Pieter Bruegel The Triumph of Death c 1562

Pieter Bruegel - The Triumph of Death - c 1562 Pandemonium to Pandemic A Brave New World of Viral Disease Dr Keith Paver

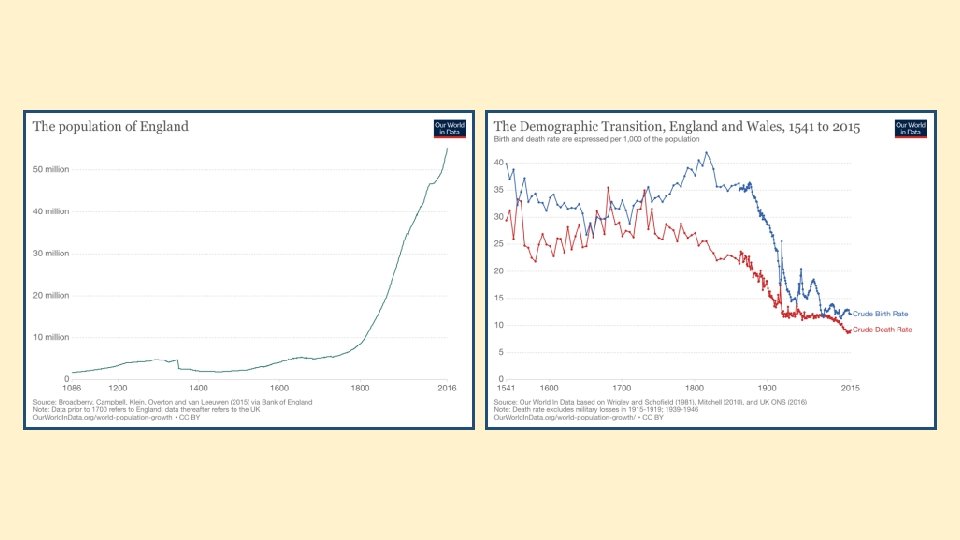
It Improved access to clean water and sanitation and dealing with extreme poverty are essential in reducing child mortality

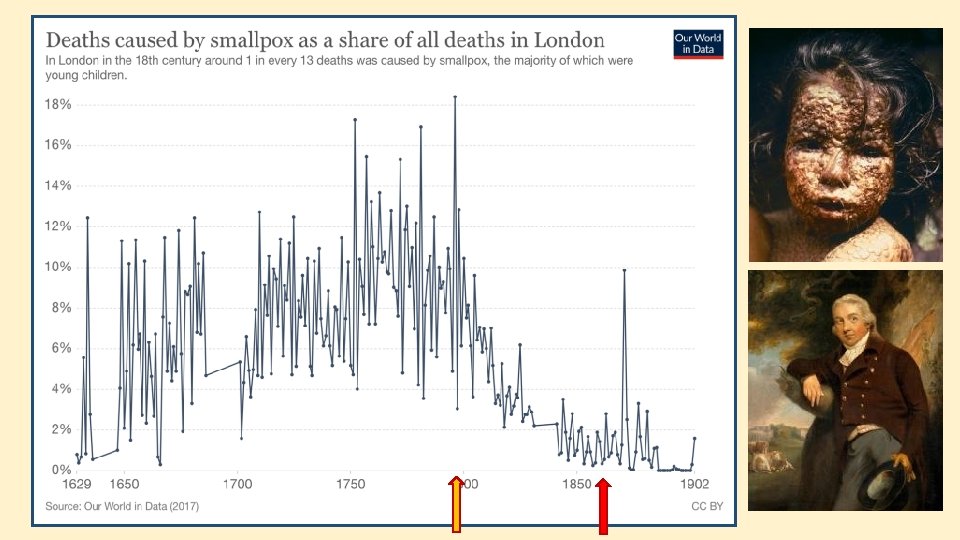
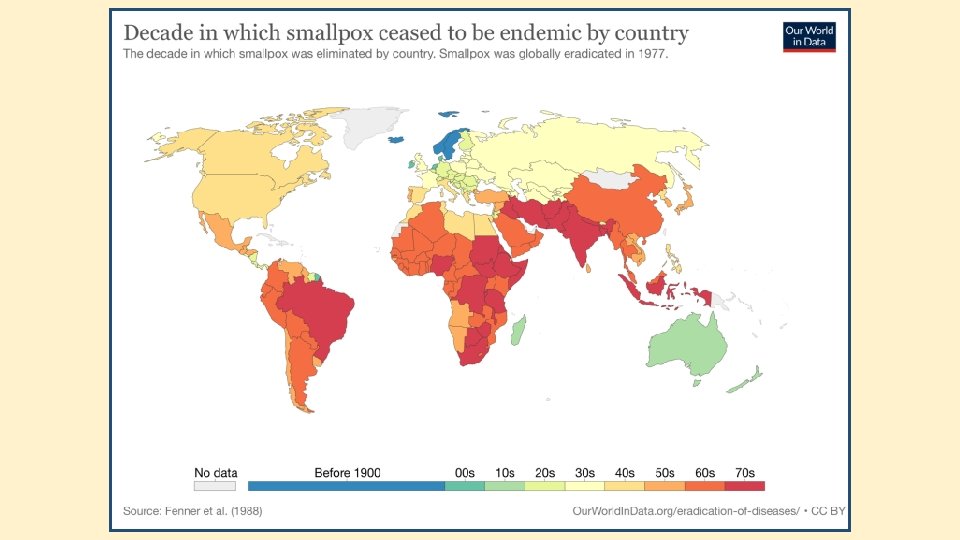
In the United Kingdom over the last two centuries many endemic and epidemic diseases have been controlled or eradicated

1851 1901


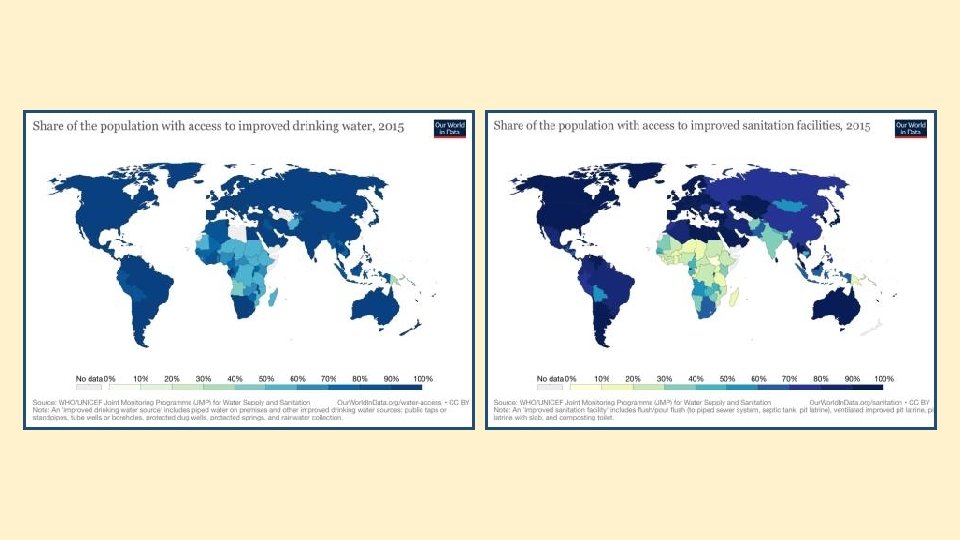

Poverty and poor health worldwide are inextricably linked. Infectious and neglected tropical diseases kill and weaken millions of the poorest and most vulnerable people each year.
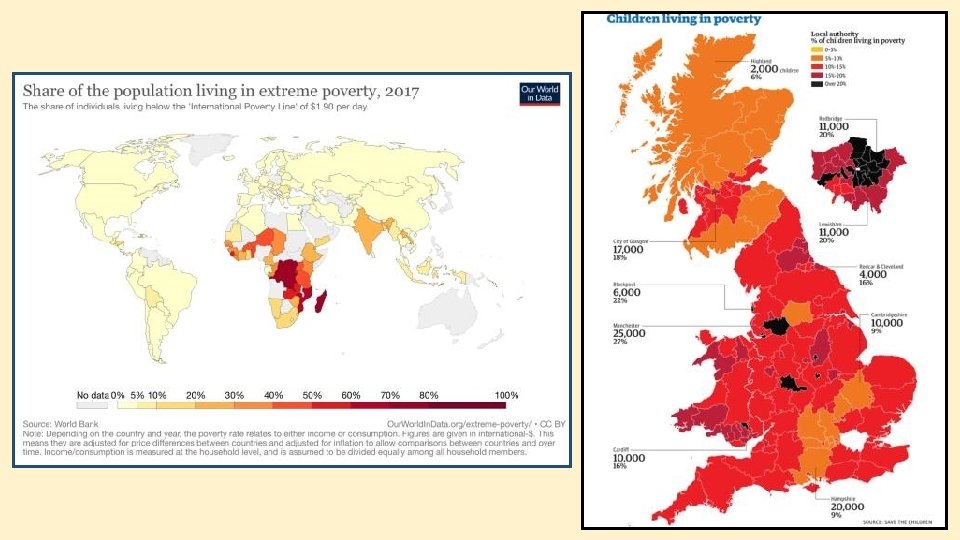

