PICORNA VIRUSES Proff M Banerjee INTRODUCTION Large number

PICORNA VIRUSES Proff. M. Banerjee

INTRODUCTION • Large number of very small RNA viruses. • Non enveloped , 27 -30 nm. • Resistant to ether and other lipid solvents. • 2 main gps- Enteroviruses • - Rhinoviruses which may found in alimentary tract or nasopharynx. .

CLASSIFICATION • 4 genera of medical importance • ENTEROVIRUS – infects the intestinal tract • RHINOVIRUS – infects the nasopharynx • HEPATOVIRUS • PARECHOVIRUS – gastroentetinal and respiratory dis in infants (sepsis like picture)

• Veterinary imp. • Aphthovirus – foot and mouth disease • Cardiovirus- encephalomyocarditis of mice

ENTEROVIRUS • Paralytic disease of children known from very early times • Experimental transmission of the disease to monkey – Landsteiner and popper. • Growth of polio Vs in non- neural cells from human embryos , producing cytopathic effect – Enders, Weller and Robbins (1949) – Nobel prize

ENTERO VS OF MEDICAL IMPPORTANCE • Poliovirus types 1 -3 • Coxsackievirus A types 1 -24 (not included: 15, 18 & 23) • Coxsackievirus B types 1 -6 • Echo virus 1 -34 (types not included: 8, 10, 22, 23, 28 and 34 ) • Enterovirus types 68 -116( types not included ; 72)

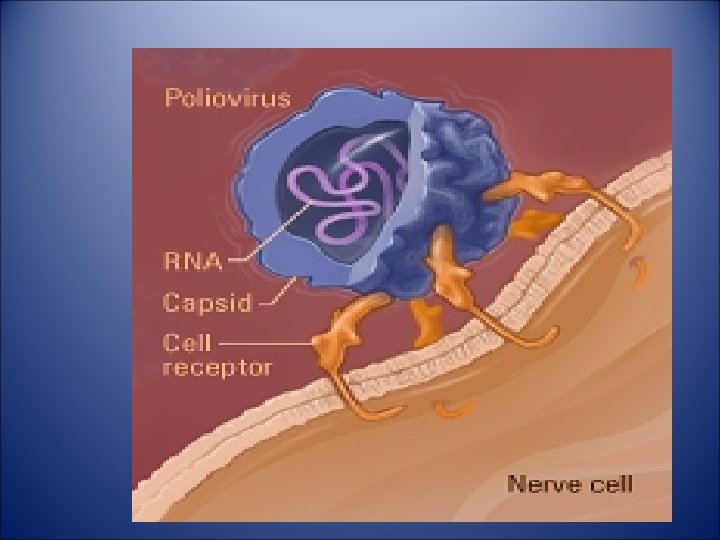
POLIOVIRUS

MORPHOLOGY • Spherical particle , approx. 27 nm in. D. • Composed of 60 subunits. • Each consisting of 4 viral proteins (VP 1 VP 4) arrange in icosahedral symmetry. • VP 1 faces outside , Major Agic site for type specific neutralising Abs. • • VP 1, VP 2, and VP 3 particles are on the surface of the capsid • whereas the VP 4 particle is inside the capsid.

• Genome is single stranded positive sense RNA of 7. 4 kb. This genome is infectious

LIFE CYCLE OF POLIO VIRUS • The main steps in the life cycle of the virus are following: • • ENTRY IN THE HOST: • • ATTACHMENT WITH THE HOST CELL: • • REALEASE OF THE RNA: • • PRODUCTION OF NEW VIRIONS: • • RELEASE OF NEW VIRIONS: • • ATTACK ON NERVE CELLS

1. ENTRY IN THE HOST • Polio virus enters the host through oral to oral route or • through oral to fecal route. The route which is more frequent is through oral to fecal route. It enters through mouth and reaches to the intestines of the host.

2. ATTACHMENT WITH THE HOST CELL • A number of cells throughout the body have on their surface a poliovirus receptor (PVR). This receptor is composed of protein called immunoglobulin and is the site where poliovirus binds to host cells. • PVR has three different loops, and poliovirus binds to the first of these loops.

