PHYSIOLOGY OF LIVER GALL BLADDER PART 2 DR

PHYSIOLOGY OF LIVER & GALL BLADDER – PART - 2 DR. M. M. KHAN PROF. & HEAD, PHYSIOLOGY

PHYSIOLOGY OF LIVER & GALL BLADDER – PART – 1 1. Functional Anatomy of Liver & Gall Bladder 2. Histology of Liver ---- Hepatic Lobule 3. Blood Flow through Liver 4. Properties of Bile Juice 5. Composition of Bile Juice 6. Enterohepatic Circulation 7. Functions of Bile Juice 8. Functions of Liver 9. Regulation of Secretion of Bile 10. Synthesis of Bile Pigments (Bilirubin) --- Fate of Haemoglobin

PHYSIOLOGY OF LIVER & GALL BLADDER – PART – 2 1. Synthesis of Bile Pigments (Bilirubin) --- Fate of Haemoglobin 2. Applied of Liver : (a) Jaundice, or, Icterus (b) Hepatitis (c) Liver Cirrhosis (d) Liver Failure, or, Hepatic Coma 3. Physiology of Gall Bladder : (a) Its Functional Anatomy (b) Functions of Gall Bladder (c) Regulation of Gall Bladder Contraction & Bile Evacuation (d) Applied of Gall Bladder : (i) Gall Stones (ii) Cholecystitis
 ( FATE OF HAEMOGLOBIN )")
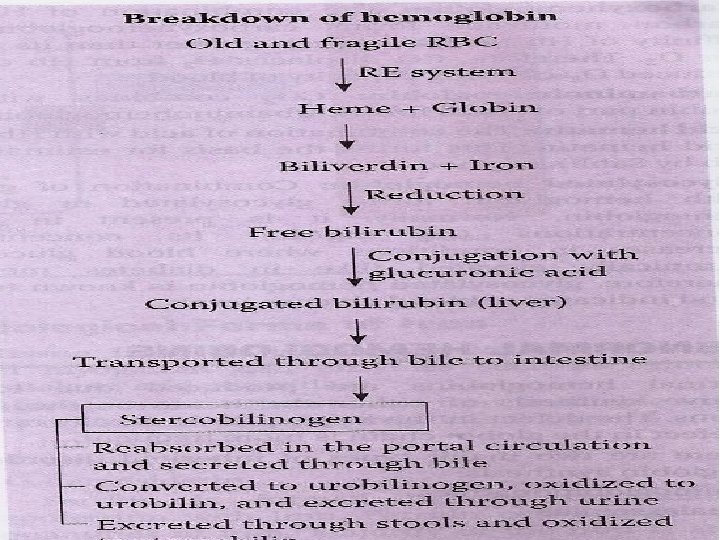
1. SYNTHESIS & CIRCULATION OF BILE PIGMENTS (BILIRUBIN) ( FATE OF HAEMOGLOBIN )
 Jaundice, or, Icterus (b) Hepatitis (c) Liver Cirrhosis")
2. APPLIED ASPECTS OF LIVER (a) Jaundice, or, Icterus (b) Hepatitis (c) Liver Cirrhosis (d) Liver Failure, or, Hepatic Coma
![[A. ] JAUNDICE , OR , ICTERUS : • It is a condition with](http://slidetodoc.com/presentation_image_h/14dfb49a89ff717654fc94b6860ad903/image-7.jpg "[A. ] JAUNDICE , OR , ICTERUS : • It is a condition with")
[A. ] JAUNDICE , OR , ICTERUS : • It is a condition with yellow discoloration of skin , mucous membrane, bulbar conjunctivae and deeper tissues of body --- due to increased level of bilirubin in blood. • - Normal serum bilirubin : 0. 5 to 1. 5 mg / 100 ml of blood. • - Subclinical, or, Latent jaundice : when serum bilirubin is > 1. 5 … upto 2 mg / 100 ml of blood. • - Clinical jaundice : when serum bilirubin is > 2 mg / 100 ml of blood.
 Unconjugated hyperbilirubinemia : (when uncojugated bilirubin is increased")
TYPES OF JAUNDICE : (I. ) Unconjugated hyperbilirubinemia : (when uncojugated bilirubin is increased in blood) (1. ) Pre - Hepatic, or Hemolytic - jaundice (2. ) Physiological Neonatal jaundice (3. ) Criggler Najar Syndrome (II. ) Conjugated hyperbilirubinemia : (when cojugated bilirubin is increased in blood) (3. ) Hepatic, or Hepatocellular – jaundice (4. ) Post - hepatic, or Obstructive , or Surgical - jaundice
 PRE- HEPATIC, OR, HEMOLYTIC - JAUNDICE - It is Due to")
(1. ) PRE- HEPATIC, OR, HEMOLYTIC - JAUNDICE - It is Due to excessive hemolysis , i. e. break down of R. B. C. s RESULTS : - Serum bilirubin : > 2 mg % up to 5 mg %. - Unconjugated / free bilirubin in blood : > 80%. - Increased urobilinogen : in urine ; but no bilirubin present : in urine. - Increased stercobilinogen : in stool.

