Place de la Radiologie dans le traitement des








 • Rt-PA iv 0. 45 mg/kg < 3 h +")
 • • • Rt-PA iv 0. 6 mg/kg")

 57 Hémorragie majeure %")


 Mort ou dépendance Tous les essais 5216")




































 Baseline TIMI 0 TIMI 1 TIMI 2")


 Median Time from Symptom Onset to Arterial 4. 1 hrs")













 technique(s) pour quels patients? • • • NIHSS < 10 < 3 h")
 technique(s) pour quels patients? Attitude nancéenne 2007 • IV – < 3 heures")










- Slides: 92
Place de la Radiologie dans le traitement des AVC ischémiques: La revascularisation cérébrale Serge BRACARD CHU Nancy 2009
Plan • Techniques • Indications • Organisation
Techniques • Thrombolyses chimiques – Thrombolyse IV – Thrombolyse IA – Thrombolyse IV + IA – Anti Gp IIb-IIIa • Thrombolyses mécaniques • Associations
Résultats 1. Taux de reperméabilisation concept: la restauration du flux permet les conditions favorables à la récupération… 2. % parenchyme sauvé 3. Résultats cliniques 4. Complications
Augmentation de la pénétration du thrombolytique dans le thrombus par application trans-crânienne d’ultrasons • CLOTBURST – 126 Patients r. Tpa IV – Randomisation +/- ultra-sons (DTC continu 2 MHz) – Reperméabilisation 49% versus 30% – Pas de différence sur la récupération clinique Alexandrov NEJM 2004, 351, 2170 -8 • Intérêt des microbulles Molina stroke 2006, 37, 425 -429 – MUST (Microbubbles and Ultrasound in Stroke Study) – Etude multicentrique, française (PHRC), contrôlée, randomisée – Occlusions M 1, alteplase iv <3 h vs alteplase + Doppler transcrânien + microbulles iv < 3 h • Augmentation du risque hémorragique ?
Thrombolyse IA: PROACT II • 180 patients avec occlusion ACM < 6 h • R-pro. UK IA + héparine vs héparine • Pas de thrombolyse mécanique R-pro. UK + héparine Héparine TIMI 2 -3 >2 h 66% 27% TIMI 3 > 2 h 19% 2% m. Rs 0 -2 à 3 mois 40% 25% ICH sympto 10% 2% Door to ia treatment time : 5, 3 h
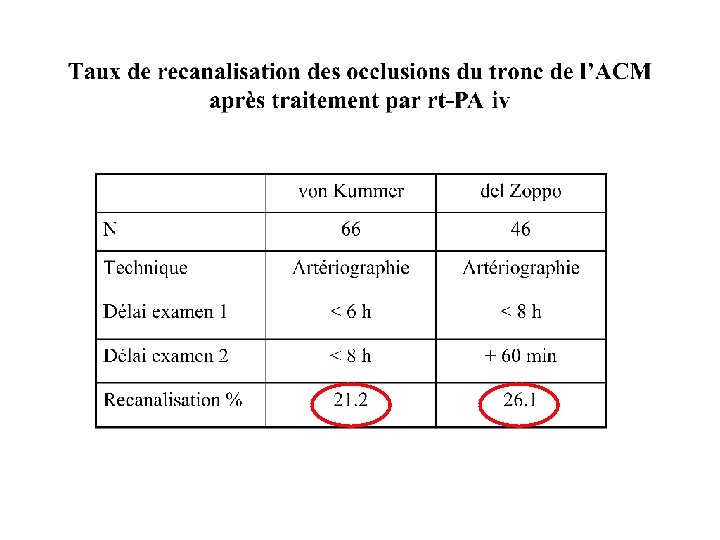
Recanalisation
Association IV +IA • IA est plus efficace en termes de reperméabilisation mais nécessite 1 h pour sa mise en route • IV est moins efficace mais plus rapide à mettre en œuvre IV +IA devrait associer les bénéfices deux…
Interventional Management Study (IMS) • Rt-PA iv 0. 45 mg/kg < 3 h + ia 22 mg en 2 h • 80 patients • Seulement 5% des patients étaient recanalisés après traitement iv • Injection dans thrombus • TIMI 3 : 11% • TIMI 2 -3 : 56% • Délai traitement ia : 217+/-46. 7 min
Interventional Management Study II (IMS II) • • • Rt-PA iv 0. 6 mg/kg < 3 h + ia 22 mg en 2 h 76 patients Injection dans thrombus + sonde à ultrasons EKOS TIMI 2 -3 : 69% Récupération, mortalité= NINDS Interventional Management Study III (IMS III) • IV vs IV+IA+ EKOS ou MERCI (en cours)
