PLASMAPHERESIS By Dr Mohamed Abd El Gawad Nephrology

PLASMAPHERESIS By Dr. Mohamed Abd El Gawad Nephrology Specialist at New Mansoura General Hospital

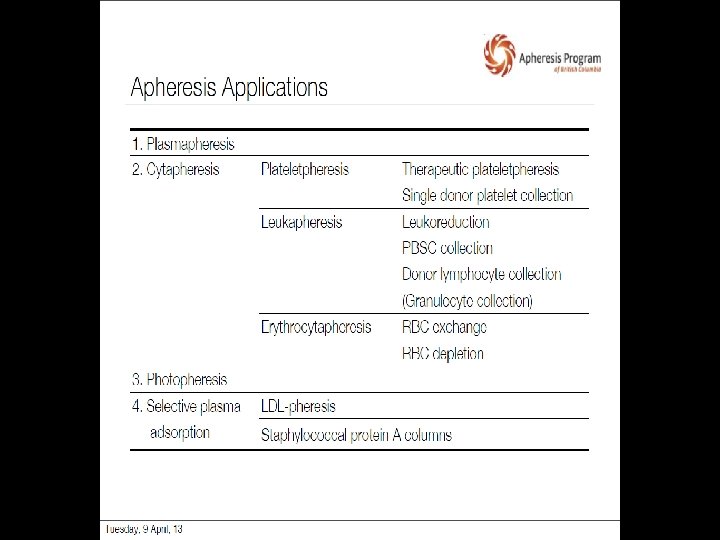
Agenda q What is Plasmapheresis ? q INDICATIONS FOR PLASMAPHERESIS q TECHNIQUES q Replacement fluid q Vascular access q Anticoagulation q Regimens of PE q Complications

