PKU and Inborn Errors of Metabolism Leora Aframian

PKU and Inborn Errors of Metabolism Leora Aframian Belen Rediet Nhu My Tran Kanako Miyoshi Kelly Bigley NTRS 413 Spring 2014

What is PKU? ● PKU stands for Phenylketonuria ● It is an autosomal recessive inborn error disease ● Results in Phenylalanine inability to be converted to Tyrosine due to a defective enzyme.

Metabolism of Phenylalanine
? ● Disorders due to a defect in")
What is Inborn Error of Metabolism (IEM)? ● Disorders due to a defect in a single gene which causes disruption in metabolic pathways ● Leads to accumulation of a particular substrate or deficiency of a product ● IEMs can be transmitted genetically by autosomal recessive or X-linked recessive

More on IEM ● Common IEM are fibrosis, hypothyroidism, sickle cell anemia, and PKU ● Affects 1 in every 5, 000 newborns ● PKU: 1 in 15, 000 births in U. S. ● Couples with one child having IEM will be at risk of having other affected children

IEM and PKU ● PKU is an inherited metabolic disorder ● Autosomal recessive disorder, requires two alleles for the individual to express the symptoms of the disease ● Those with PKU lack the enzyme phenylalanine hydroxylase (PAH) ● This prevents the phenylalanine from converting to tyrosine (amino acid used in many bodily synthesis)

Consequences of PKU ● Defective PAH results in an accumulation of phenylalanine which in turns converts to phenylpyruvate (this is detected in urine). ● Those with PKU can experience seizures, delayed development, behavioral problems, and psychiatric disorders. ● Children with PKU often have lighter skin and hair.

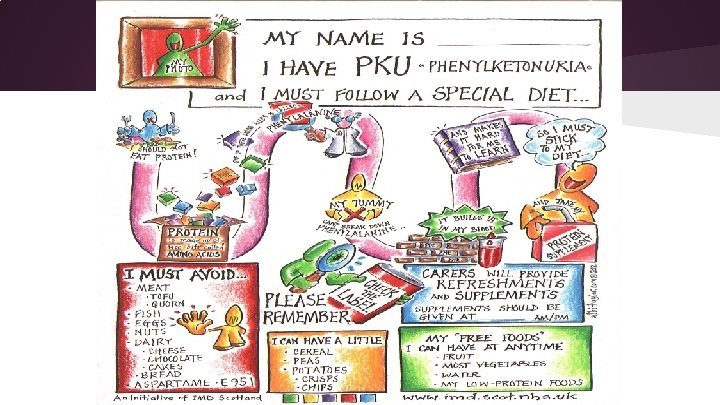
PKU Dietary Treatment

Maternal phenylketonuria and hyperphenylalaninemia in pregnancy: pregnancy complications and neonatal sequelae in untreated and treated pregnancies. Babette W Prick, Wim CJ Hop, and Johannes J Duvekot The American Journal of Clinical Nutrition 2012
")
Author’s Objective ● To present an overview of pregnancy complications and neonatal sequelae (consequences) of maternal phenylketonuria or hyperalaninemia in untreated and treated pregnancies.

Who were the Subjects? Subjects of the study: ● Authors conducted a search on 2 databases for published case studies from January 1980 to October 2009 for treated and untreated pregnancies with maternal phenylketonuria or hyperalaninemia ● 15 unpublished cases were added from their own clinic.

The authors noticed a trend. . . ● In 1974 postnatal screening for phenylketonuria was introduced in the Netherlands (where this study was conducted, prevalence is 1: 18, 000) ● Consequently, more women were diagnosed with phenylketonuria and hyperphenylalaninemia and followed a special diet. ● However, this protective diet was discontinued by many women after adolescence because there are few noticeable negative effects of elevated phenylalanine concentrations after this time.

Trend continued. . . ● Untreated phenylketonuria and hyperphenylalaninemia have many negative effects on both the mother and her baby such as congenital heart disease, low birth weight babies, and facial dysmorphism. ● Because of these serious side effects mothers are urged to keep a strict diet preconception.

Methods ● Cases were reviewed in Medline and Embase ● For treated cases, phenylalanine concentrations before conception and per trimester were recorded. ● For untreated cases, at least one maternal phyanalline concentration before or during pregnancy had to be reported. ● Total of 39 articles were reviewed, 181 pregnancies in 84 mothers ● 15 pregnancies from their own clinic were added to the pool. ● The phenylalanine concentrations between the treated and untreated group during all trimesters were analyzed and compared using statistical analysis.

Results -Total of 196 pregnancies in 88 women - PKU diet and protein supplements introduced to 70 of these pregnancies, 30 of which started before conception. - Target Phenylalanine concentration averaged 480 micrograms/mol as a TUL. -Average concentration of treated group was 1. 5, 2. 6, and 3. 2 respectively for the 1 st, 2 nd and 3 rd trimester.