Association de produits avec des cibles différentes Thrombus rt-PA Fibrinolyse Exposition de thrombine Activation plaquettaire Anti-GP IIb-IIIa • Thrombus fibrino-plaquettaire • Libération PAI-1
En cardiologie: TIMI 14 Traitement TIMI 3 % (90 min) 57 Hémorragie majeure % Abciximab 32 3 SK faible + abciximab 34 10 SK fort + abciximab 46 10 Alteplase 50 mg+ abciximab 77 7 (1) Alteplase 100 mg 6 Rien n’est démontré en neurologie…
Efficacité: taux de reperméabilisation • Variable • r. Tpa IV seul – d’autant plus efficace que l’occlusion est distale – insuffisant pour les « gros troncs » • r. Tpa IA plus efficace • Associations +++ • Limite actuelle : 60 -70%
Efficacité : Résultats cliniques Study N ECASS Fibrinolytic Time window Mortality ________ Active Placebo Rankin 0 -1 ________ Active Placebo 620 rt-PA- 1. 1 mg/kg 6 h 17. 9%£ 12. 7%£ (14. 6%) (11. 7%) 22. 4%££ 15. 8%££ (19. 4%) (14. 8%) 0 difference (0 difference) NINDS 624 rt-PA – 0. 9 mg/kg 3 h 17%££ 21%££ ECASS II 800 rt-PA – 0. 9 mg/kg 6 h 10. 3%££ 10. 5%££ 54, 3%* 46, 1% ATLANTIS 547 rt-PA – 0. 9 mg/kg 3 -5 h 11%££ 6. 9%££ 36% 34% + 13% SK: Streptokinase; UK: Urokinase; rt-PA: recombinant tissue plasminogen activator; : intent-to-treat population, ( ): target population (intent-to-treat population less protocol violations); ECASS II : analyse post hoc ( but initial: Rankin 0, pas de différence)
Méta analyses Nombre de malades Mort (OR) Mort ou dépendance Tous les essais 5216 1, 31 0, 83 rt-Pa < 6 h 2688 1, 24 0, 79 rt-Pa < 3 h 869 0, 95 0, 55
Study N MAST-E Fibrinolytic Time window Mortality ________ Active Placebo Symptomatic ICH ________ Active Placebo 310 SK - 1. 5 M 6 h 34%* 18%* 45%§ 35%§ 21%* 2. 6%* MAST-I 622 SK - 1. 5 M Aspirin 6 h 27%* 12%* 36%$ 26%$ 8% 1. 3% ASK 340 SK - 1. 5 M 4 h 36%££ 20%££ 12. 6% 2. 4% ECASS 620 rt-PA- 1. 1 mg/kg 6 h 17. 9%£ 12. 7%£ (14. 6%) (11. 7%) 22. 4%££ 15. 8%££ (19. 4%) 14. 8%) 19. 8%£ 6. 5%£ (19. 4%) (6. 8%) NINDS 624 rt-PA – 0. 9 mg/kg 3 h 17%££ 21%££ 6. 4% 0. 6% ECASS II 800 rt-PA – 0. 9 mg/kg 6 h 10. 3%££ 10. 5%££ 8. 8% 3. 4% ATLANTIS 547 rt-PA – 0. 9 mg/kg 3 -5 h 11%££ 6. 9%££ 7% 1. 1% PROACT II 180 IA Pro-UK 6 h 25%££ 27%££ 10% 2% Cleveland group 54 6 h 24%££ - 17% - IA UK SK: Streptokinase; UK: Urokinase; rt-PA: recombinant tissue plasminogen activator; IA: intra-arterial; *: at day 10; § : at day 108; $: at 6 months; : intent-to-treat population, ( ): target population (intent-to-treat population less protocol violations); £ at 1 month; ££: at 3 months; : no placebo group; only PROACT II and the Cleveland group’s study evaluated intra-arterial thrombolysis while the other studies reported in this table evaluated intravenous thrombolysis.