High income countries Low income countries

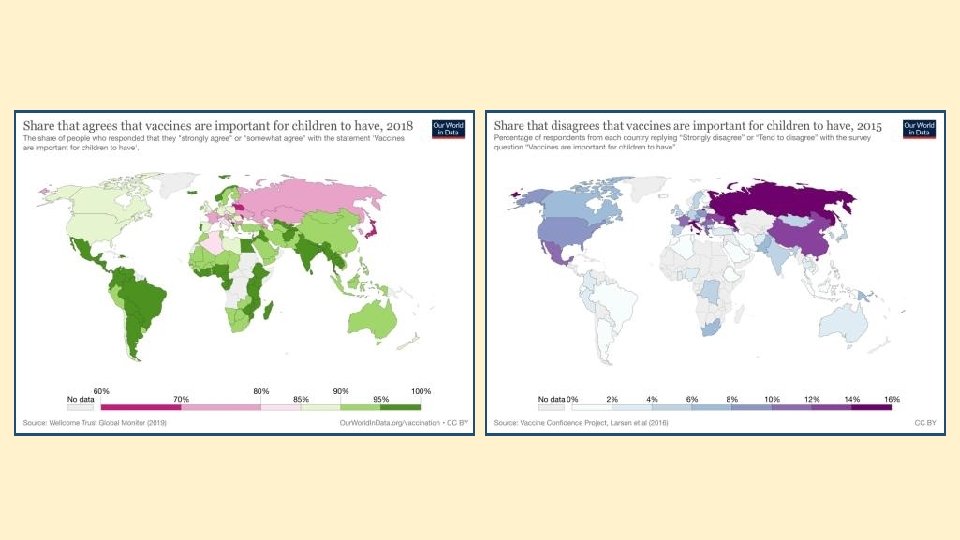
It Vaccination is the single most important medical intervention in the history of humankind.

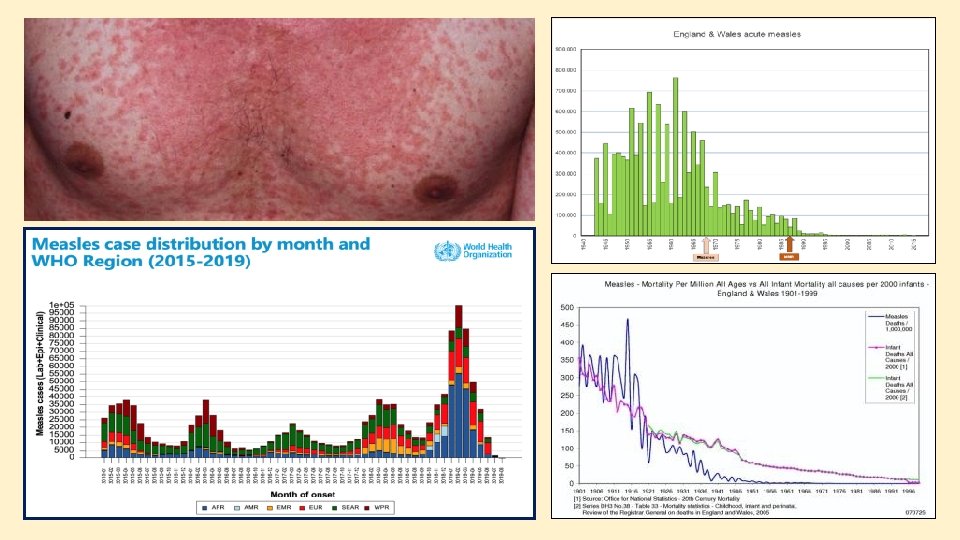
top ten causes of mortality in children aged 1 -4 in England & Wales in 1915 males cause Measles Broncho-pneumonia Other bronchitis Whooping cough Diphtheria Tuberculous meningitis Pneumonia Meningitis Infective enteritis Scarlet fever females percent 20. 5 16. 4 6. 3 6. 2 5. 0 4. 2 4. 1 2. 4 2. 2 2. 0 cause Measles Broncho-pneumonia Whooping cough Other bronchitis Diphtheria Tuberculous meningitis Pneumonia Meningitis Infective enteritis Scarlet fever percent 20. 9 15. 6 9. 0 6. 2 5. 0 4. 2 4. 0 2. 3 2. 2 2. 1

Vanishing diseases in the UK Bacterial • • Cholera Typhoid Whooping cough Diphtheria Tuberculosis Bacterial pneumonia Meningitis Viral • • Smallpox Polio Measles Mumps Rubella Human papilloma virus Rotavirus

UK vaccine timeline 1940 diphtheria 2000 annual flu vaccine for over 65 s 1950 s whooping cough whole cell vaccine 2004 whooping cough acellular vaccine 1953 BCG (tuberculosis) 1955 inactivated polio vaccine 1961 tetanus 1962 oral polio vaccine (discontinued 2004) 2004 inactivated polio vaccine reintroduced 2006 pneumococcal vaccine for over 65 s 2008 human papillomavirus (HPV) 2013 rotavirus 2013 chickenpox vaccine for over 70 s 1968 measles 2013 children’s annual flu vaccine 1960 s flu vaccine for high risk patients 2015 meningitis B and meningitis ACWY 1970 rubella 2018 diphtheria, tetanus, pertussis, IPV, Haemophilus influenzae type b and hepatitis B combined vaccine for infants 1988 MMR 1999 meningitis C (Men. C)

A Few Facts About Epidemiology • • • Infection and disease are not the same. Infection can occur in the absence of symptoms of disease, but not vice versa. Endemic viruses are constantly detected in a population, often at low levels, and maintained without external inputs. An epidemic is a greater than expected number of endemic cases in a coherent population. Pandemic disease is a widespread epidemic affecting more than one region or country. The aim of public health measures including vaccination is to prevent both infection and disease.




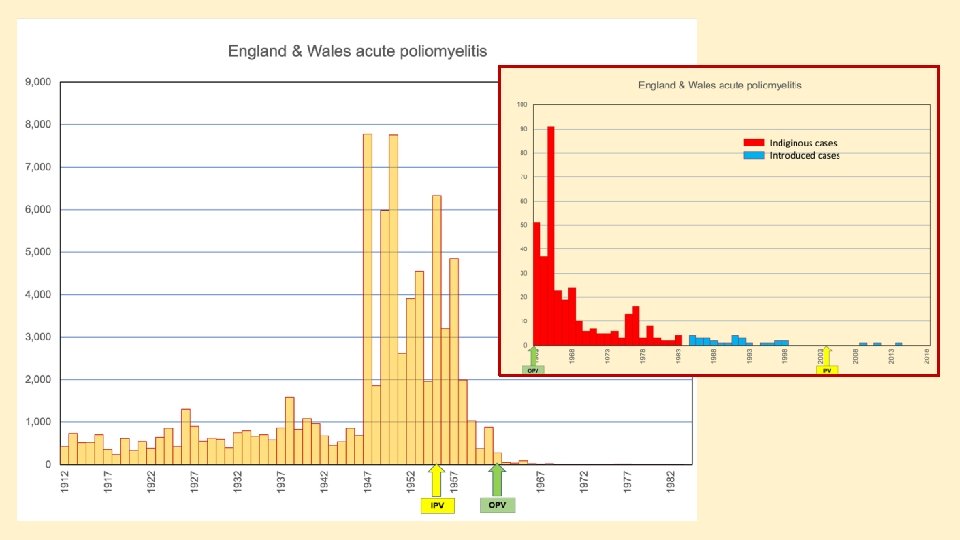
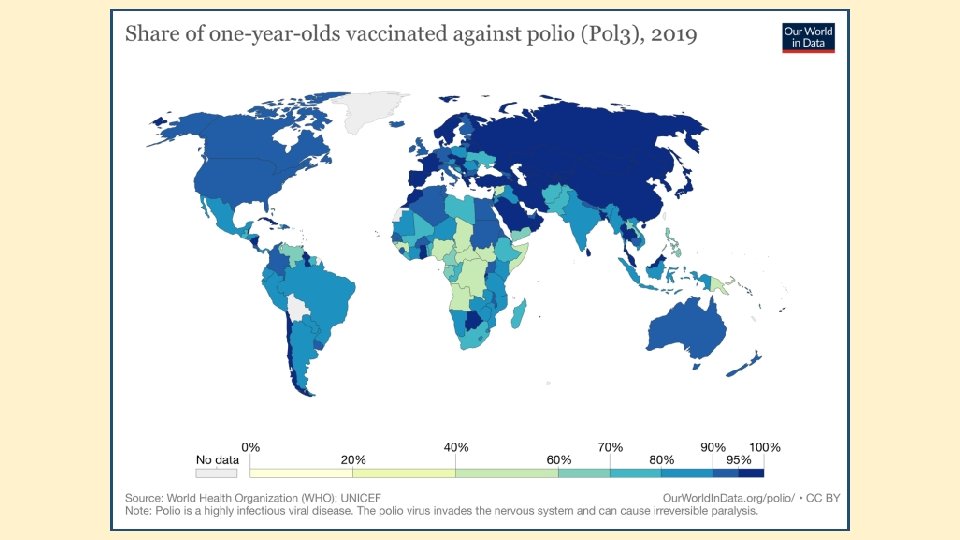
Epidemic poliomyelitis Before the late 19 th century almost all people were infected with poliovirus before their 1 st birthday when they were protected by maternal antibody. As water, sanitation and hygiene standards improved, the age at which children were first exposed to the poliovirus increased and this meant that maternal antibodies were no longer present to protect them. Over the course of the 20 th century the age at which polio was contracted increased, and by the 1950 s the average of infection was 6 -8 years with a substantial proportion of cases in teenagers and young adults.

