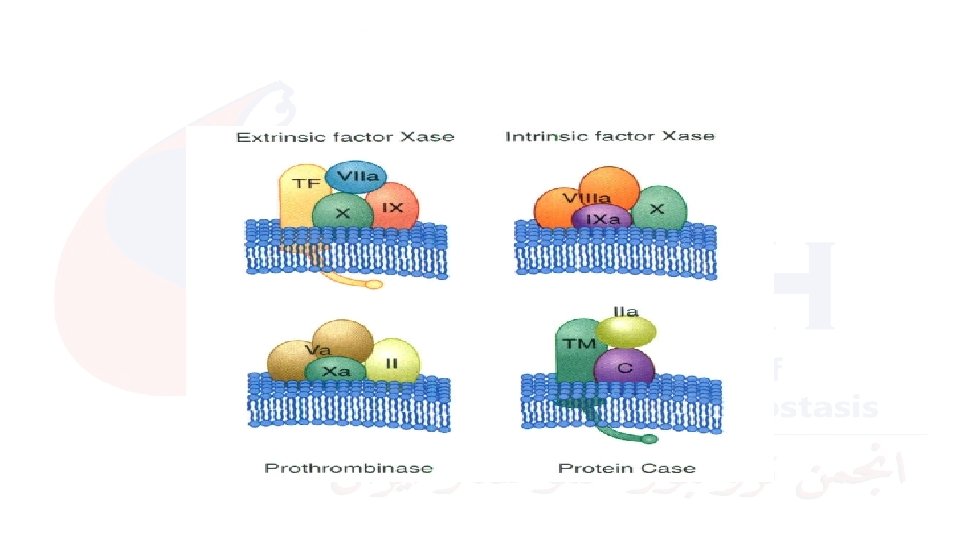
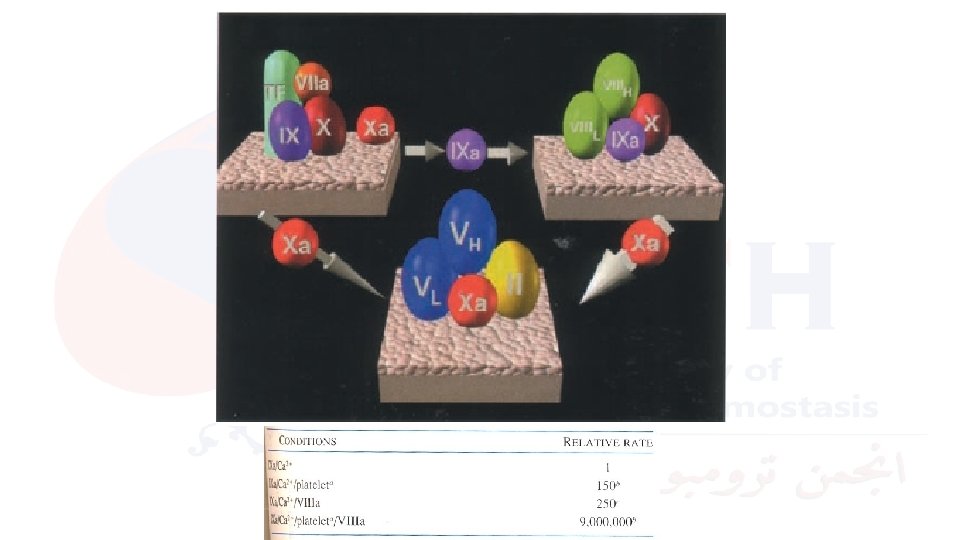
New, Cell Based Coagulation Model modified from Hoffman & Monroe, Thromb Haemost 2001; 85: 958 -965 VIIa TF TF-Bearing Cell TF VIIa
New, Cell Based Coagulation Model X VIIa TF Xa TF-Bearing Cell Initiation TF VIIa
New, Cell Based Coagulation Model II X VIIa TF Xa TF-Bearing Cell Initiation TF VIIa Va IIa
New, Cell Based Coagulation Model II X VIII / VWF VIIa TF TF VIIIa Platelet VIIa V XIa Activated Platelet Amplification IIa Va TF-Bearing Cell Initiation XI Xa Va
New, Cell Based Coagulation Model II X VIII / VWF VIIa TF TF IXa XIa IX Amplification IIa Va VIIIa TF-Bearing Cell Initiation XI Xa Platelet VIIa V IX Propagation IXa VIIIa Activated Platelet Va
New, Cell Based Coagulation Model II X VIII / VWF VIIa TF Xa TF IX Amplification VIIIa Platelet VIIa V IX IXa XIa Va TF-Bearing Cell Initiation XI IIa X IXa Propagation Xa VIIIa Activated Platelet Va
New, Cell Based Coagulation Model II X VIII / VWF VIIa TF Xa TF IX Amplification VIIIa Platelet VIIa X IXa Va V IX IXa XIa Va TF-Bearing Cell Initiation XI IIa II Xa VIIIa Activated Platelet Va Propagation IIa Clot formation
Normal Haemostasis II X TF IX VIIa TF IXa XIa IX VIIa Xa Va IIa TF-bearing cell II X VIIIa IXa VIII/v. WF Xa activated platelet VIIIa V Va XI XIa platelet Va IIa
ADDITIONAL ROLES FOR PLATELETS IN VASCULAR PHYSIOLOGY • leukocyte trafficking and inflammation: • P-selectin/PSGL-1 interaction • P-selectin expressed on cytokine-activated endothelial cells • platelet P-selectin • Proinflammatory chemokines role in development of atherosclerosis: • chemoattraction of leukocytes • stimulating proliferation of vessel wall smooth muscle cells and fibroblasts. • IL-1β : potent stimulator of endothelial cells and monocytes that upregulates adhesion molecule expression • Degradative enzymes • Growth-promoting factors : • • • Vascularendothelial growth factor (VEGF), PDGF, Fibroblast growth factor (FGF) Epidermal growth factor (EGF), Angiopoietin 1
Questions