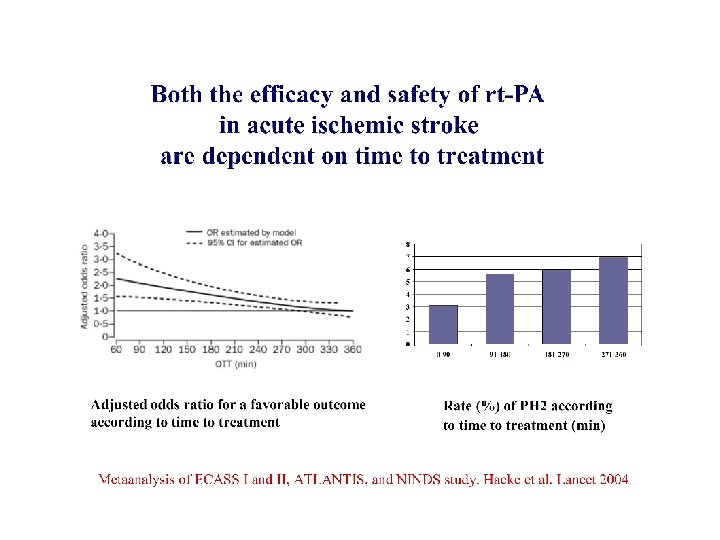
Thrombolyse IV: délai de 3 h? • Délai légal AMM • Méta analyse Hacke 2004 bénéfice au delà? • ECASS III: efficacité entre 3 et 4 h 30 – – 821 patients r. Tpa vs placebo Rankin 0 -1 à 90 jours: 52, 4% vs 45, 2% p=0, 04 Hémorragies symptomatiques: 2, 4 vs 0, 12 p=0, 008 Mortalité: 7, 66 vs 8, 44% Hacke NEJM 2008, 359, 1317 • EPITHET – Thrombolyse IV 3 -6 h chez des patients avec un mismatch en IRM. – A 3 mois volume infarctus non diminué mais pronostic meilleur Davis Lancet neurol 2008, 7, 299 -309
PROACT II - Patients
Intracranial hemorrhage
90 -day Modified Rankin Outcome 0 -2 control r. Pro. UK 3 -4 25% 40% 5 -6 41% 34% 26% 35% P=0, 043
Autres études • Urokinase: – MELT Ogawa Stroke 2007, 38, 2633 – Iv vs IA nancy Ducrocq 2005 J of Neuroradiology – Etude cas témoin (m. Rs 0 -2: 50, 5 vs 34%) Inoue cerebrovasc dis 2005 • r. Tpa – Études observationnelles
IV ou IA • Pas d’étude randomisée importante • Etude de 83 patients avec une ACM hyperdense – Thrombolyse IV: meilleur pronostic avec IV si pas de MCA hyperdense – Thrombolyse IA: pas de différence Agarwal Cerebrovas Dis 2004, 17, 182
Association IV+IA: rt-PA iv 0. 45 mg/kg < 3 h + ia 22 mg en 2 h
Efficacité sur le plan clinique Limite actuelle: 40% de patients autonomes à 3 mois - IV Toutes occlusions confondues - IA et associations : sur les « gros troncs »
FACTEURS PRONOSTIQUES • CIRCULATION COLLATERALE • DELAI • TOPOGRAPHIE
VALEUR PREDICTIVE du CBF • CBF >55% : récupérable > 6 heures • CBF > 35%: récupérable < 6 heures • CBF< 35% : Résultats ? Risques d’hémorragie Ueda, J Cereb Blood Flow Metab 1999, 19, 99 -108
Thrombolyse: localisations Other factors: NIHSS <20, LIT started <4 h Gonner F Stroke 1998, 29, 1894 -900
Thrombolysis - results
600000 IU 900000 IU J 7
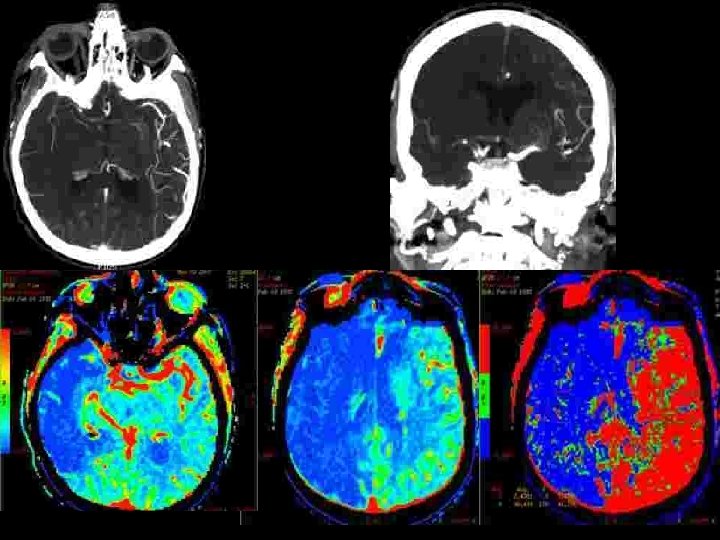
CBF CBV MTT
Occlusion en T de la carotide: pronostic effroyable • Evolution spontanée : – mortalité : 41 -50%, dépendance sévère : 29 -51% • Control group of the Duplex sonography in acute stroke study (27 patients avec traitement médical seul ) – Recanalisation (6 h) 1/27 – Hémorragies 6/27 (18%) – Évolution clinique (3 mois) • m. RS 0 -2 • m. RS 3 -5 • décès 0 17/27 (63%) 10/27 (37%) Wunderlich MT et al Cerebrovascular diseases 2005; 20: 355 -361
Occlusion en T de la carotide: pronostic effroyable • Pourquoi? • Deux facteurs principaux – Intéresse les artères lenticulostriées – Pauvreté de la circulation collatérale: l’artère communicante antérieure est elle perméable?
