Platelet Aggregation Inhibitors Professor Dr MAHMOUD KHATTAB The

Platelet Aggregation Inhibitors Professor. Dr. MAHMOUD KHATTAB,

The components of a platelet
 shape change (b) secretion")
Platelet Aggregation n Activated platelets undergo three consecutive processes: (a) shape change (b) secretion of platelet granular contents (ADP, fibrinogen & 5 HT) (c) platelet aggregation Platelet aggregation occurs when the receptor (GP IIb/IIIa) binds to fibrinogen GP IIb/IIIa platelet fibrinogen platelet There is 50, 000 GP IIb/IIIa receptors on the surface of each platelet
 Collagen thrombin Activation of G-protein TXA")
Platelet Aggregation ADP Thromboxane a 2 (TXA 2) Collagen thrombin Activation of G-protein TXA 2 Arachidonic acid GP IIb/IIIa undergoes insideout (exposed on the surface of platelet) The receptor binds to fibrinogen COX enzyme TXA 2 • Then TXA 2 acts on its own receptor (act as a positive feedback mediator) • It also has vasoconstriction effect

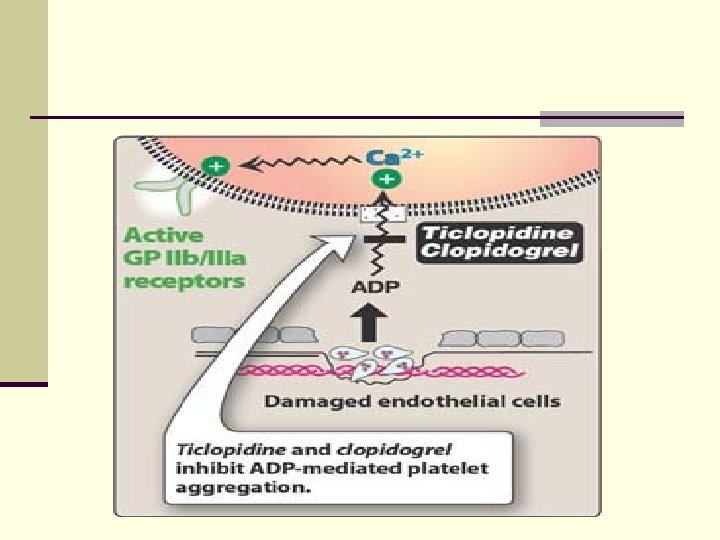
ADP n Stored ADP released and acts on its own receptor(positive feedback mediator n ADP activates Gi-coupled P 2 Y 12 receptors. n ADP-ADP receptor complex c. AMP IIb/IIIa exposed GP GP IIb/IIIa It binds to arginine – glycine – asparagine sequence (R – G – D) in fibrinogen molecule or in Von Willebrand factor (v. Wf).
 Fibrinogen mimetics (Tirofiban) TXA 2 receptor TXA")
Overview of antiplatelet drugs Glycoprotein receptor (IIb/IIIa) Fibrinogen mimetics (Tirofiban) TXA 2 receptor TXA 2 antagonist (Ridogril) COX inhibitor (Aspirin) 2 - antibody (Abciximab) ADP receptor blocker Gb IIb/IIIa receptor blocker 1 - (R-G-D) mimetics

Mechanism of action of Aspirin N. B. Aspirin inhibits Thromboxane A 2 & prostacyclin too, but the former is more affected because platelets don’t have nuclei can’t synthesize new enzymes TXA 2 remains low for 7 days (platelet lifespan)

I- ASPIRIN n After oral intake, this action is apparently occurring in the portal circulation (more action in portal circulation than systemic circulation) Low dose antiplatelet (80 -160 mg) Aspirin High dose analgesic, antipyretic, , ,

Uses & adverse effect Uses Prophylaxis against unstable angina Adverse effects GI -ulceration Post MI Prolonged bleeding time ↑ risk of hemorrhage Post stroke Can not be used in child suffering from viral infection N. B. these are dose dependent

Aspirin Antiplatelet Efficacy 1 - Dose n Most authorities recommend initial therapy with a dose of 160 mg (one half-tablet) to 325 mg (one adult tablet) n Aspirin should be crushed/chewed (to facilitate faster absorption by breaking the enteric-coated delayed release tablet)

Aspirin Antiplatelet Efficacy A. Efficacy of aspirin in patients with unstable angina q Reduces morbid ischemic events B. Efficacy of aspirin in patients following acute MI q Reduces nonfatal MI and nonfatal stroke C. Reduce morbidity and mortality in stroke patients