Poliovirus infection and disease • • Infection takes place by ingestion of nasopharyngeal fluids or faecally contaminated fomites (clothing, food or water). Maximum infectivity lasts for approx 7 days beginning 7 days after contact, but faecal shedding can last for several weeks. Virus grows in cells lining the throat and upper small intestine and can enter the blood stream (viraemia). 70% children under 5 have no symptoms. Approx 25% of children under 5 have a mild flu-like illness. Approx 5% of children have non-paralytic neurological illness (aseptic meningitis) with complete recovery. Only 0. 5% of children develop acute flaccid paralysis.

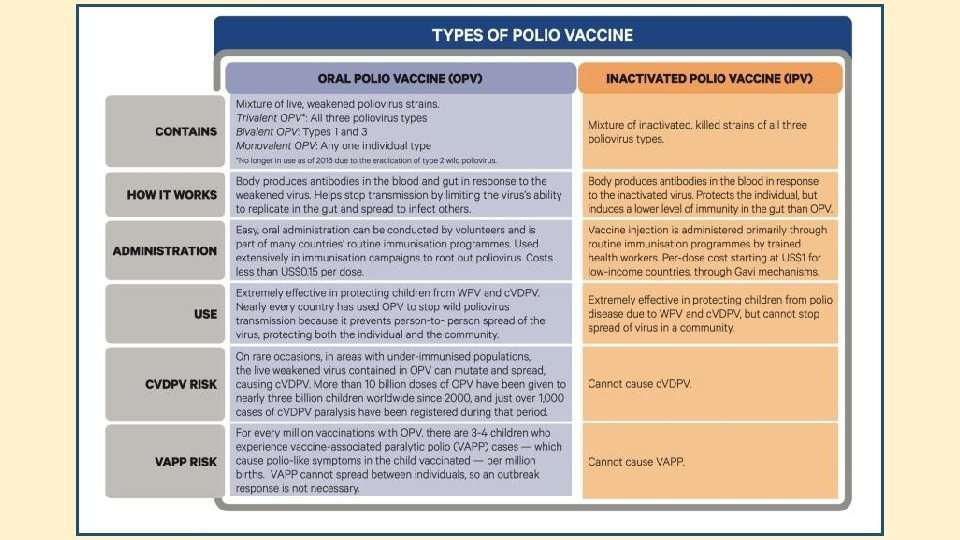
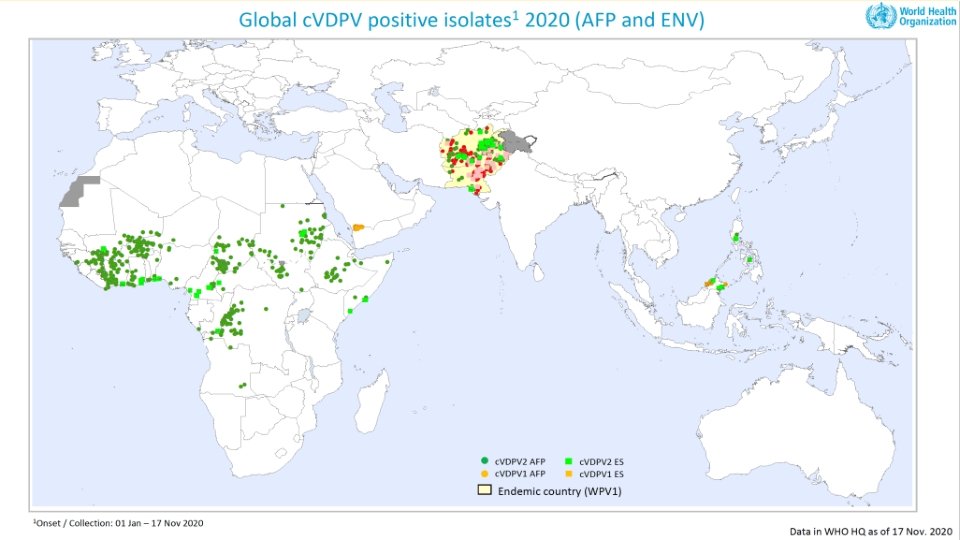
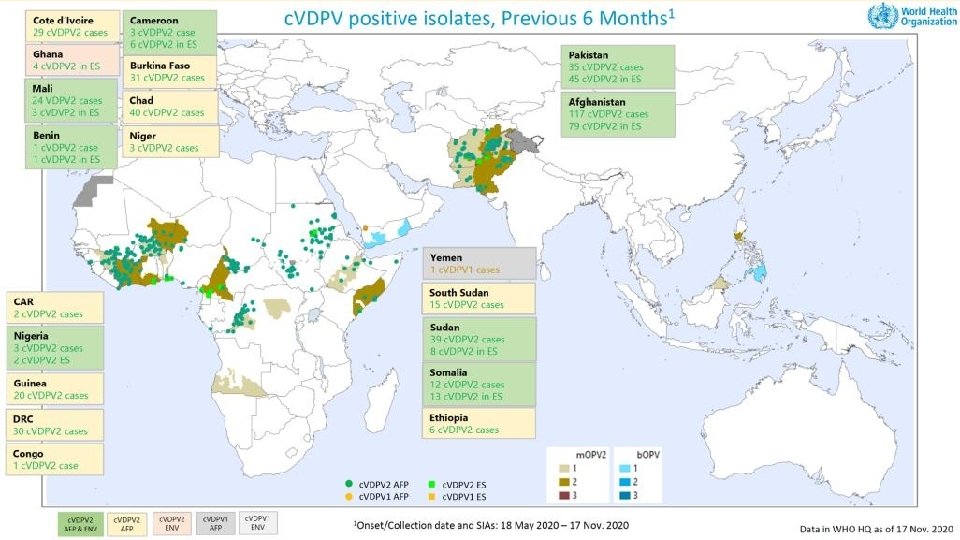
Developing immunity to polio Inactivated polio vaccine is 90%-95% effective in preventing disease but gives little protection against infection and onward transmission. Oral polio vaccine is effective at controlling an outbreak of polio, giving both protection against disease and blocking transmission. Continued use of oral polio vaccine carries two risks that are more significant than wild type disease when case numbers are very low. 1. Vaccine associated paralysis – approximately 1 in 2. 7 million doses of OPV. 2. Vaccine derived paralytic polio – occurs in populations where there is inadequate vaccination coverage. Over a period of several months to a year vaccine strains can circulate and revert to a more transmissible and pathogenic form by reverse mutation. Cases of c. VDVP now outnumber the number of cases caused by wild type polioviruses.