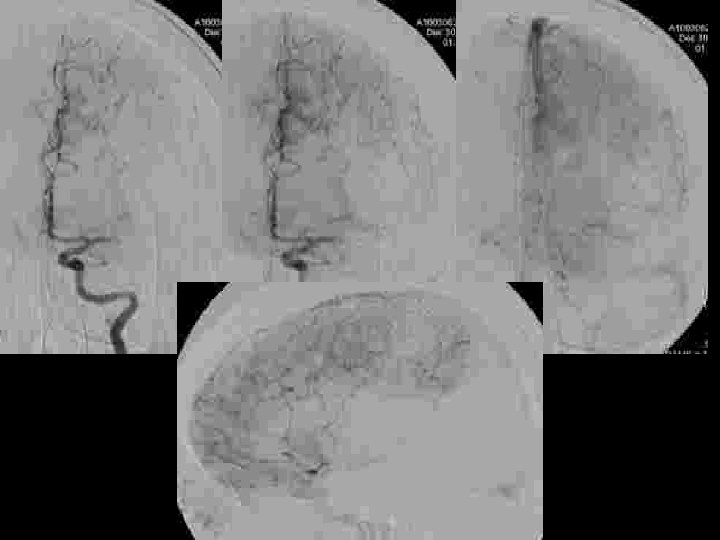
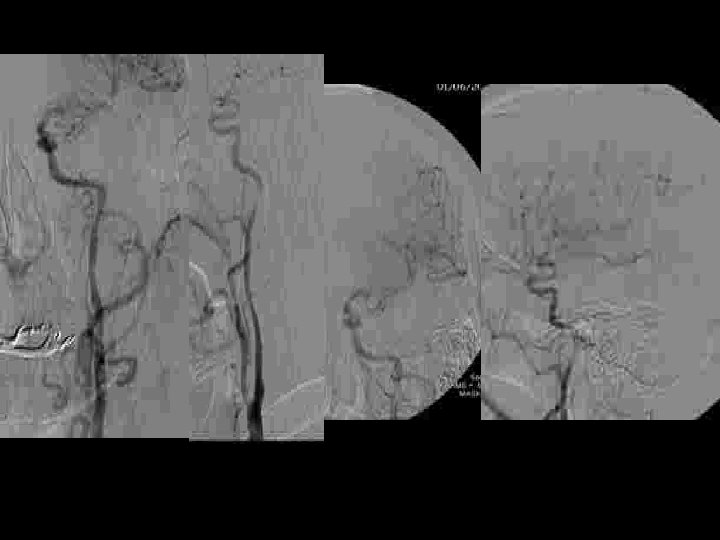
OCCLUSION du « T » CAROTIDIEN : RESULTATS DE LA THROMBOLYSE INTRA-ARTERIELLE CHEZ 21 PATIENTS • Etude rétrospective de 21 patients traités dans les 6 heures – – – 14 femmes, 7 hommes Age: 58. 4 ans (31 -84) NIHSS à l’admission: 18. 9 (12 -33) Délai de traitement: 262. 4 minutes (180 – 330) maladie cardio-embolique : 10 patients (47, 7%)
OCCLUSION du « T » CAROTIDIEN : RESULTATS DE LA THROMBOLYSE INTRA-ARTERIELLE CHEZ 21 PATIENTS • circulation collatérale – Artère communicante antérieure • Présente • Absente 14 7 – Opacification rétrograde de l’ACM • Jusqu’à la région insulaire • Incompléte • Absence 3 cas 9 cas • Technique • thrombolyse Mécanique • Mécanique +chimique 6 cas 15 cas * Urokinase (900. 000 UI): 7 cases * Actilyse (0, 9 mg/kg): 8 cases + 1/15 stenting carotidien cervical (sténose >90%)
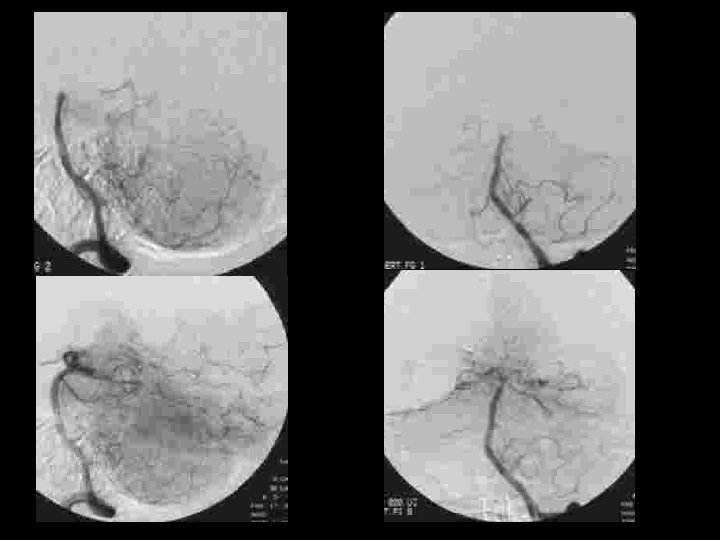
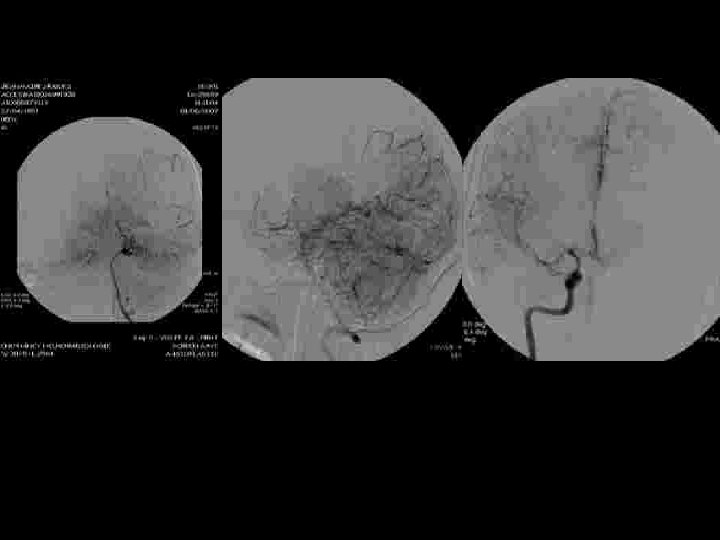
Thrombectomie mécanique « Catch , Balt» + 70 mg r. Tpa
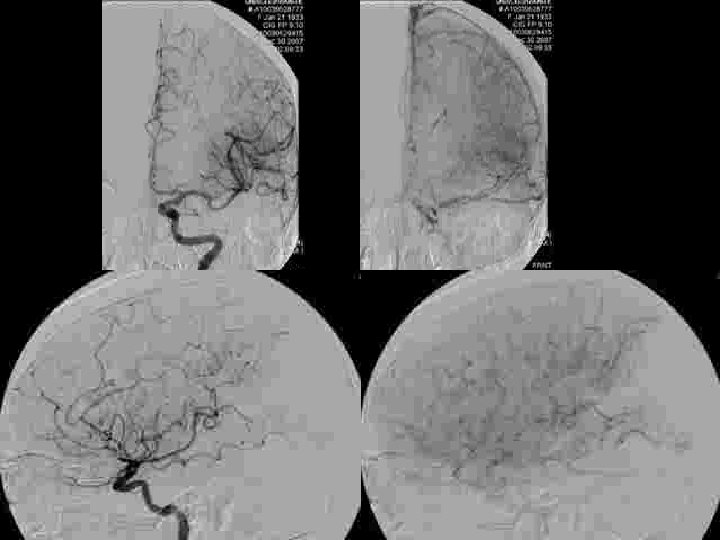
Résultats Recanalisation • Immediate en Angiographie : – TIMI 0 6/21 – TIMI 1 5/21 – TIMI 2 -3 10/21 • DTC à 24 heures: Recanalisation - 13 cas (62%) Hémorragies 9 cas Transformation hémorragique 2/9 Hématome symptomatique 7/9 à 3 mois m. RS 1 m. RS 3 -4 décès 2/2 1/7 3/7