II- Glycoprotein IIb/IIIa Receptor Antagonists 1 - Glycoprotein IIb/IIIa murine-derived 7 E 3 Fab monoclonal antibody (Abciximab) n Abciximab is composed of 7 E 3 Fab fragments. n derived from murine (mouse) n Abcixi(m)ab (m): monoclonal antibody. n directed against glycoprotein receptor type GPIIb/IIIa. n Mechanism: The m 7 E 3 Fab binds selectively to the glycoprotein GPIIb/IIIa receptors inhibiting platelet aggregation (see next slide)
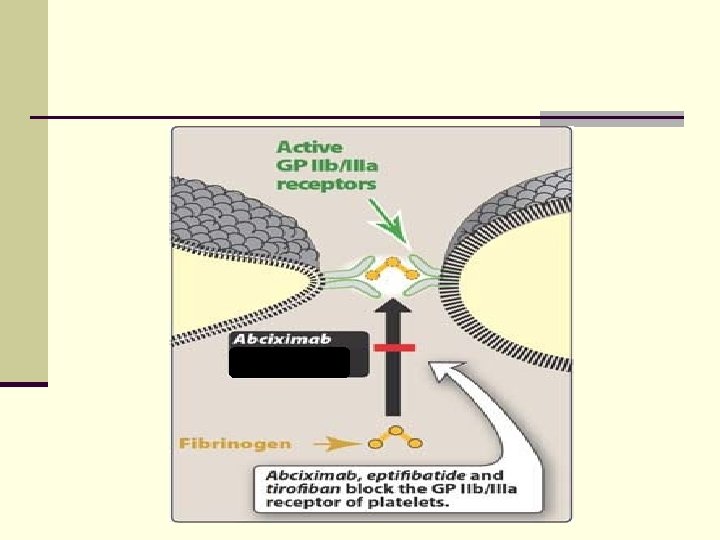

II- Glycoprotein IIb/IIIa Receptor Antagonists 1 - Glycoprotein IIb/IIIa murine-derived 7 E 3 Fab monoclonal antibody (Abciximab) q Administration and therapeutic use: in angioplasty surgery to prevent ischemic complication (taken IV) o Heparin or aspirin are given along with abciximab
 sequence mimetics")
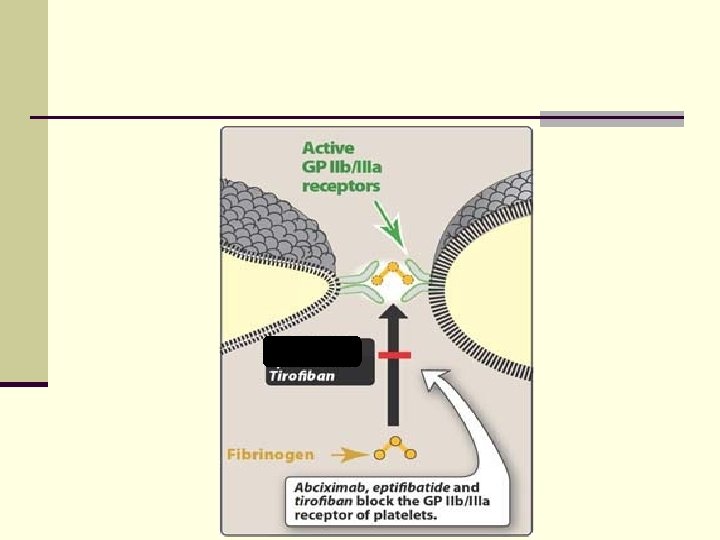
II- Glycoprotein IIb/IIIa Receptor Antagonists 2 - Synthetic arginine-glycine-aspartic acid (R -G-D) sequence mimetics n Tirofiban (non-peptic) is a synthetic mimetic of the R-G-D sequence of fibrinogen n Hence, it blocks the binding of fibrinogen to glycoprotein GPIIb/IIIa receptors n They are given intravenously for the reduction of thrombotic complications during coronary angioplasty (if they are given orally they are toxic) n Clinical trials showed reductions in the incidence of death and non-fatal MI in response to the use of tirofiban.

III- Thromboxane Antagonists q Ridogrel is a combined thromboxane synthase inhibitor and thromboxane A 2 (TXA 2) receptor antagonist, orally active q It has no effect on the vascular production of prostacyclin but cyclic endoperoxides (PGH 2) may increase q It decreases recurrent ischemic events e. g. (angina, reinfarction, ischemic stroke) more than aspirin. q Used in aspirin intolerant patients.
 Ticlopidine & Clopidogrel Ø They inhibit irreversibly ADP")
IV- Platelet ADP Receptor Antagonists (Thienopyridines) Ticlopidine & Clopidogrel Ø They inhibit irreversibly ADP binding to receptors inhibit platelet aggregation Ø No effect on PG synthesis Ø Used in aspirin intolerant patients

ADVERSE EFFECTS q. Ticlopidine is associated with more side effects than Clopidogrel. Ticlopidine Clopidogrel Nausea, dyspepsia, diarrhea (20% of patients) Same Hemorrhage (5%) same Leukopenia in 1% of patients (most serious). (N. B. monitor WBC in the first 3 months of treatment) same Thrombotic thrombocytopenic purpura Same fatal neutropenia nothing

Antiplatelet Drugs drug mechanism

THING TO REMEMBER … n Glycoprotein IIb/IIIa: GP IIb/IIIa Antagonists Antibody tirofiban abciximab n Aspirin: • Inhibits COX 1 enzyme TXA 2 • Is beneficial in prophylaxis of unstable angina and pre/postmyocardial infarction. • Aspirin may cause gastric ulcers and hemorrhage.

THINGS TO REMEMBER … n Ridogrel: • Is TXA 2 synthetase inhibitor and TXA 2 receptor antagonist. n Ticlopidine and clopidogrel: • Bind irreversibly to ADP receptors inhibiting the activation of GP IIb/IIIa. • They are only used in aspirin-intolerant patients because of adverse side effects

TXA 2 Prostacyclin Aspirin ↓↓↓ ↓ Ridogril ↓↓ Zero Ticlopidine, clopidogrel Zero Remember: TXA 2: increases platelet aggregation and vasoconstrictor Prostacyclin: decreases platelet aggregation and vasodilator
- Slides: 24