Country/ region Population million Area sq km Density per sq km Afghanistan 31. 39 645, 807 48. 61 Pakistan 211. 94 874, 209 242. 44 England 56. 29 130, 309 431. 95 Scotland 5. 46 77, 911 70. 12 Wales 3. 15 20, 736 152. 05 Northern Ireland 1. 89 13, 793 137. 29 Greater Manchester 2. 82 1, 277 2, 209. 87 Manchester 0. 55 116 4, 769. 22
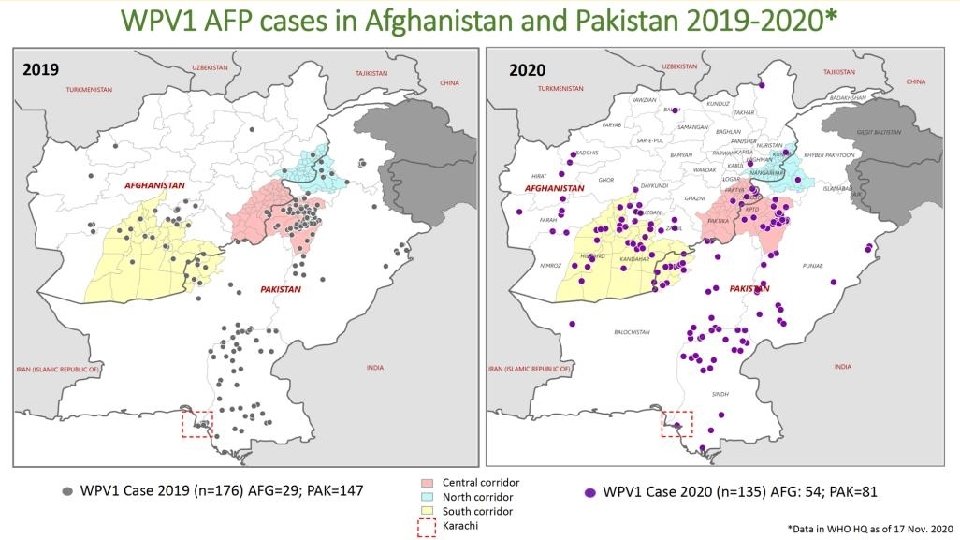

Notifications of new cases of wild polio type 1 paralysis 36

Afghanistan Pakistan 2019 2020 population 38 million 39 million 217 million 221 million children 0 -4 7. 4 million 7. 6 million 32 million 33 million live births 1. 2 million 6 million children reached in vaccination campaigns 43. 6 million 21. 9 million 188 million 108 million



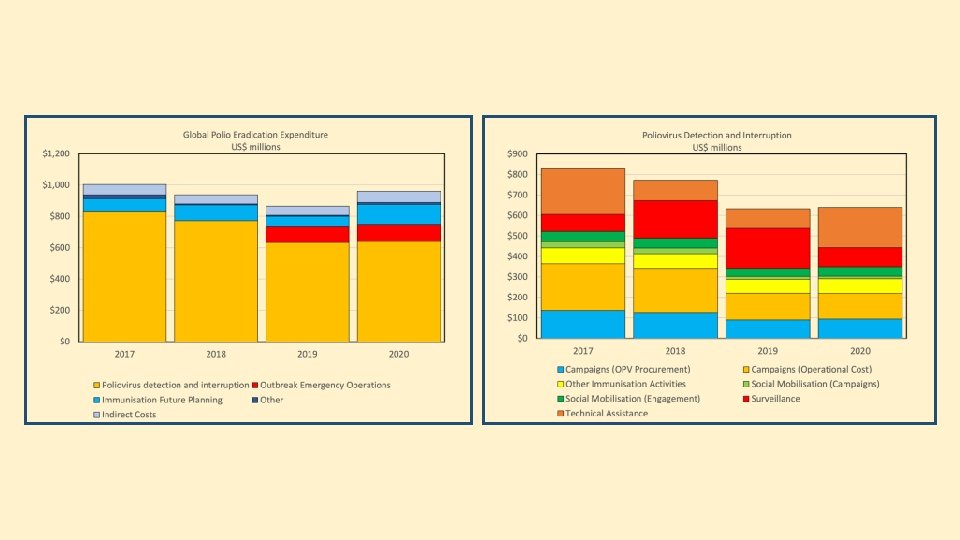
The Poliovirus Eradication Plan has Four Objectives 1 • Detect and interrupt all poliovirus transmission 2 • Strengthen immunization systems, introduce inactivated polio vaccine (IPV) and withdraw oral polio vaccines (OPV) 3 • Contain poliovirus and certify interruption of transmission 4 • Plan polio’s legacy 41
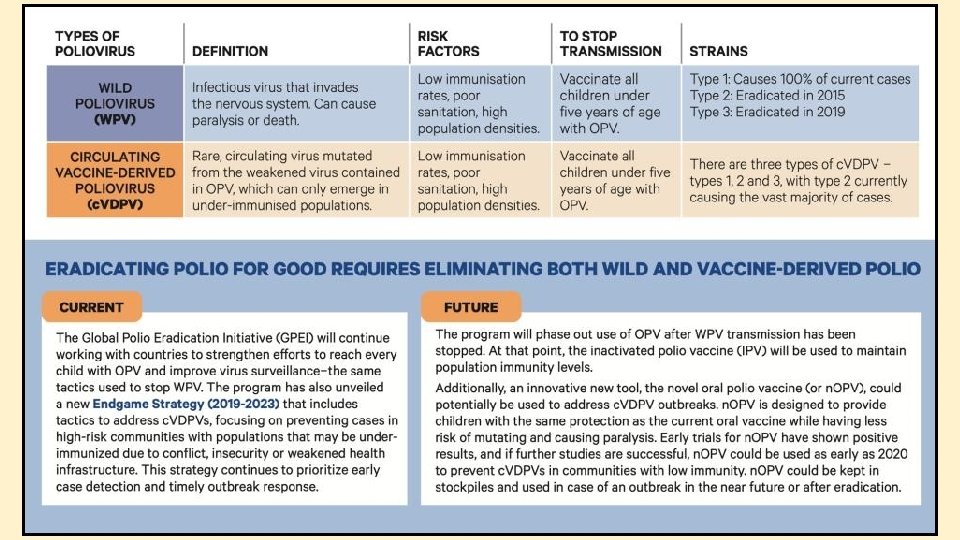

Novel oral polio vaccine n. OPV 2 • Modified version of the existing type 2 monovalent OPV (m. OPV 2 • Provides comparable protection against poliovirus while being more genetically stable and less likely to revert into a form which can cause paralysis in low immunity settings. • Increased genetic stability means there is a reduced risk of seeding new c. VDPV 2 outbreaks, compared to m. OPV 2.

Novel oral polio vaccine n. OPV 2 Will be deployed under WHO’s Emergency Use Listing procedure (EUL) for unlicensed vaccines to enable its rapid field availability. Even after meeting rigorous EUL criteria for safety and immunogenicity, n. OPV 2’s performance in the field will be closely monitored in line with EUL standards.

Surveillance is an Essential Component of the Eradication Strategy • Detection of all cases of acute flaccid paralysis followed by testing of two faecal samples taken 24 -48 hours apart withing 14 days of onset of paralysis in an accredited laboratory. • Testing of contacts of cases of suspected poliovirus paralysis. • Environmental sampling for polioviruses.

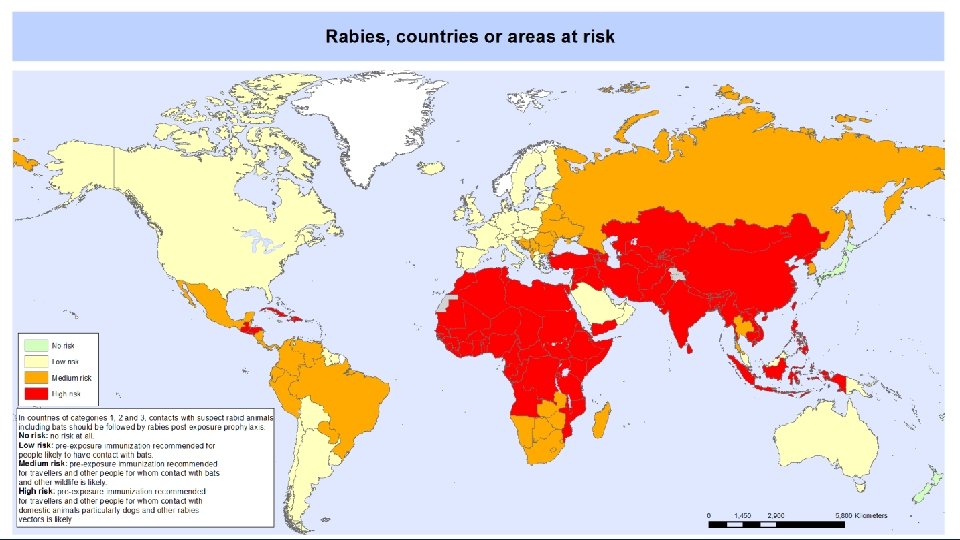
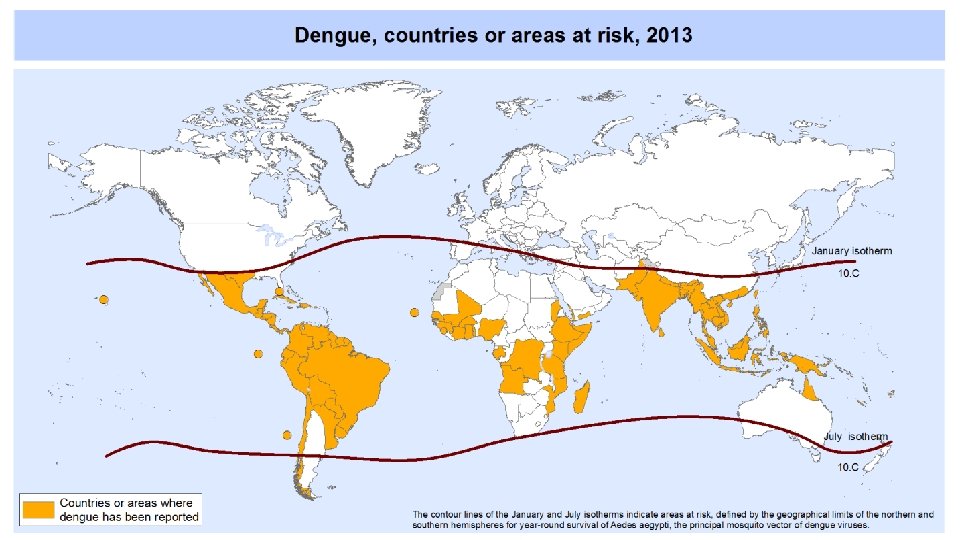
Emerging Infections Animal to human transmission • Direct transmission without human to human transmission – rabies • Transmission via an insect vector without human to human transmission – dengue • Genetic adaptation leading to spillover – Covid 19, HIV • Random mutation leading to antigenic change – seasonal flu • Genetic re-assortment leading to antigenic change and increased pathogenicity – pandemic flu, avian flu Host factors • Immunosuppression • Military action • Increased mobility – airflight • Mass migration – refugees Export of live animals • 11, 569, 796 individual live wild animals, representing 1, 316 different species exported from 189 different countries between 2012 and 2016. Environmental changes • Climate change • Deforestation • Urbanisation