EVOLUTION CLINIQUE • A J 7 – – • A 3 mois (Modified Rankin Scale –m. RS) – – – • 7 morts (33, 3 %) (3 complications hémorragique) 14 patients survivants avec un score NIH de 6. 8 m. RS 0 -1 m. RS 2 m. RS 3 -4 10 patients 1 patient 3 patients résultats m. RS 0 -1 m. RS 2 m. RS 3 -4 m. RS 6 47. 7 % 14. 2 % 33. 3 % 4. 8 %
Recanalisation / Evolution Clinique
Conclusions • Le pronostic des occlusions en T de la carotide interne reste sévère – recanalisation (TIMI 2 and 3) moins fréquente que pour M 1 – complications hémorragiques plus fréquentes (7/21) • La thrombolyse intra artérielle améliore le pronostic • La thrombectomie mécanque améliore le taux de recanalisation et son délai
Carotide cervicale
THROMBO ASPIRATION
Après THROMBO ASPIRATION
stent + protection device + angioplastie
Destruction mécanique du caillot • Thrombo-aspiration • Fragmentation – Injections pulsées – Guides – Ballons: angioplasties – Stents – Ultrasons • Retrait
AVANTAGES THÉORIQUES • Temps: la thrombectomie peut être réalisée en quelques minutes alors que la dissolution chimique peut prendre jusqu’à 2 heures – Extension de la fenêtre thérapeutique • Pas d’effet anti thrombotique – Moins de complications hémorragiques – Moins de contre indications (chirurgie, saignement récent…) • Efficacité en termes de reperméabilisation
Merci à René Chapot!