CAUSES : - Similar causes as of Hemolytic – anemia : e. g. - Malaria, - Snakebite, - Mismatched blood transfusion - Erythroblastosis - foetalis (Rh – Incompatibility) - Sickle cell anemia, - Spherocytosis - Some drugs (e. g. quinine, primaquine , dapsone, sulphanamides) - Physiological neonatal jaundice
 PHYSIOLOGICAL JAUNDICE (NEONATAL HEMOLYTIC JAUNDICE) nd rd 1. It occurs in newborn")
(2. ) PHYSIOLOGICAL JAUNDICE (NEONATAL HEMOLYTIC JAUNDICE) nd rd 1. It occurs in newborn babies -- on the 2 or the 3 day after birth and disappears before 10 days. 2. It is caused by rapid hemolysis --- leading to increased bilirubin production. 3. The condition is self limiting and requires no treatment. 4. Exposure of morning sunlight is preferred … The U. V. rays present in sunlight breaks excess of Bilirubin into Lumirubin , which is excreted through urine and Jaundice disappears.
 CRIGGLER - NAJJAR SYNDROME - A congenital disorder , - Due to")
(3. ) CRIGGLER - NAJJAR SYNDROME - A congenital disorder , - Due to deficiency, or, absence of : * Glucoronyl - transferase enzyme in Liver cells. - So, no conjugation of bilirubin takes place in liver cells. - So, free / unconjugated bilirubin is increased in liver cells. - This free bilirubin comes back in blood. - Hence , serum free bilirubin is increased.
 HEPATIC, OR, HEPATOCELLULAR - JAUNDICE Reason : Occurs due to destruction of")
(4. ) HEPATIC, OR, HEPATOCELLULAR - JAUNDICE Reason : Occurs due to destruction of liver cells. - So , conjugated bilirubin can’t be excreted out from liver , & come back in blood. Causes : Hepatitis : - Viral, - Alcoholic, - Toxic, - Drug induced . Liver cirrhosis Contd ….

Contd …. In blood : Serum bilirubin : > 5 mg% up to 15 mg % Most of bilirubin is conjugated : > 50% Liver function tests are altered : ( SGOT / SGPT in blood) In urine : No urobilinogen, or , very less. Bile - pigment (bilirubin) & bilesalts - present. So , mustard oil colour of urine. In stool : No stercobilinogen. So, white china clay colour of stool
 POST - HEPATIC, OR, OBSTRUCTIVE, OR, SURGICAL - JAUNDICE Reason : Occurs")
(5. ) POST - HEPATIC, OR, OBSTRUCTIVE, OR, SURGICAL - JAUNDICE Reason : Occurs , due to obstruction in biliary tract. - So, conjugated bilirubin in not excreted in intestine , & comes back in Liver, & then in blood. Causes : Gall stone, in common bile duct , Carcinoma head of pancreas.

In blood : Serum bilirubin : > 10 mg % up to 30 mg%. Mostly conjugated bilirubin Liver function tests : Normal , or , exaggerated. Serum Alkaline phosphates : increased In urine : No urobilinogen , Bile pigment (bilirubin) & bile salts : present. So, mutard oil colour of urine In stool : No stercobilinogen. So, white china clay colour of stool.

FEATURES OF JAUNDICE : • Skin , nails , & bulbar conjunctivae : Yellow. • Urine : Dark yellow , or, mustard oil - colour. • Stool : Dark yellow , or, China clay colour • General weakness , Nausea & Indigestion • Hepatomegaly --- In Hepatocellular - jaundice.
![[B. ] HEPATITIS * Cause : It is due to Inflammation & damage](http://slidetodoc.com/presentation_image_h/14dfb49a89ff717654fc94b6860ad903/image-18.jpg "[B. ] HEPATITIS * Cause : It is due to Inflammation & damage")
[B. ] HEPATITIS * Cause : It is due to Inflammation & damage of Liver cells. * Aetiological types : (A. ) Infective Hepatitis: e. g. (1. )Viral Hepatitis - A , B , C , D & E (2. ) Bacterial Hepatitis (3. ) Fungal Hepatitis (B. ) Non - Infective Hepatitis: e. g. (1. ) Alcoholic hepatitis (2. ) Toxic Hepatitis - by CCl 4 - poisoning , etc. (3. ) Drug - induced Hepatitis - e. g. by excess use of Paracetamol , Refampicin , INH , etc. Contd….