1918 -19 Pandemic Flu approx 50 million deaths

2002 -03 SARS Co. V 8, 098 cases and 774 deaths
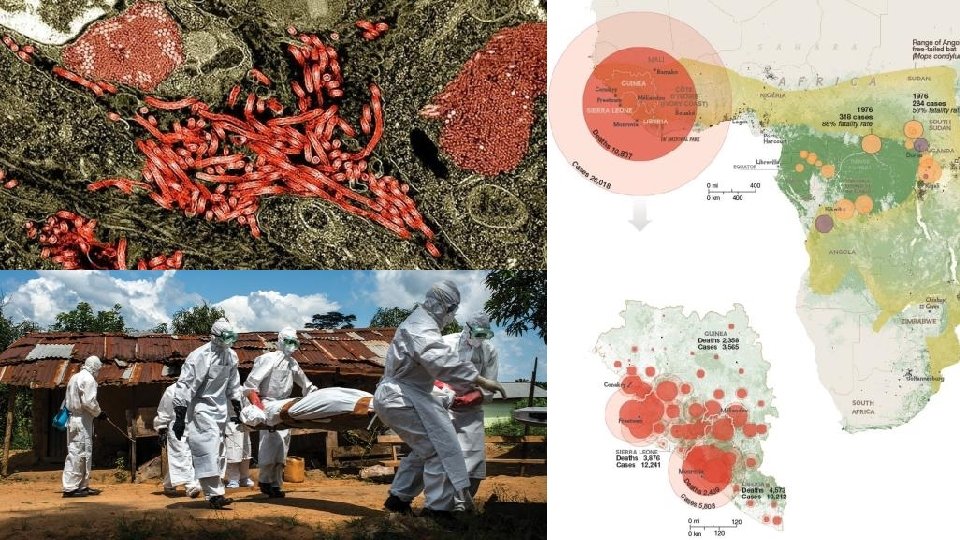

Most pandemics begin in the emerging disease hotspots of the world; the edges of forests in regions such as west Africa, the Amazon basin and south-east Asia. Tropical rainforests are home to a rich diversity of wildlife, which in turn carry an array of viruses. An estimated 1. 7 m viruses exist in mammals, birds and arthropods, but less than 0. 1% have been described.


Emerging Infections About one-third of emerging diseases are the product of rapid changes in land use, with as much as half of the world’s tropical forest transformed for agriculture and human settlement. People are thus pushed into contact with wildlife they would once have rarely encountered. Human activity has created a continuous cycle of viral spillover and spread.

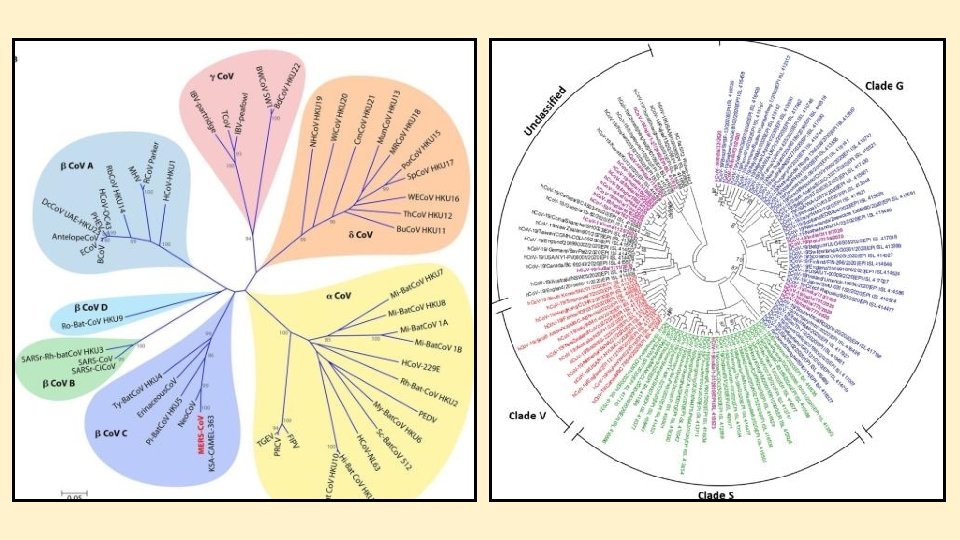
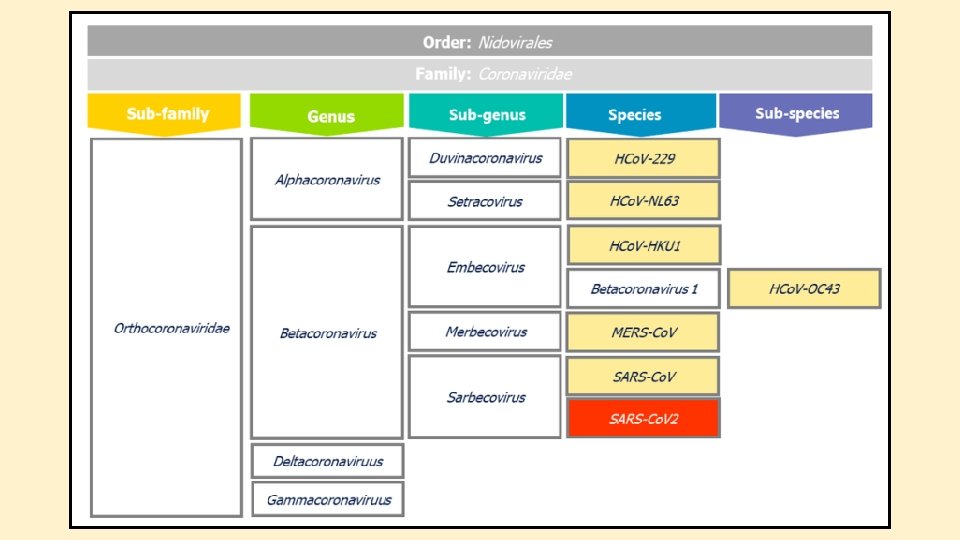
Coronaviruses • There are hundreds of coronaviruses, most of which circulate among such animals as pigs, camels, bats and cats. • Sometimes those viruses jump to humans — called a spillover event — and can cause disease. • Four of the seven known human coronaviruses cause only upper-respiratory tract illnesses like the common cold. • There are three highly pathogenic human coronaviruses SARS-Co. V (2002 -03), MERS (2012) and SARS-Co. V 2 (2019)

Human respiratory coronaviruses • Most people get infected with one or more of the respiratory viruses at some point in their lives. • They are usually spread from an infected person to others through the air by coughing and sneezing, close personal contact, like touching or shaking hands, touching an object or surface with the virus on it, then touching your mouth, nose, or eyes before washing your hands. • These viruses spilled over from bats or rodents into humans sometime in the past few hundred years via an intermediate mammalian species, usually domesticated.