The MERCI retrieval system : - a retriever in a microcatheter - a 9 F balloon guide catheter 1 st step: the retriever is deployed inside the clot to ensnared the thrombus 2 nd step: The ensnared clot is withdrawn - occlusion of the carotid or vertebral artery - continuous aspiration
• 151 patients treated – 10 adverse events: 3 dissections, 3 arterial perforations and 2 distal embolisation. 2 patients died – Hemorrhages • Symptomatic hemorrhage rate: 7. 8% • Asymptomatic hemorrhage rate: 28. 9% – Recanalization: 46% (69/151) – Overall mortatity at 90 days: % • Patients successfully revascularised: 32% • Patients not revascularised: 54% – Modified Rankin score at 90 days • 46% of patients successfully revascularised had a m. Rs from 0 to 2 • 10% of patients not revascularised
Thrombus Debulking and Aspiration • Reperfusion Catheter and Separator™ System – Operator motion of Separator clears catheter tip to allow continuous entry of thrombus – Three sizes to match the site of occlusion: 041, 032, 026 – Optimizes inner diameter and flexibility for maximum aspiration & navigation – Neuro-designed Separator tip softness – Faster, easier revascularization when time is brain The Penumbra System™
Baseline Characteristics No. of Patients Screened 856 No. of Patients Enrolled 125 Age ( Years) Female 63. 5 ± 13. 5 49% NIHSS at Baseline 17. 6 + 5. 2 m. RS at Baseline 4. 5 + 0. 8 Target Vessel Locations: ICA 18% (23/125) MCA 70% (87/125) Vertebrobasilar 9% (11/125) Other 3% (4/125) TIMI 0 96% (120/125) TIMI 1 4% (5/125) Mean Time to Presentation (Hrs) 1. 9 + 1. 6
Primary Endpoint TIMI Scores (N = 125) Baseline TIMI 0 TIMI 1 TIMI 2 TIMI 3 96% 4% 0 0 TIMI 2 & 3 0 Post Treatment 10% 9% 54% 27% 82% (102/125)
Primary Endpoint Procedural SAEs Event Perforation ICH Total N=125 N 2 2 4 % 1. 6% 3. 2% • All 4 events were adjudicated by the Clinical Events Committee as not device related. • There were no incidents of device malfunction or breakage.