? What is Plasmapheresis

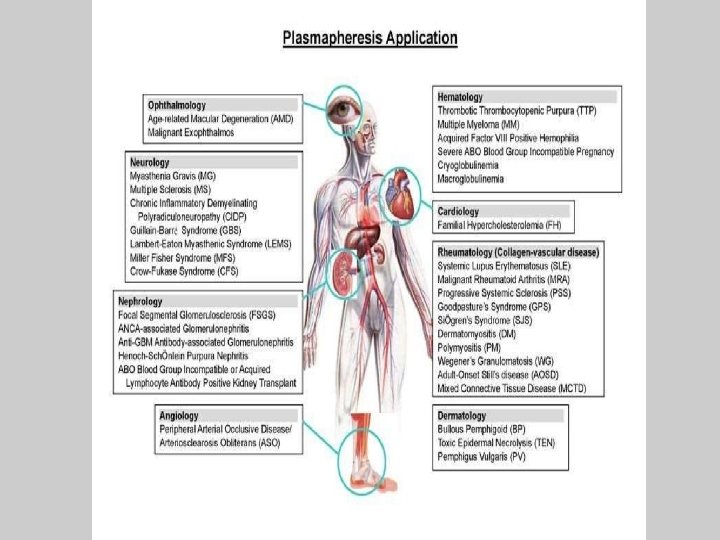
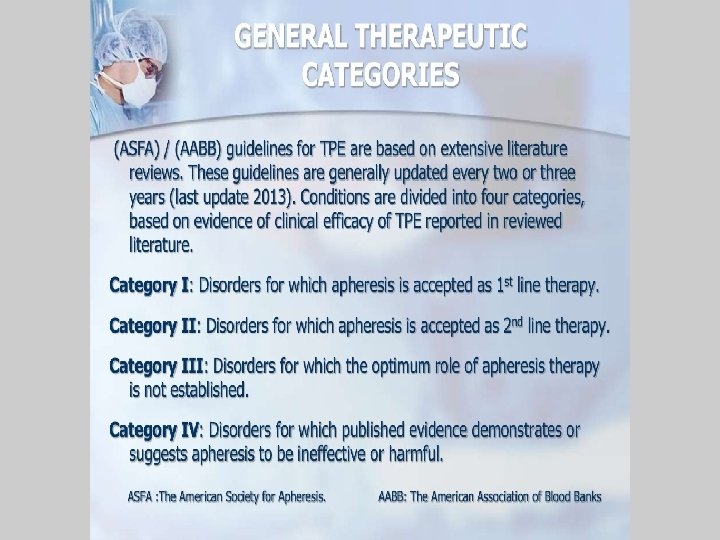
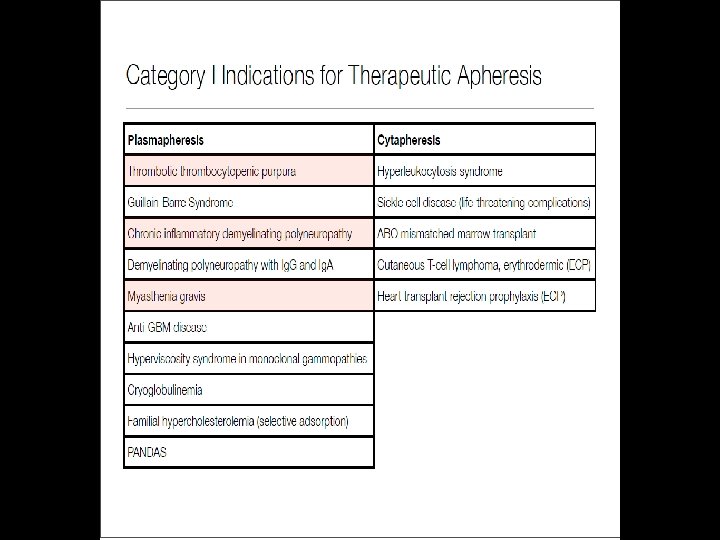
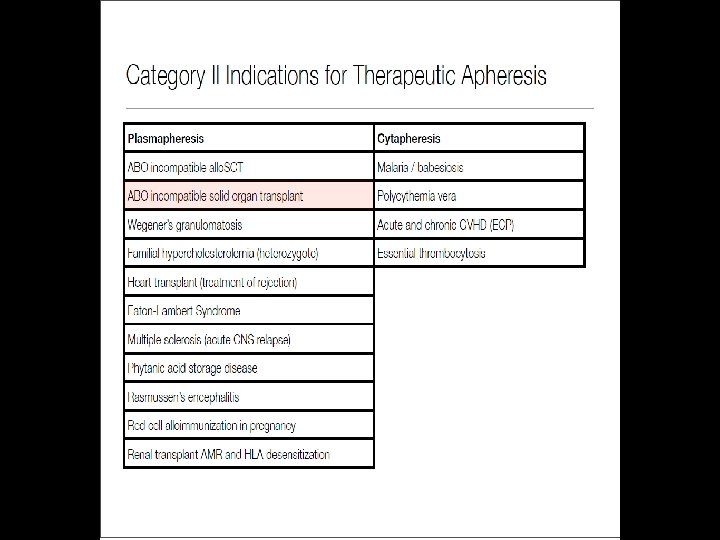
INDICATIONS FOR PLASMAPHERESIS

TECHNIQUES q A: Centrifugal plasma separation : blood cells are separated during centrifugation , there are two centrifugation methods Intermittent flow device and continuous flow device q B: membrane plasma separation : plasma separators use membranes with a molecular weight 3 million
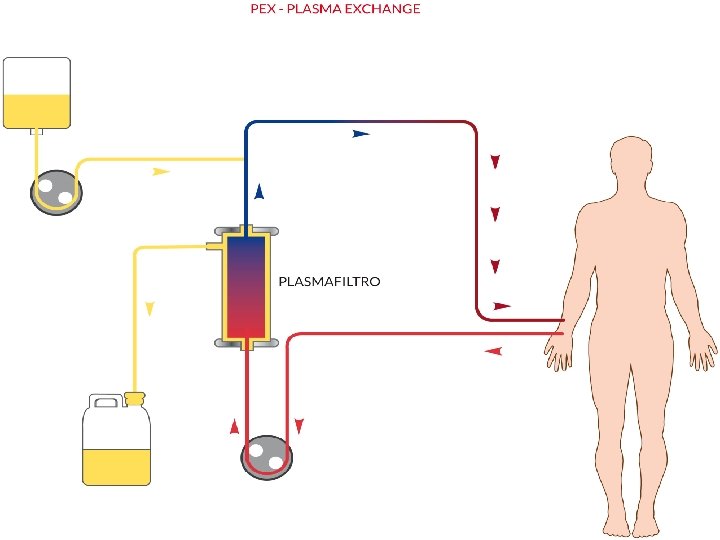



