Plasma Cell Neoplasms and Related Disorders These Bcell

Plasma Cell Neoplasms and Related Disorders

• These B-cell proliferations contain neoplastic plasma cells that virtually always secrete a monoclonal Ig or Ig fragment, which serve as tumor markers and often have pathologic consequences. • The most common and deadly of these neoplasms is multiple myeloma.

• A monoclonal Ig identified in the blood is referred to as an M component, in reference to myeloma. • Because complete M components have molecular weights of 160, 000 or higher, they are restricted to the plasma and extracellular fluid and excluded from the urine in the absence of glomerular damage.

• neoplastic plasma cells often synthesize excess light chains along with complete Igs. • Occasionally only light chains are produced, and rare tumors secrete only heavy chains. • In patients with plasma cell tumors, the level of free light chains is usually elevated and is markedly skewed toward one light chain (e. g. , kappa) at the expense of the second (e. g. , lambda). • Because free light chains are small in size, they are also excreted in the urine, where they are referred to as Bence-Jones proteins.

• Terms used to describe the abnormal Igs associated with plasma cell neoplasms include monoclonal gammopathy, dysproteinemia, and paraproteinemia. • These abnormal proteins are associated with the following clinicopathologic entities: - Multiple myeloma (plasma cell myeloma) - Plasmacytoma - Smoldering myeloma (lack of symptoms) - Waldenström macroglobulinemia (high levels of Ig. M , hyperviscosity of the blood) - Heavy-chain disease - Primary or immunocyte-associated amyloidosis - Monoclonal gammopathy of undetermined significance (MGUS)

Multiple Myeloma • Multiple myeloma is a plasma cell neoplasm commonly associated with: - lytic bone lesions, - hypercalcemia, - renal failure, - and acquired immune abnormalities. It is chiefly a disease of older adults, with a peak age of incidence of 65 to 70 years.

• Pathogenesis: - Multiple myeloma is associated with frequent rearrangements involving the Ig. H locus and various proto-oncogenes. - The proliferation and survival of myeloma cells are dependent on several cytokines, most notably IL-6. It is produced by the tumor cells themselves and by resident marrow stromal cells. - Myeloma cell growth and survival are also augmented by direct physical interactions with bone marrow stromal cells. - Factors produced by neoplastic plasma cells mediate bone destruction, the major pathologic feature of multiple myeloma
")
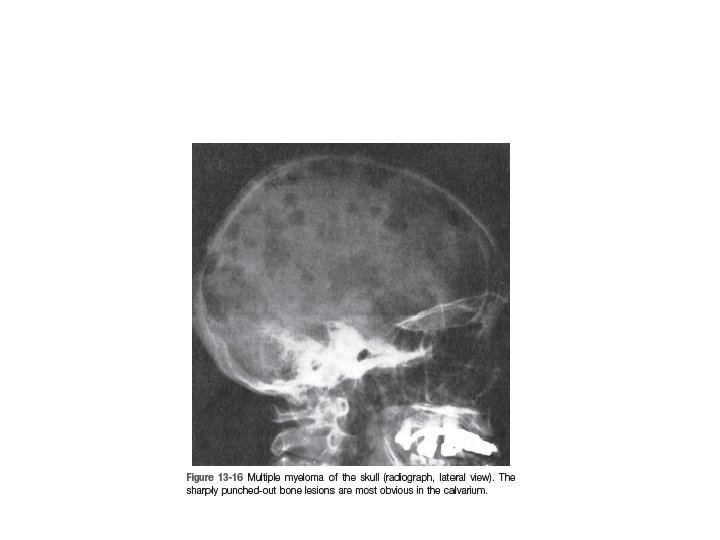
• MORPHOLOGY: - Multiple myeloma usually presents as destructive plasma cell tumors (plasmacytomas) involving the axial skeleton. - The bones most commonly affected (in descending order of frequency) are the vertebral column, ribs, skull, pelvis, femur, clavicle, and scapula. - Lesions begin in the medullary cavity, erode cancellous bone, and progressively destroy the bony cortex, often leading to pathologic fractures; these are most common in the vertebral column, but may occur in any affected bone. - Less commonly, widespread myelomatous bone disease produces diffuse demineralization (osteopenia) rather than focal defects.