Covid-19 transmission to mink • Seven countries are now reporting mink-related Sars-Co. V-2 mutations in humans, according to new scientific analysis. • The mutations are identified as Covid-19 mink variants as they have repeatedly been found in mink and now in humans as well. • Uncertainty around the implications of the discovery of a Covid-19 mink variant in humans led Denmark, the world’s largest mink fur producer, to launch a nationwide cull earlier this month.
 cellular entry Two cell membrane bound receptors are involved on")
SARS-Co. V 2 (Covid-19) cellular entry Two cell membrane bound receptors are involved on viral entry into the cell. • Activation – TMPRSS 2 – a protease enzyme • Attachment – ACE 2 – part of the angiotensin system for regulating blood pressure ACE 2 (angiotensin converting enzyme 2) receptors are found on cells in many organs including • Cells lining the respiratory tract and lungs • Arterial and venous endothelial cells • Smooth muscle cells in most organs • Cerebral cortex, hypothalamus and brain stem

World Population 7. 594 billion 25 November – 59, 877 cases and 1, 410, 082 deaths Europe Population 741. 4 million 23 November – 16, 888, 461 cases and 383, 213 deaths

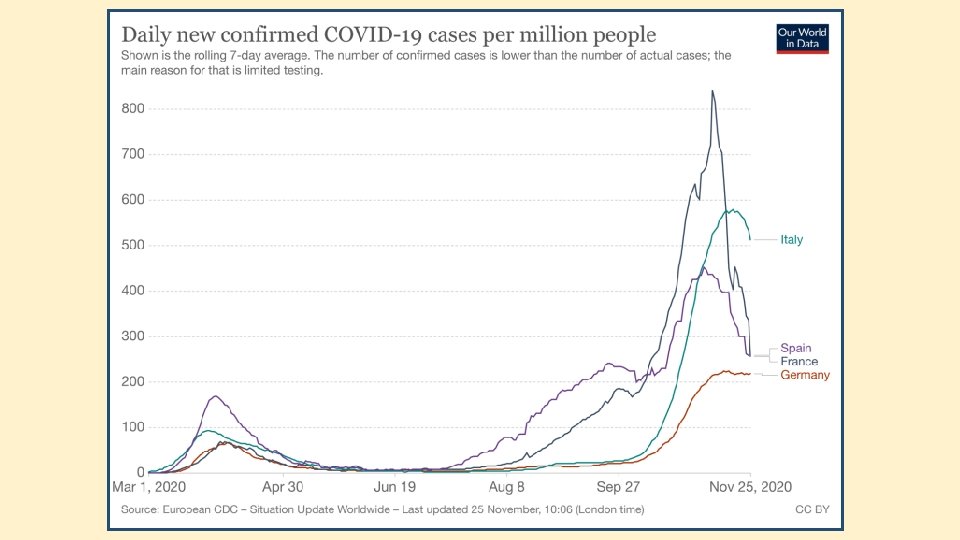
September 27 - October 11 October 25 - November 13 France – population 65. 27 million 25 November – 2, 153, 815 cases and 50, 237 deaths Italy – population 60. 46 million 25 November – 1, 455, 022 cases and 51, 306 deaths Spain – population 46. 75 million 25 November – 1, 594, 844 cases and 43, 668 deaths Germany – population 83. 78 million 25 November – 961, 320 cases and 14, 771 deaths

United Kingdom – population 67. 89 million 25 November – 1, 538, 794 cases and 55, 838 deaths Ireland – population 4. 9 million 25 November – 70, 930 cases and 2, 028 deaths

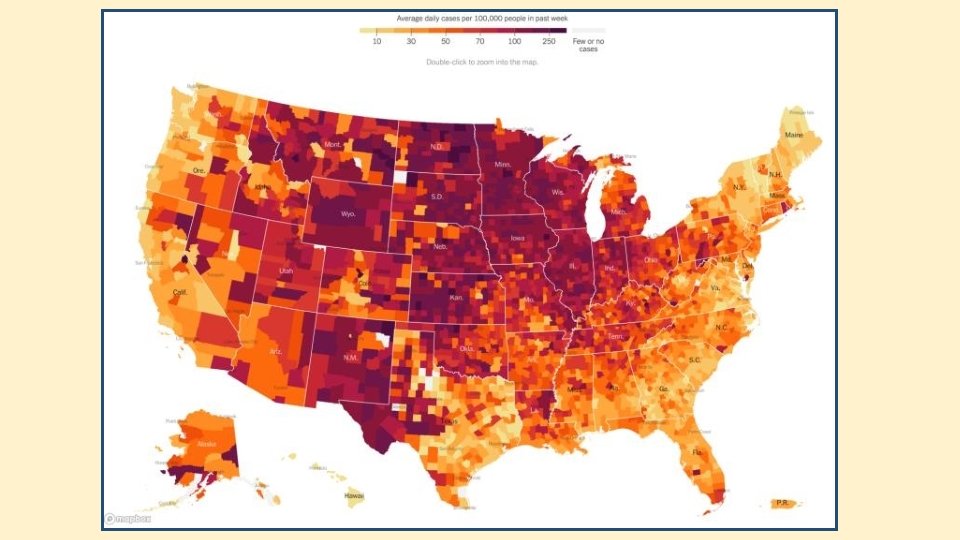
United States – population 328. 2 million 23 November – 12. 3 million cases and 257 thousand deaths

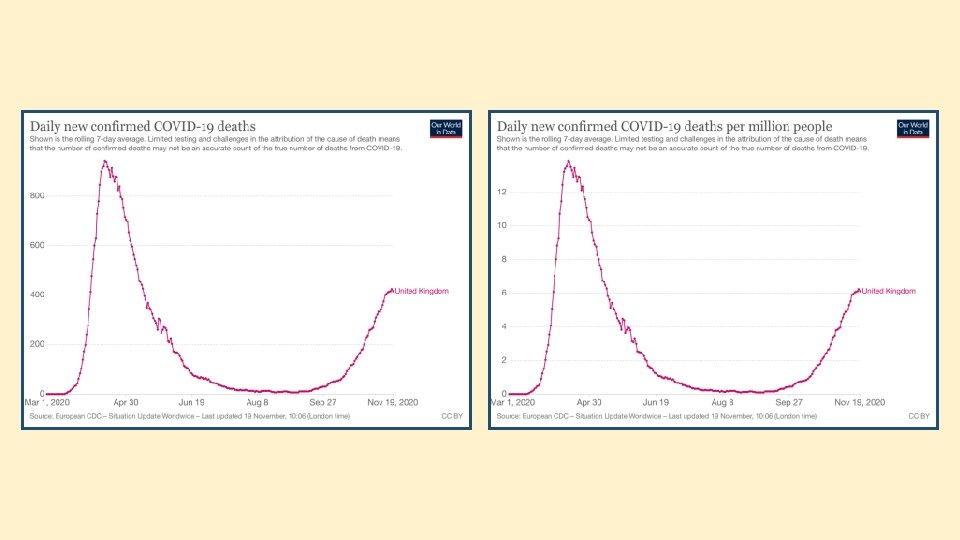
United Kingdom Mar-Oct 2020 – Covid-19 rate per 100, 000 w/e 1 Apr w/e 19 Aug w/e 29 Apr w/e 27 May w/e 24 Jun w/e 22 Jul w/e 16 Sep w/e 14 Oct w/e 11 Nov w/e 19 Nov

22 -28 June 10 -16 August

14 -20 September 9 -15 November

31 August – 13 September 21 September – 4 October 12 – 25 October 2 – 15 November

Covid-19 risk of infection The risk of infection is not the same as the risk of serious illness or death. Major risk factors are – The nature of the virus The means of transmission Duration of infectivity Living conditions – shared accommodation/multi occupier Number of contacts – communal activity Occupation

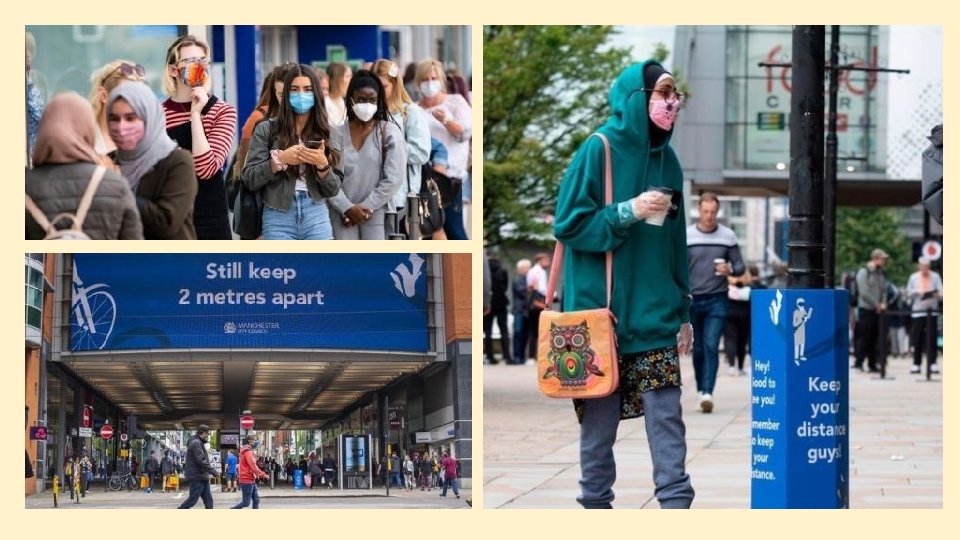
Covid-19 risk of infection We now understand how this virus spreads – through droplets, small aerosol particles and on surfaces – and that aerosols are probably the most significant transmission route. It spreads largely in indoor, crowded and unventilated settings, and even at a two-metre distance, you can still be infected indoors, as the virus can spread through the air and circulate for hours. Ventilating indoor spaces, wearing face coverings, distancing and getting outside for socialising and exercise are all essential to prevent transmission.