Secondary Endpoints Clinical And Functional Outcome ≥ 4 point improvement in NIHSS at discharge ≥ 10 point improvement in NIHSS, or NIHSS 0 -1 at discharge % 58% 27% m. RS ≤ 2 at 90 days 25% Death at 30 days 26% Death at 90 days 33%
Time to Revascularization (N=125) Median Time from Symptom Onset to Arterial 4. 1 hrs Puncture Median Time Required for Revascularization 45 mins
INDICATIONS SELECTION DES PATIENTS CONTRE INDICATIONS
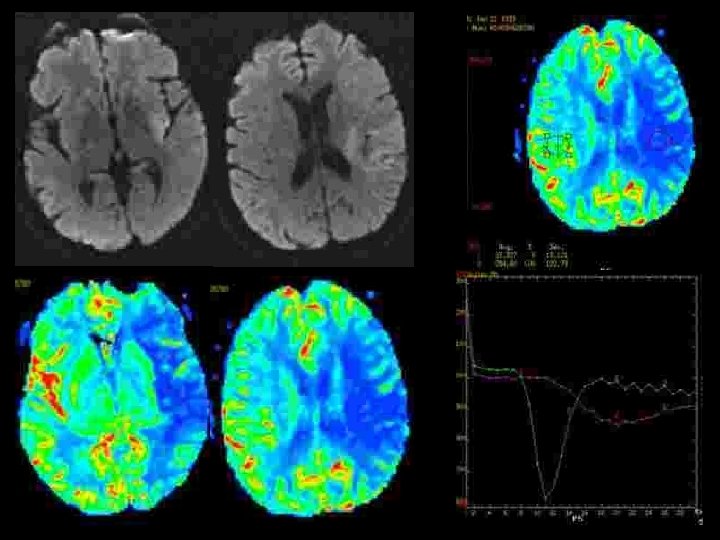
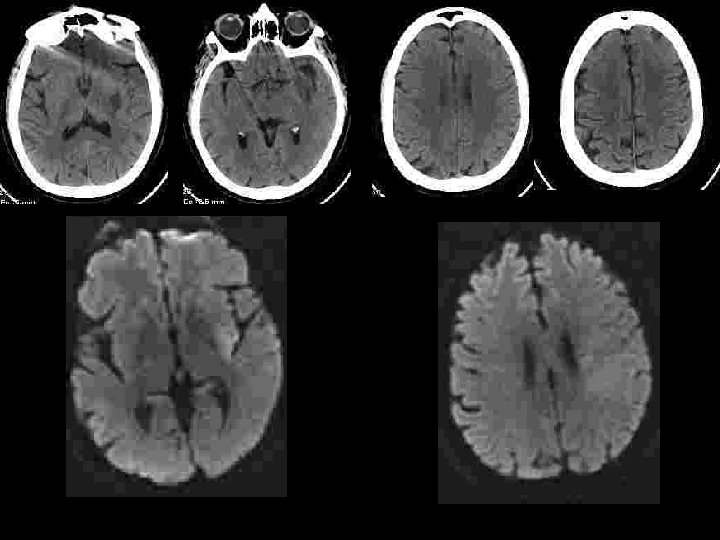
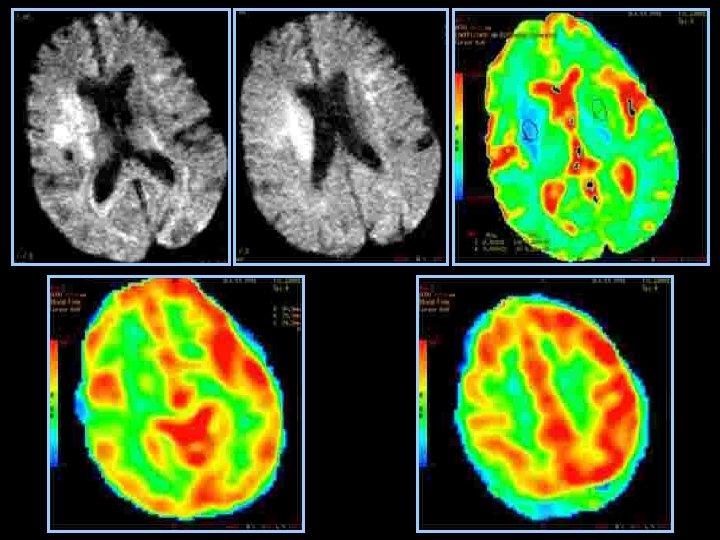
Sélection des patients • Être efficace : y a t’il du parenchyme a sauver ? – Diffusion : nécrose définitive! discutable: • diminution des zones d’anomalies de diffusion après thrombolyse IA • Hétérogénéité des niveaux de baisse d’ADC à l’intérieur de la zone anormale • diminution progressive de l’ADC de la périphérie vers le centre: notion de seuil? – < 50 % : évolution vers la nécrose certaine – >70 -80% : récupérable si recanalisation – Importance de l’évaluation de l’ischémie: • collatéralité en angiographie • perfusion en IRM ou en scanner
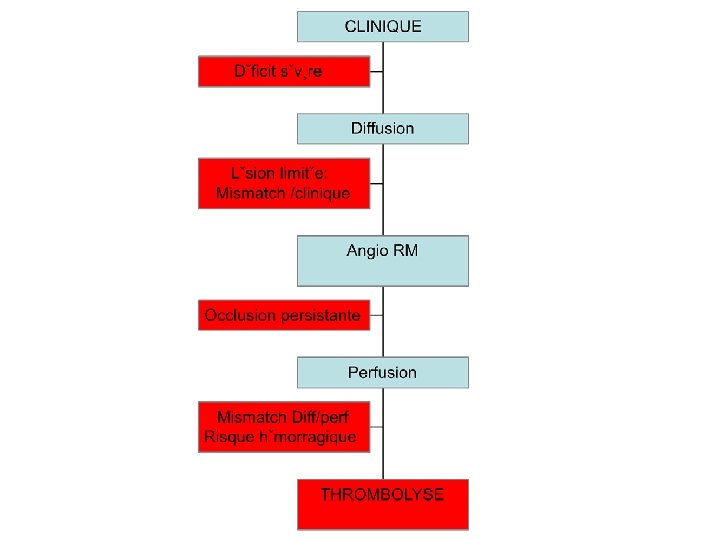
Sélection des patients imagerie • Efficace – – Est ce un AVC? Ischémique ou hémorragique? Mismatch? Occlusion persistante? • Rapide < 15 minutes Time is brain!! – MRI: Diffusion+3 d TOF MRA+ Perfusion. MR – CT scanner+angio CT+ perfusion CT
Sélection des patients • Ne pas être dangereux: identifier les patients à haut risque d’hémorragie – Localisation profonde – Délai – Baisse de l’ADC: risques si ADC< 33% – Hypoperfusion sévère : CBF< 33%
46 centers Stroke survey Belgium 2 Czech Republic 1 France 10 Germany 5 Hungary 1 Italy 8 Latvia 1 Norway 2 Portugal 2 Romania 1 Spain 4 Sweden 1 Switzerland 2 Serbia 1 Turkey 2 United Kingdom 3
Diagnosis in emergency 75% use CT scan always or frequently!