• the marrow contains an increased number of plasma cells, which usually constitute more than 30% of the cellularity. • Relatively normal-appearing plasma cells, plasmablasts with vesicular nuclear chromatin and a prominent single nucleolus, or bizarre, multinucleated cells may predominate.

• • flame cells Mott cells Russell bodies Dutcher bodies

Flame cell

Mott cells

Russell bodies

Dutcher bodies

• the high level of M proteins causes red cells in peripheral blood smears to stick to one another in linear arrays, a finding referred to as rouleaux formation. • Rouleaux formation is characteristic but not specific, as it may be seen in other conditions in which Ig levels are elevated, such as lupus erythematosus and early HIV infection. • Bence Jones proteins are excreted in the kidney and contribute to a form of renal disease called myeloma kidney.
 the")
• Clinical Features: The clinical features of multiple myeloma stem from: (1) the effects of plasma cell growth in tissues, particularly the bones; (2) the production of excessive Igs, which often have abnormal physicochemical properties; (3) the suppression of normal humoral immunity.

• Bone resorption often leads to pathologic fractures and chronic pain. • hypercalcemia can give rise to neurologic manifestations (confusion, weakness, lethargy, constipation, and polyuria), and contributes to renal dysfunction. • Decreased production of normal Igs sets the stage for recurrent bacterial infections. Cellular immunity is relatively unaffected. • renal insufficiency, occurs in up to 50% of patients, the single most important factor seems to be Bence-Jones proteinuria, as the excreted light chains are toxic to renal tubular epithelial cells. • amyloidosis • Marrow involvement often gives rise to a normocytic normochromic anemia, sometimes accompanied by moderate leukopenia and thrombocytopenia

• In 99% of patients, laboratory analyses reveal increased levels of Igs in the blood and/or light chains (Bence-Jones proteins) in the urine. • The monoclonal Igs are usually first detected as abnormal protein “spikes” in serum or urine electrophoresis and then further characterized by immunofixation.


• more than 3 gm/d. L of serum Ig • and/or more than 6 mg/ d. L of urine Bence. Jones protein. • The most common monoclonal Ig (“M protein”) is Ig. G (approximately 55% of patients), followed by Ig. A (approximately 25% of cases). Myelomas expressing Ig. M, Ig. D, or Ig. E occur but are rare.

• Both free light chains and a serum M protein are observed together in 60% to 70% of patients. • However, in about 20% of patients only free light chains are present. Around 1% of myelomas are nonsecretory; hence, the absence of detectable M proteins does not completely exclude the diagnosis.

definitive diagnosis requires a bone marrow examination.

• The median survival is 4 to 7 years, and cures have yet to be achieved • Patients with multiple bony lesions, if untreated, rarely survive for more than 6 to 12 months, whereas patients with “smoldering myeloma” may be asymptomatic for many years.
 - Thalidomide and")
• Treatment: - Proteasome inhibitors (misfolded proteins activate apoptotic pathways) - Thalidomide and related compounds (protein degradation) - Biphosphonates
 • Solitary osseous plasmacytoma almost inevitably progresses to multiple myeloma, but")
Solitary Myeloma (Plasmacytoma) • Solitary osseous plasmacytoma almost inevitably progresses to multiple myeloma, but this can take 10 to 20 years or longer. • extraosseous plasmacytomas, particularly those involving the upper respiratory tract, are frequently cured by local resection.

Smoldering Myeloma • Plasma cells make up 10% to 30% of the marrow cellularity • the serum M protein level is greater than 3 gm/d. L • patients are asymptomatic. • About 75% of patients progress to multiple myeloma over a 15 -year period.

Monoclonal Gammopathy of Uncertain Significance. • patients are asymptomatic • the serum M protein level is less than 3 gm/d. L. • Approximately 1% of patients with MGUS develop a symptomatic plasma cell neoplasm, usually multiple myeloma, per year, • MGUS is an early stage of myeloma development.
- Slides: 28