The phenomenon of overdispersion The R number is only an average, and this average masks an interesting phenomenon known in scientific circles as “overdispersion”. Overdispersion simply means that a minority of infected individuals are responsible for an unexpectedly high percentage of transmission. Roughly 10% of individuals infected with Covid are responsible for 80% of new infections Overdispersion in disease transmission mirrors overdispersion in patterns of social contact: a typical day for most of us might result in only a few contacts, but on some days we may see hundreds of people. Biological and environmental factors are important for overdispersion, too. Most people infected with Sars-Co. V 2 will start to transmit the virus unknowingly before

Superspreaders

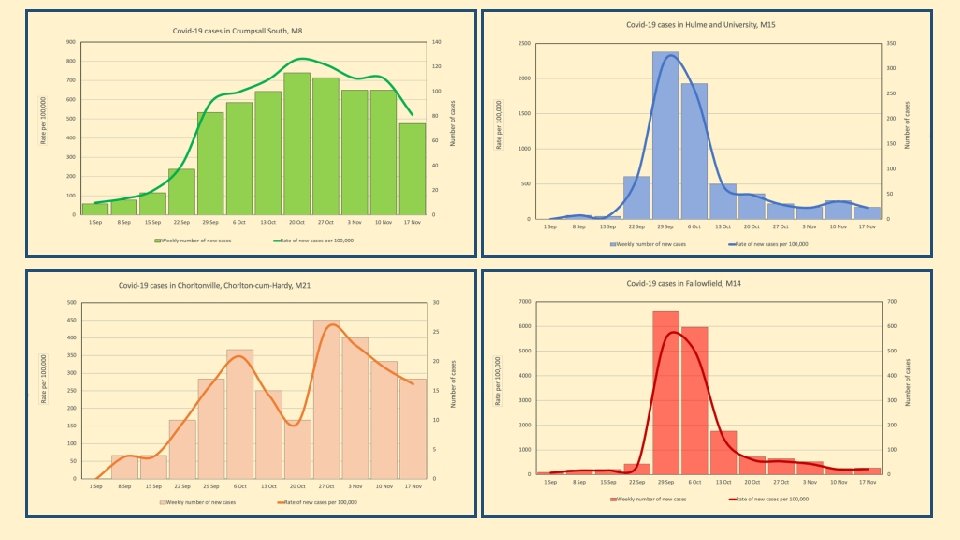
Week ending 8 September 2020 Week ending 29 September 2020 11 Oldham S 123 10 Crumpsall N 111 13 Salford C 86 26 Crumpsall N 288 5 Moston W 56 8 Hulme 55 122 Salford C 806 12 Droylsden C 127 20 Fallowfield 167 4 Chorlton 63 18 Oldham S 202 333 Hulme 2274 661 Fallowfield 5532 17 Chorlton 269 7 Didsbury 74 111 Didsbury 116 20 Newall G 242 3 Newall G 36 No cases Location Rate per 100, 000 15 Moston W 167 15 Droylsden C 159

Week ending 27 October 2020 Week ending 17 November 2020 54 Oldham S 605 62 Crumpsall N 687 94 Salford C 621 36 Crumpsall N 399 39 Moston W 434 31 Hulme 2122 52 Salford C 344 58 Droylsden C 615 64 Fallowfield 536 27 Chorlton 426 50 Oldham S 561 24 Hulme 164 27 Fallowfield 226 17 Chorlton 269 54 Didsbury 571 27 Didsbury 286 52 Newall G 629 92 Newall G 1112 No cases Location Rate per 100, 000 42 Moston W 467 34 Droylsden C 360




The Basic Reproduction Number R 0 = β ✕ D ✕ K β is the risk of transmission per contact (attack rate) D is the duration of infectiousness K is the number of contacts per unit time

More about Covid-19 transmission Organism characteristics • Infectivity • Duration of infectiousness • Mixing patterns • Demographics • Population density Population Characteristics May be different for the same virus in different populations For Covid-19 estimates vary from between 1. 4 to 4, with a mean of about 3. 5.

More about Covid-19 transmission • Covid-19 median incubation period 5 -6 days with a range of 2 -14 days. • Median pre-symptomatic infectious period varies for 1 -4 days following contact. • One study showed the median infectious period of asymptomatic cases was 6. 5 -9. 5 days. • Estimated mean time from onset of symptoms to two consecutive negative PCR tests was 13. 5 days, but was shorter when children and less sever case were involved. • Severe cases may shed virus for longer.

Covid-19 reducing infection risk – REDUCING ATTACK RATE Personal Protective Equipment • NHS staff, care workers & paramedics Social Distancing • risk is proportional to square of the distance between people Improved Ventilation • reduces risk of aerosol transmission Face coverings • chiefly for protecting others Hand washing • protects against surface contamination with respiratory droplets Screens • counter staff in shops, banks and bars etc. Hospitality Venues • curfew, table service only, rule of 6

Covid-19 reducing infection risk – REDUCING TRANSMISSION Case Detection • as soon as possible after onset of symptoms – optimally within 1 day • sensitivity and precision of tests, confirmatory assays • speedy notification of results Contact Tracing • timely – optimally within 1 day • completeness – optimally at least 80% of contacts • use of mobile apps Self Isolation of Mild or Symptomless Cases Hospitalisation of Very Sick Cases Self Isolation Following Contact Quarantine of Travellers

Covid-19 reducing infection risk – REDUCING THE NUMBER OF CONTACTS Lockdown School Closures Closure of Shops Closure of Pubs and Restaurants Closure of Places of Worship Restrictions on Travel Restrictions on Social and Sporting Gatherings

Covid-19 testing Mass testing in the community is important, because it helps us identify as many infectious people as possible, even if they don’t have symptoms. Lab testing based on PCR is a reliable way of identifying carriers, even at low viral doses, it is time- and labour-intensive. There are now rapid antigen tests that can give results within 30 minutes for just £ 3. 90 each. The WHO has already acquired 120 m of these tests for poorer countries that struggle with lab capacity. Testing is one of the key ways to control this virus. The playbook in east Asian and Pacific countries, which have largely eliminated transmission and dealt quickly with flare-ups, involves testing, tracing and isolation, strict border measures, good voluntary guidance and – sparingly used – lockdowns.

Covid-19 testing In the UK, the government plans to roll out mass, cheap testing in the coming months that will help identify carriers of the virus who then need to be supported to isolate. One limitation of testing is that the incubation period of the virus is long, up to 14 days – so testing people repeatedly will be necessary to pick up those who are infected. We now have decent antibody tests that can identify whether someone has had Covid recently. These have shown us that the antibody response to Covid lasts about 12 weeks. Seroprevalence, the proportion of people with antibodies, is low across most countries, and even in certain boroughs of New York City where 50%+ antibody prevalence is reported, the epidemic is still accelerating, dashing hopes that “herd immunity” could be achieved once a certain number of people have been infected.