Results - 196 Pregnancies received - 126 pregnancies untreated 70 treated - No significant difference between treated and untreated in regards to pregnancy complications - Preterm delivery occurred less often in untreated women, but not statistically significant -SGA, microcephaly, and Intellectual and Developmental Disabilities was significantly related to mean phenylalanine concentration in each trimester, with Facial Deformities only relating to the first trimester

Results Untreated -Out of 117 Neonates -19 born SGA - 48 with microcephaly - 5 born with CHD (2 fatalities) - A follow up of 81 Neonates -38 with IDDs -14 with Facial deformities - 7 with epilepsy

Results Treated Out of 62 pregnancies - 2 fatalities -10 Microcephaly - 2 CHD Follow-up of 42 Neonates -11 IDDs deformities - 4 SGA - 6 Facial

Discussion -Most birth defects higher in untreated group - Some occurrences higher in untreated group but not necessarily statistically significant. - Lower significance may be the result of fewer numbers

Conclusion - Continue PKU diet if already on it. Start it if not.

Long-chain polyunsaturated fatty acid concentration in patients with inborn errors of metabolism M. A. Vilasseca, L. Gomez-Lopez, N. Lambruschini et al. Nutricion Hospitalaria 2011
 that")
Background of IEMs and LCPUFAs ● Caused by defects in specific proteins (enzymes) that help break down (metabolize) parts of food. ● Diet of patients with IEMs exclude a specific protein ● LCPUFAs are essential for normal growth ○ DHA: fundamental in the structure and function of the central nervous system and retina ● Food Source of LCPUFAs ○ fatty fish those are usually excluded from ○ eggs their diet ○ milk

Objective ● IEMs are disease with a special risk for LCPUFA deficient status ● To evaluate LCPUFA status in patients with different IEMs.

Subject Cross sectional study of plasma and erythrocyte LCPUFA phospholipid composition in 132 patients with classified into 2 group

Subject continued. . Group 1: 63 patients with IEMs, protein-restricted diets ○ 27 with urea cycle disorders ○ 15 with homocystinuria ○ 12 with organic acidurias ○ 5 with MSUD ○ 2 with Tyrosinemia-I ○ 2 with NKH Group 2: 69 patients with IEMs, protein unrestricted diet

Methods ● Nutritional examination Three-day food record Group 1: natural protein daily intake according to individual tolerance o Group 2: natural protein intake with WHO recommendations for age and gender o o

Method continued. . . ● Biochemical methods o Blood sample after an overnight fast for PUFA analysis o Serum total and free carnitine were analysed by a spectrometric procedure o Plasma and erythrocyte total fatty acids were derivatized to fatty acid methyl esters, and data was expressed as weight percentage of total fatty acids ● Statistical analysis

Results ● In clinical data and intake of patients with IEM o No significant differences were observed in natural protein intake compare to the different inborn errors of metabolism treated with protein restrictions

More Results. . . ● ● In protein-restricted group, 45% of patients showed decreased amount of erythrocyte and plasma DHA values. Only 7% and 10% of patients in the proteinunrestricted group From the groups: ● 12% and 28% of group 1 patients showed decreased erythrocyte and plasma AA (arachidonic acid) values ● 14% and 20% of group 2… they conducted Chi square test: X= 14. 13; p= 0. 007 only for plasma

More Results. . . ● Serum-free carintine and alpha-tocopherol concentration weren’t different among the three studied groups. o Total carnitine levels were significantly higher in patients who were treated in protein- restricted diets then the other two groups.

Limitations ● Difficulties to gather a large number of patients with each disease. ● The heterogeneity of the patient groups, which can lead to a bias in the interpretation of the results. o Difficult to get homogenous groups of patients

Conclusion -LCPUFA has had extended reports in PKU patients but only few data on IEM. -Those with IEM to have rise on their nutritional management

References Prick, Babette, Wim Hop, and Johannes Duvekot. "Maternal phenylketonuria and hyperphenylalaninemia in pregnancy: pregnancy complications and neonatal sequelae in untreated and treated pregnancies 1– 3. " The American Journal of Clinical Nutrition 95: 374 -82. Web. 17 Apr. 2014. Vilaseca, Ma. A. , et al. "Long-Chain Polyunsaturated Fatty Acid Concentration In Patients With Inborn Errors Of Metabolism. "Nutricion Hospitalaria 26. 1 (2011): 128 -136. Academic Search Premier. Web. 8 May 2014. "What Is PKU? " NSPKU. N. p. , n. d. Web. 01 May 2014. "Family Area. " Welcome to the IMD Scotland Website. N. p. , n. d. Web. 5 May 2014. William R. "Phenylalanine: An inborn error of Phenylalanine Metabolism. " NCBI. 2008.
 Phenyleprine B) Phenylketonuric C) Phenylalanine D)")
Question #1 What does PKU stand for? A) Phenyleprine B) Phenylketonuric C) Phenylalanine D) Phenylketonuria
 Phenylketonuria")
Answer #1 D) Phenylketonuria
 Phenylalanine Oxylase B)")
Question #2 What enzyme is defective in those with PKU? A) Phenylalanine Oxylase B) Phenylalanine Hydroxylase C) Phenylalanine enzyme D) PKU Hydroxylase
 Phenylalanine Hydroxylase")
Answer #2 B) Phenylalanine Hydroxylase

Question #3 In the U. S. , out of every 15, 000 live births how many are borned with PKU? A) 2 B)500 C) 1 D) 100
 1")
Answer #3 C) 1

Thank you!!!!
- Slides: 41