3. REALEASE OF THE RNA • • The virus either injects its RNA by making a hole in the plasma membrane or gets entry in the cell by endocytosis. • • When it injects the RNA in the cell first it makes a hole in the membrane and then injects its RNA. • • And when it gets entry in the cell, it first decoats.

PRODUCTION OF NEW VIRIONS • Poliovirus is a positive stranded RNA virus. Thus the genome enclosed within the viral particle can be used as messenger RNA and immediately translated by the host cell. • • On entry the virus hijacks the cell's translation machinery, causing inhibition of cellular metabolism

• protein synthesis in favour of viral specific protein production. • Poliovirus m. RNA is translated as one long polypeptide. • The polyprotein is cleaved, yielding mature viral proteins. The positivesense RNA • serves as template for complementary negative-strand synthesis.

• When polyprotein is cleaved it forms P 1 P 2 and P 3 precursors. • P 1 forms the capsid proteins and the remaining two precursors forms the genome of the virus. • The encapsulations of the genome results into the formation of new virions.

• If these virions enter into the blood stream they reach the spinal cord/brain

RESISTANCE • R to ether, chloroform, bile, proteolytic enzymes of intestinal contents & ditergents. • Stable at Ph 3. • In feces can survive for months at 4 C. & Years at -20 C • Depending on envirenment can survive at RT from 1 D to several WKs in feces.

• Heat – inactivate vs at 55 C X 30 mins. • Molar Mg. Cl 2 protect the Vs against heat inactivation, milk or ice cream also protect. • Formaldehyde and oxidising disinfectants also destroy. • Phenolic agents are not effective. • Does not survive lypholization

ANTIGENIC TYPES • Three antigenic types • Type-1 – most common , causes most epidemics • Type-2 - usually cause epidemic infection • Type-3 - strain have caused epidemics, immunity is type specific
- can be")
• 2 antigens C and D (C-coreless or capsid, D- dense)- can be recognise by CFT , ELISA or precipitation test. • D antigen –Native or N antigen, associated with whole virion and is type specific • C-antigen- heated or H antigen , associated with”empty” non infectious virus, Anti-c. Ab does not neutralise virus infectivity & is not protective

• D antigen convert into C antigen by heating the virus at 56 C. • Anti-D antibody is protective. Potency of injectable polio vaccine can be measured in terms of D antigen units.

HOST RANGE AND CULTIVATION • Natural infection only in humans. • Experimental – Chimpanzees, cynomolgus monkeys – by intracerebral, intraspinal or by oral route. • Rapidly grow- primary monkey kidney cultures , or continuous culture from human tissue – used for isolation , vaccine production.

• In cell culture- cells round up, refractile, pyknotic, eosinophilic intranuclear inclusion bodies by stained preparation. • Well formed plaque – in infected monolayer.

U. S. Centers for Disease Control and Prevention Poliomyelitis U. S. Centers for Disease Control and Prevention http: //www. immune. org. nz/site_resources/Professionals/Diseases/Polio. jpg

Poliomyelitis is an infection of the CNS • poliós -Greek word “grey”, + myelós “spinal cord’ + suffix – itis “inflammation =poliomyelitis • Viral infection of the nerves of the CNS

Transmission by fecal-oral route http: //www. co. washington. or. us/HHS/Environmental. Health/Public. Pools/

Risk Factors – Not being vaccinated in areas where polio is common – infants, pregnant women, immunocompromised (eg. HIV)

WHO, 2008.
,")
Three basic patterns • Subclinical infection(95% of infections),
, • Nonparalytic poliomyelitis(1 -2%)")
Three basic patterns • Subclinical infection(95% of infections), • Nonparalytic poliomyelitis(1 -2%)
, Nonparalytic poliomyelitis(1 -2%) Paralytic poliomyelitis(0.")
Three basic patterns • • Subclinical infection(95% of infections), Nonparalytic poliomyelitis(1 -2%) Paralytic poliomyelitis(0. 1– 0. 5%) -result of accidental transfer of virus from GI tissue to neural tissue – Spinal polio - 79% of paralytic cases— Bulbospinal polio - 19% of paralytic cases— Bulbar polio - 2% of paralytic cases

– poliovirus enters digestive tract via mouth – Primary site of infection is epithelial and lymphoid tissue associated with the oropharynx and gut • Virus production at this site leads to a transient viremia, following which the virus may infect the CNS http: //cmbi. bjmu. edu. cn/www-learn/micro-ac-uk/335/Picornaviruses. html

• Multiply in reticuloendothelial system Vs again enter the blood stream ( Sec viremia) – carried to spinal cord and brain. • Pass along the axon of peripheral nerves to CNS. • In CNS vs multiplies in neurons and destroy them. Earliest change degeneration of Nissl bodies.