Effective reproduction number R • Average number of secondary infections produced by a typical infective index case where a proportion of the population are immune Pi. • In a homogeneously mixing population R = R 0(1 -Pi) Examples • R 0=3. 5, Pi = 0. 5, R = 1. 75 • R 0=3. 5, Pi = 0. 6, R = 1. 4 • R 0=3. 5, Pi = 0. 7, R = 1. 05 • R 0=3. 5, Pi = 0. 8, R = 0. 7
 and vaccine impact (Vi) Incidence of disease in unvaccinated = Vu")
Vaccine efficacy (Ve) and vaccine impact (Vi) Incidence of disease in unvaccinated = Vu Incidence of disease in vaccinated = Vv Ve = 100((Vu-Vv)/Vu) Incidence before vaccine introduced = Iu Incidence after vaccine introduced = Iv Vi = 100(Iu-Iv) Number of doses required is important

Calculating susceptibility of a cohort Proportion of cohort unprotected by vaccine as a percentage where % vaccine efficacy after 1 dose = Ve Initially susceptible (0 doses) = 100% Susceptible after 1 dose = (100 -Ve)% Susceptible after 2 doses = (100+Ve 2/100 -2 Ve)%

Covid-19 vaccines 164 candidate vaccines in preclinical evaluation 48 candidate vaccines in clinical evaluation 10 types of vaccine • live attenuated • Inactivated • protein subunit • virus like particle • replicating viral vector • non-replicating viral vector • replicating bacterial vector • DNA • RNA • T-cell based

Oxford/Astra. Zeneca Covid-19 vaccine Ch. Ad. Ox 1 n. Cov-2019 coronavirus vaccine The vaccine is a chimpanzee adenovirus vaccine vector, which has been shown to generate a strong immune response from a single dose. It is a harmless, weakened adenovirus that usually causes the common cold in chimpanzees, and which has been genetically changed so that it is impossible for it to grow in humans. The genetic sequence of this surface spike protein has been inserted into the virus vector. When the vaccine enters cells inside the body, it uses this genetic code to produce the surface spike protein of the coronavirus. Vaccine efficacy has been assessed based on analysis of data from the COV 002 Phase II/III trial in the UK and COV 003 Phase III trial in Brazil. Over 23, 000 participants have been assessed following two doses of either a half-dose/full-dose regimen or a regimen of two full doses of vaccine.

Covid-19 vaccines Pfizer-Bio. NTech RNA vaccine Moderna RNA vaccine • 2 injections 21 days apart • 2 injections 4 weeks apart • 90% effective • 95% effective • Store at -75 C or below • Store at -20 C up to 6 months Oxford/Astra. Zeneca vaccine has been shown in trials to have an average efficacy of 70% after a two doses at least one month apart. The vaccine efficacy was 90% in about 2, 741 people who were accidentally given a half dose at first followed by a full dose 4 weeks later. Efficacy was only 62% in 8, 895 people in the larger trial who were given 2 full doses 4 weeks apart. The vaccine was shown to trigger a robust immune response in
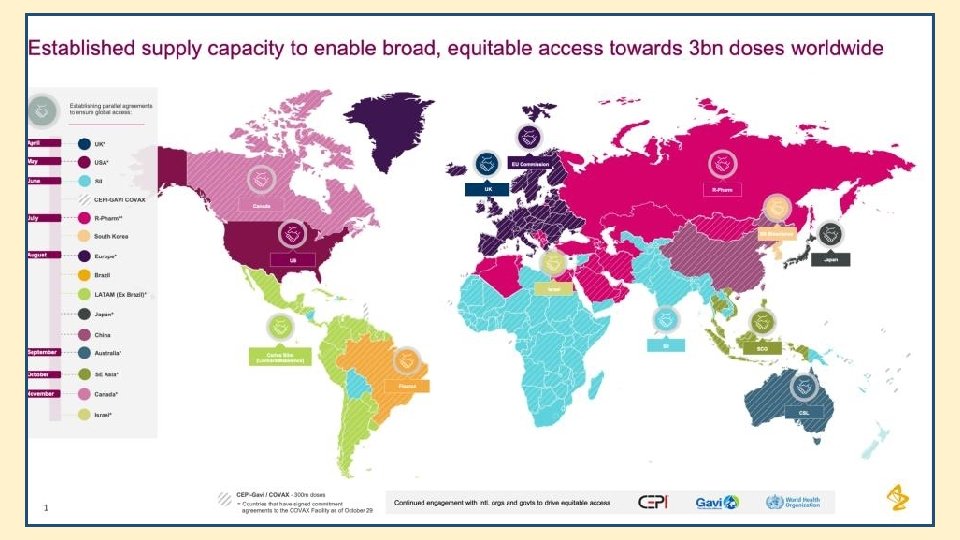

Covid-19 vaccines ordered by UK Gov 100 million doses of University of Oxford/Astra. Zeneca vaccine – phase 3 clinical trials 40 million doses of Bio. NTech/Pfizer vaccine – phase 3 clinical trials 60 million doses of Novavax vaccine – phase 3 clinical trials 60 million doses of Valneva vaccine – pre-clinical trials 60 million doses of GSK/Sanofi Pasteur vaccine – phase 1 clinical trials 30 million doses of Janssen vaccine – phase 2 clinical trials 5 million doses of Moderna vaccine – phase 3 clinical trials

Covid-19 vaccines – THE CHALLENGE Vaccines don’t save lives, but vaccination does. Following successful clinical trials the next challenge is to produce vaccines in large quantities. Product safety testing will still be essential. Unknowns still include actual efficacy, duration of immunity, age related response rates, adverse events. Who should the vaccine be given to first depends upon the agreed strategy – will the vaccine be used to eliminate, suppress or mitigate the virus? When a covid-19 vaccine has been produced in sufficient quantity delivery will depend on a complex supply chain – the same as the one that left parts of the world in desperate need of things like disposable gloves and protective equipment just months ago.



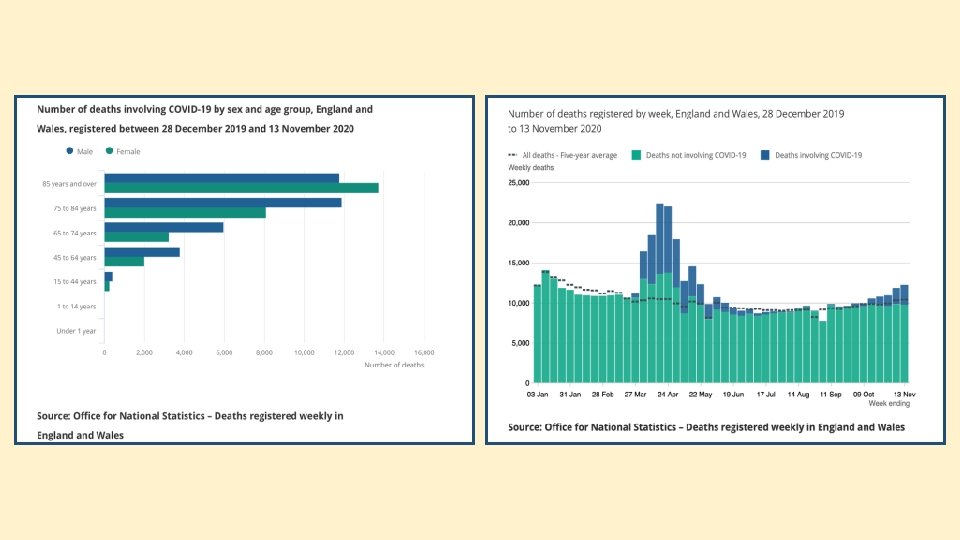
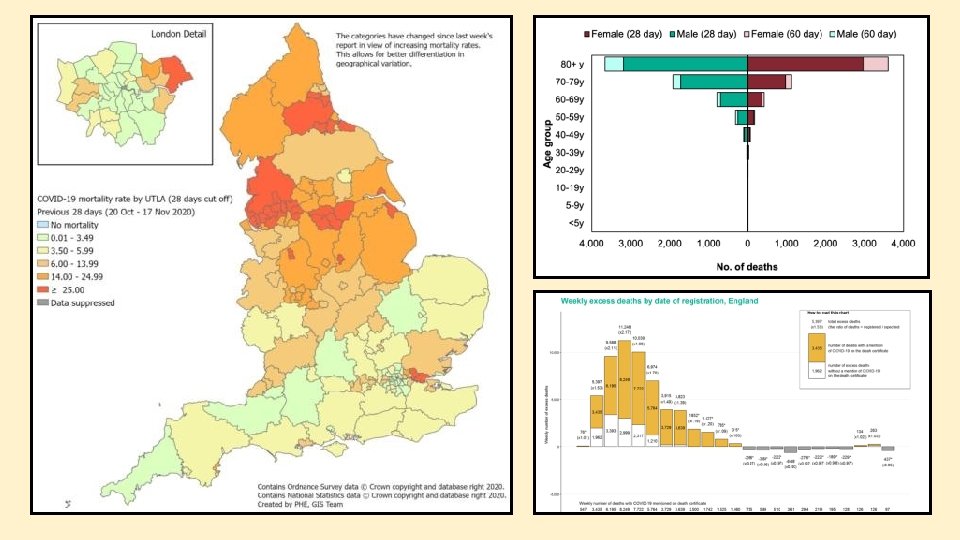
Covid-19 risk of mortality Mortality rates are difficult to compare between countries because of different recording methods. Case relation mortality is not the same as infection related mortality. Major risk factors are – Age Gender Occupation Co-morbidities Obesity Standards of health care
- Slides: 113