Contd … Features : - Nausea, vomiting, Anorexia ; - Fever , Pain in right hypochondnum ; - Hepotomegaly ; - Jaundice …. . Yellow skin , nails , bulbar conjunctivae ; - Urine : Dark mustard oil colour - Stool : China clay white colour TESTS : - Blood, urine & stool examination shows : Hepatocellular jaundice.
![[C. ] LIVER -CIRRHOSIS • - It is a complication of hepatitis. • -](http://slidetodoc.com/presentation_image_h/14dfb49a89ff717654fc94b6860ad903/image-20.jpg "[C. ] LIVER -CIRRHOSIS • - It is a complication of hepatitis. • -")
[C. ] LIVER -CIRRHOSIS • - It is a complication of hepatitis. • - Due to : * Inflammation & severe damage of liver - parenchyma , * Destruction of Liver cells & dysfunction of liver • - Initially hepatomegaly & then liver atrophy. • - May also result into : * Liver failure & hepatic - encephalopathy (hepatic coma )
![[D. ] LIVER FAILURE , OR , HEPTIC COMA , OR, HEPATIC ENCEPHALOPATHY -](http://slidetodoc.com/presentation_image_h/14dfb49a89ff717654fc94b6860ad903/image-21.jpg "[D. ] LIVER FAILURE , OR , HEPTIC COMA , OR, HEPATIC ENCEPHALOPATHY -")
[D. ] LIVER FAILURE , OR , HEPTIC COMA , OR, HEPATIC ENCEPHALOPATHY - Occurs as a complication of hepatitis, or, liver cirrhosis. - Extreme damage of liver cells. - Liver is not able : * to convert toxic ammonia into nontoxic - urea. - Increased ammonia concentration in blood. - Ammonia reaches to brain & damages it. - Brain functions are altered. - Patient also may go into coma state : Hepatic - coma.

3. PHYSIOLOGY OF GALL – BLADDER

PHYSIOLOGY OF GALL – BLADDER • It is a part of Hepatobiliary system. • Bile, secreted from liver --- is stored & concentrated in gall bladder. • It is a non - essential part for life.

FUNCTIONS OF GALL- BLADDER 1. Storage of bile, secreted from liver. 2. Concentration of bile : by absorbing water & electrolytes (except K+ & Ca ++ ) 3. Mucin secretion - acting as lubricant. 4. Evacuation of bile : by its contraction , when fats come in duodenum .
Neural Regulation : During Cephalic")
REGULATION OF G. B. CONTRACTION FOR BILE - EVACUATION (A)Neural Regulation : During Cephalic & Gastric phase of gastric secretion Vagal stimulation Release of acetylcholine Contraction of G. B. Evacuation of bile in intestine. (B) Hormonal Regulation : During Intestinal phase Chyme food rich in fats , entering intestine Secretion of C. C. K. (cholecystokinin) hormone , from intestine Contraction of G. B. Evacuation of bile in intestine.
 Gall – Stones : - Formed by : cholesterol,")
APPLIED OF GALL BLADDER (A) Gall – Stones : - Formed by : cholesterol, lecithin, bile pigments & calcium, in gall bladder - Stones in gall bladder -- termed as Cholelithiasis. - Stones in bile duct -- termed as Choledocholithiasis. Features : - Severe colicky / intermittent pain in right hypochondriam. - Nausea, Vomiting, indigestion. Diagnosis : - By Ultrasound scanning - By Cholangiography - By E. R. C. P. ( Endoscopic retrograde cholangio pancreatico graphy) Contd ….

Contd. . . Complications : 1. Cholecystitis 2. Obstructive jaundice Treatment - Surgery : 1. Cholecystectomy ( removal of gall bladder ). 2. Cholelithotomy ( removal of stone from gall - bladder) 3. Choledocholithotomy ( removal of stone from bile duct )
 CHOLECYSTITIS : CAUSE : 1. It is the Inflammation of gall")
(B. ) CHOLECYSTITIS : CAUSE : 1. It is the Inflammation of gall – bladder 2. It occurs usually, as a complication of gall – Stone FEATURES : Severe pain in right hypochondrium , i. e. Nausea, vomiting TREATMENT – Cholicystectomy , i. e. removal of gall – bladder.

IMPORTANT QUESTIONS 1. Jaundice : its definition , types, features and investigations. 2. Short notes on : a. Synthesis of bile pigment ( Fate of Hb) b. Physiological jaundice c. Hepatitis , Liver cirrhosis, Liver failire d. Functions of Gall bladder e. Gall stones.

THANK YOU
- Slides: 30