membrane plasma separation q Uses highly permeable hollow fibers with membrane pores of 0. 2 to 0. 5 µm. q The hollow fiber functions as a membrane, with the pore size (0. 2 to 0. 5 µm) allowing transport of plasma across the membrane while retaining other blood components. q Plasma. Flux filters contain the polysulfone based Plasmasulfone membrane, which has been designed to minimise the activation of the patient’s immune system during blood– membrane interaction
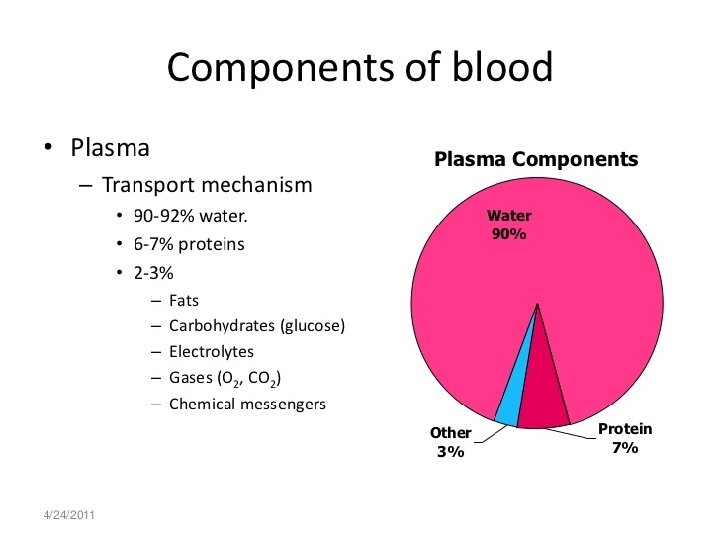
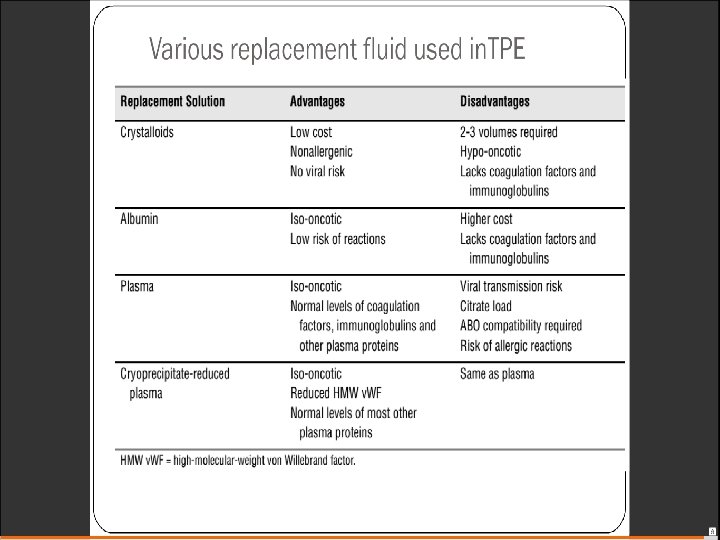

Serum Albumin q Serum Albumin : 4 g /d. L 40 g /L 40 × 3 = 120 g /3 L

Electrolytes Calcium: 10 ml of calcium gluconate solution per liter of replacement solution Potassium : 4 mmol of Potassium to each liter of replacement solution
 fistula q Peripheral access through")
Vascular access q Standard central venous catheters q Arteriovenous(AV) fistula q Peripheral access through large bore, short, intravenous cannulae

Anticoagulation 1 Citrate q IT is used for centrifugal plasma exchang. q citrate has particular advantages in patients at higher bleeding risk in view of its lack of systemic anticoagulant actions. q Citrate is rapidly metabolized by the liver (normal levels within 4 hours). Hepatic dysfunction ⇒ severe hypocalcemia

2 – Heparin q Used for membrane plasma filtration q Higher doses may be needed than in hemodialysis as a result of increased losses during the procedure (heparin is protein bound). q Bolus doses of unfractionated heparin 2000 to 5000 U are given initially, and then 500 to 2000 U/h.