• Angio CT • Perfusion CT Most often without CT angio or CT perfusion. Only 24% used systematically CTA and 19% CT perfusion
MRI in emergency MRI is less often used in emergency with 43% using MRI always or frequently
With a cerebral MRAngiography in the same session in 79%
Perfusion MRI With an MR perfusion study in 60% of cases The mismatch evaluation in 81% even in the first 3 hours in 50% of cases
Sécurité • La sélection sur l’IRM augmente t’elle la sécurité de la thrombolyse? – Ringleb et al JNNP 2007; 78: 690 -693 • 90 octogénaires • Hémorragies 9, 4% avec CT , 0 avec IRM • 0 influence sur l’évolution globale – Schellinger et al Stroke 2007 • 1210 patients (CT<3 H: 714, MRI<3 h: 316, MRI >3 h: 180) • Hémorragies symptomatiques : 5, 3%, 2, 8% et 4, 4% • mortalité: 13, 7% vs 11, 7% avant 3 h • Influence sur le taux d’évolution favorable après 3 h
INDICATIONS • Thrombolyse à la carte ! Ou plutôt indication personnalisée: – Clinique – Diffusion – Perfusion – Angio-RM
Quelle technique pour quels patients? • IV: NINDS • tous type d’AVC (résultats moins bons pour les artères principales) • < 3 h • IA : PROACT II • NIHSS > 10 • < 6 h • Mismatch ? • Risque hémorragique?
Quelle(s) technique(s) pour quels patients? • • • NIHSS < 10 < 3 h IRM/CT ? r. Tpa IV +Abciximab? + Ultrasons? • • • NIHSS > 10 < 3 h IRM r. Tpa IA +Abciximab? r. Tpa IV? • NIHSS > 10 • > 3 h • IRM • Mécanique ± r. Tpa IA • ±Abciximab?
Quelle(s) technique(s) pour quels patients? Attitude nancéenne 2007 • IV – < 3 heures – « mismatch » ? – M 1 distal et au delà • IA – > 3 heures : toutes localisations – < 3 heures : TB, ACI, M 1 proximal – Mismatch diff/perf
46 centers Stroke survey Belgium 2 Czech Republic 1 France 10 Germany 5 Hungary 1 Italy 8 Latvia 1 Norway 2 Portugal 2 Romania 1 Spain 4 Sweden 1 Switzerland 2 Serbia 1 Turkey 2 United Kingdom 3
Techniques
Indications In M 2 occlusion IV T is often preferred in the first 3 hours and IA r. Tpa after 3 hours
In M 1 occlusion, IVT is preferred in the first 3 hours, often associated with IA thrombolysis. After 3 hours a mechanical thrombectomy is proposed alone or combined with IA r. Tpa in 20 centers
In the same way, IA mechanical thrombolysis is proposed in 21 centers for T occlusion of ICA and only 4 centers used an IVT alone!
For a basilar tip occlusion an IVT is proposed in only 2 centers and IA in 33 with a mechanical device in 18.
Organisation: EN PRATIQUE ! Priorité de l ’établissement ! Organisation simple et économe en temps: • un seul point d’entrée • accès direct à l’imagerie 24 h/24 • un nombre limité d’intervenants
Objectifs • Aller vite! aller vite… – Rester dans les délais • PROACT II 5, 3 h • Nancy IA/IV 5, 2 h IA/ 4, 25 IV – Efficacité: récupération fonction du délai
Objectifs 1 er médecin consulté • Aller vite! aller vite…? Hôpital de proximité SAU neurologue Thrombolyse IRM scanner
Objectifs Patient-famille 1 er médecin consulté Hôpital de proximité 15 - SAMU IRM neurologue Thrombolyse scanner