• Lesions are mostly in anterior horn cells of spinal cord. Causing flaccid type of paralysis. • In some cases encephalitis may occur.

Dual Tropism Thought to be the Cause of Poliomyelitis from Poliovirus • Reflects the distribution of the poliovirus receptor CD 155 on cells lymphoid cells as well as the epithelial cells in the gut and on neurons in the CNS • Viral Tropism relies on host cell permissiveness and receptor susceptibility

Virus Replicates Through Viropexis – attachment of the virus to specific cellular receptors of cells with CD 155 – penetration and uncoating of the virus is energy dependent, and occurs by receptormediated endocytosis (viropexis)

SYMPTOMS OF POLIO • COMMON SIGNS AND SYMPTOMS OF POLIO • SYMPTOMS INCLUDE FEVER, SORE THROAT, AND NAUSEA. UP TO 95 PERCENT OF PEOPLE WHO ARE INFECTED WITH POLIOVIRUS WILL HAVE NO SYMPTOMS.

• THIS PERIOD BETWEEN POLIO TRANSMISSION AND THE START OF SYMPTOMS IS CALLED THE "POLIO INCUBATION PERIOD. " THE INCUBATION PERIOD FOR POLIO CAN BE AS SHORT AS 4 DAYS OR AS LONG AS 35 DAYS.

POLIO OUTCOMES AND THEIR RATIO • OUTCOMES • No symptoms • Minor Illness • Non paralytic aseptic meningitis • Paralytic polio • PROPORTION OF CASES • 95 -90% • 4 -8% • 1 -2% • 0. 1 -0. 5%

• spinal polio • 79% of paralytic cases • bulbospinal polio • 19% of paralytic • bulbo polio cases • 2% of paralytic cases

TYPES OF POLIO • • The types of polio are briefed below Non-paralytic polio Post-polio syndrome

NON PARALYTIC POLIO • Some people who develop symptoms from the poliovirus contract non-paralytic polio — a type of polio that doesn't lead to paralysis (abortive polio). • • Signs and symptoms, which generally last one to 10 days, include:

• Fever , sore throat , headache , vomiting • Fatigue , Back pain or stiffness , Neck pain or stiffness • Pain or stiffness in the arms or legs • Muscle weakness or tenderness

• In rare cases, poliovirus infection leads to paralytic polio, the most serious form of the disease.
 • brainstem (Bulbar polio) • or both (Spino-bulbar")
• spinal cord (Spinal polio) • brainstem (Bulbar polio) • or both (Spino-bulbar polio)

PARALYTIC POLIO S/S of paralytic polio. Loss of reflexes Severe muscle ache or weakness Loose and floppy limbs (Flaccid paralysis) often worse on one side of body • These signs often mimic those of nonparalytic , after two to three weeks the typical signs of paralytic polio appear • •

POST POLIO SYNDROME • Post-polio syndrome is a cluster of disabling signs and symptoms that affect some people • several years — an average of 35 years — after they had polio. Common signs and symptoms • include: • Progressive muscle or joint weakness and pain

• • General fatigue and exhaustion after minimal activity • • Muscle atrophy • • Breathing or swallowing problems. • • Sleep-related breathing disorders, such as sleep apnea • • Decreased tolerance of cold temperatures • • Cognitive problems, such as concentration and memory difficulties
 CSF Blood")
LABORATORY DIAGNOSIS • • SPECIMENThroat swab and feces (rectal swab) CSF Blood

• VIRAL ISOLATION • Blood- primary vireimia , 3 -4 days after inf. Usually not done. • Throat swab- early stage of disease • Feces –Possible in 80% of Pt. in 1 st Wk. 50% in till 3 rd Wk, 25% till 6 th Wk. • CSF- Seldom isolated

• SERODIAGNOSIS – • Neutralization or CFT in paired sera. • Abs soon appear after the onset of paralysis, persist for life. • CFT for Anti C Ab – appear first & disappear early. Anti D Ab – takes Wks to appear last for abt 5 yrs.