Regimens of PE? Volume of exchange Frequency of procedures 1 -1. 5 plasma volume Duration of therapy
 ×")
Plasma volume q Plasma volume = ( 0. 07 × Body Weight ) × ( 1 Hct ) ( 0. 07 × 70 ) × ( 1 . 4 ) = 2. 9 L

Frequancy of procedures 1 Daily plasma exchange q Most effective in rapidly depleting total body load. q Intensity of exchanges has no major effect on outcomes except in hemolytic uremic syndrome. 2 Alternate day exchanges q proven efficacy in antineutrophil cytoplasmic antibody (ANCA)–associated diseases.
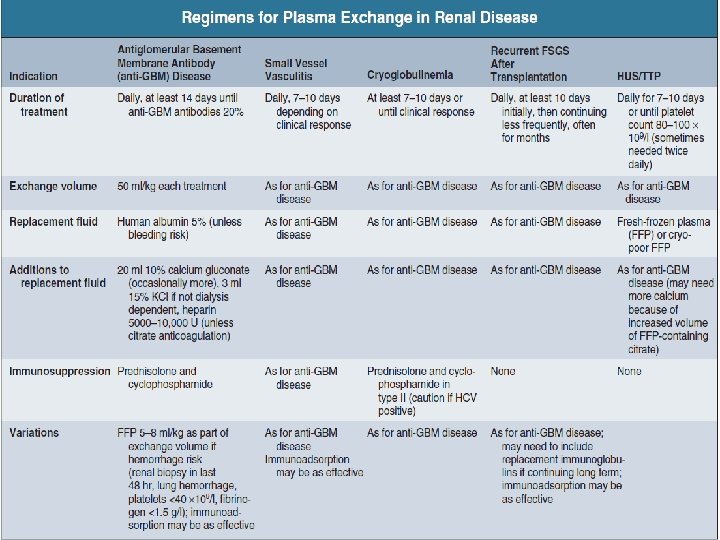

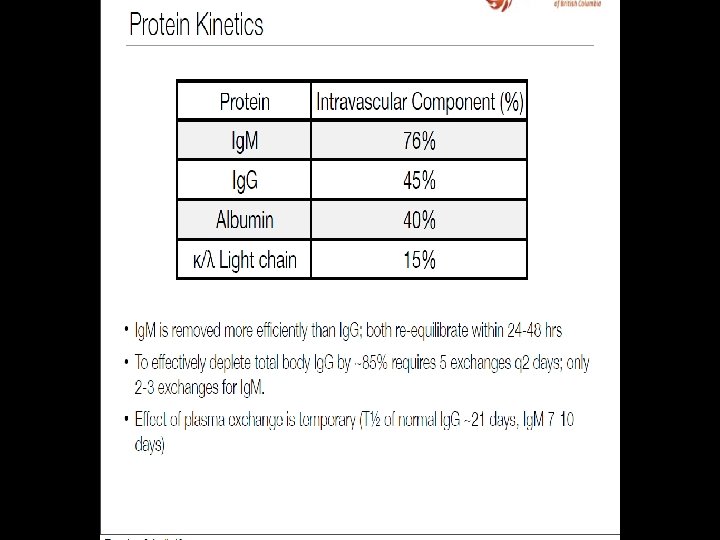
q A single plasma volume exchange will lower plasma macromolecule levels by approximately 60%. q Five exchanges during 5 to 10 days will clear 90% of the total body Immunoglobulin

Target molecule kinetics during therapeutic plasma exchange. Mark E. Williams, and Rasheed A. Balogun CJASN doi: 10. 2215/CJN. 04680513 © 2013 by American Society of Nephrology


THANK YOU
- Slides: 31