• MOLECULAR DIAGNOSIS • Reverse Transcriptase PCR • Sequencing

IMMUNITY • Type specific and permanent • Humoral Antibodies • . Circulating Igm- within wk of inf, lasts for abt 6 mnths. - protects Vs of same serotype , not prevent inf of intestinal epith. and Vs shedding in feces. Abs cannot protect once the infection spread to CNS

• Vaccination must prior to infection. Secretory Ab – Ig. A- Mucosal immunity, prevent intestinal inf & viral shedding. • Breast milk Containing Ig. A Abs protect infant from infection. •

POLIO VACCINE • The vaccine for the cure of polio is available. • TYPES OF POLIO VACCINE: • There are two types of polio vaccine: • • Inactivated polio vaccine • • Oral polio vaccine

Only IPV used in US today – OPV known to in rare cases become virulent and cause iatrogenic (vaccine-induced) polio – Both used today in the world – IN US, only IPV used since 1990 s from policy changes – Only cases of polio (8 -10 per year) were from people with vaccine-induced polio
 Albert Sabin – oral live attenuated virus (OPV) 1952")
Jonas Salk- Injected Poliovirus Vaccine(IPV) Albert Sabin – oral live attenuated virus (OPV) 1952 1957
, is based on")
• The Salk vaccine, or inactivated poliovirus vaccine • (IPV), is based on three wild virulent, strains, type • 1 poliovirus, type 2 poliovirus, and type 3 poliovirus • which are then inactivated with formalin • .

• The injected Salk vaccine confers mediated immunity in the bloodstream, which prevents polio infection from progressing to vireimia and protects the motor neurons, thus eliminating the risk of bulbar polio and post polio syndrome

ORAL POLIO VIRUS • OPV consists of a mixture of live attenuated poliovirus strains of each of the three serotypes, selected by their ability to mimic the immune response following infection with wild polioviruses, • but with a significantly reduced incidence of spreading to the central nervous system.
 is two-pronged. • OPV produces")
• The action of oral polio vaccine (OPV) is two-pronged. • OPV produces antibodies in the blood ('humoral' or serum immunity) to all three types of poliovirus, and in the event of infection, this protects the individual against polio paralysis by • preventing the spread of poliovirus to the nervous system.
 •")
VACCINATION SCHEDULE • 1 - Killed vaccine-inactivated or injectable polio vaccine – (IPV) • 1 st dose- after 6 months , maternal Abs should not enerfere. • 2 nd dose – 4 -8 wks apart • 3 rd dose – 6 -12 months later , • Booster dose – 3 -5 yrs thereafter

• Sabin’s live attenuated vaccine– immunises by active multiplication. • Stimulate systemic production of Ig. M , Ig. G and scretory Ig. A in intestine. • In india OPV contains Type 1 Vs 10 lakhs, Type 2 – 2 lakhs, Type 3 – 3 lakhs • Prepared by growing attenuated strain in monkey kidney cells.

• Rarely – OPV leads to vaccine associated paralytic polio or vaccine derrived polio virus(VDPV). • Caused by genetically changed polio Vs in intestine from original attenuated vaccine strain. • Doses- 3 doses , 4 -8 wks interval. In some areas eg in tropics may increase to 5 doses.

• OPV is not safe in immunocompromised or immunodefficient subjects. But IPV is safe.

Accusation now debunked, but stigma lingers for new reasons – New reasons for vaccination stigma such as rumors of sterility in some areas

Present Treatments Offer Relief to Symptoms – No current cure – Respiratory apparatus – Antibiotics for UTIs, medication for urine retention – Heating pads and towels for muscle spasms & pain – Physical therapy, braces, or orthopedic surgery for recovery of muscle strength/function

What still needs to be done • Eradication efforts – Get rid of stigma surrounding vaccine in Africa and other polio-afflicted places – Develop new targets for polio cure
- Slides: 70