Physiology of Growth Growth Definition q A complex




: 1)")
 A slower progressive growth: from 3 to 12 years of age")



 Lymphoid type: § Grow rapidly in early childhood, and reach their")
 Reproductive type: - Gonads and accessory organs of reproduction remain undeveloped")
 Genetic factors. 2) Role of nutrition. 3) Season.")






, thyroid hormone, androgen, estrogens, glucocorticoids and")




 Ø A protein hormone bearing a structural")
 Ø Bound to two proteins in plasma.")





 v Chronic abuse")

- Slides: 34
Physiology of Growth
Growth • Definition: q A complex phenomenon characteristic of living organisms. q It involves: 1) An increase in: - Size, Length, and Weight Due to an increase in number and size of cells. 2) Maturational changes • e. g. differentiation of homogenous cells into cells with specialized functions e. g. bone marrow cells.
Growth q At the same time, cells in some parts of the body are dying and shed off e. g. mucosal cells of the G. I. T. tract and cells of the epidermis. q Some types of cells e. g. somatic cells and nerve cells, cease to divide after 5 -6 months of fetal life but they increase in size, and nerve cells ramify and grow myelin sheath in postnatal life.
Growth q In adult life, the capacity of repair after injury and growth is retained by some tissues and certain organs e. g. liver and healing of superficial wounds. q At middle and old age, some cells continue to: o Multiply e. g. nails and intestinal epithelial cells o Enlarge e. g. adipocytes and prostate o Decay e. g. teeth fall out, baldness, reproductive system atrophies after menopause in females q By the age of 65 -70, 20% of brain neurons are lost in both sexes.
Growth patterns Includes 4 phases, Two of which are growth spurts (rapid growth): 1) In infancy: continuation of fetal growth especially in the 1 st year [from 3. 5 to 10. 5 Kg] 2) Marked acceleration at the time of puberty: - In girls: between 12 -13 years of age - In boys: between 14 -15 years of age.
Growth patterns 3) A slower progressive growth: from 3 to 12 years of age 4) At 18 years of age in girls, and at 20 years of age in boys: small slow growth until 30 years of age. In girls: the increase in weight during adolescence is mainly increased fat formation. - In boys: it is due to increased muscular growth [Estrogens, androgens and growth hormone]
Growth patterns § After illness, there is a period of rapid growth in children (catch up growth). § The growth rate is 400% above normal until the previous growth curve is reached, and then growth slows to normal. § The cause is unknown.
Growth Curve § The general growth curve applies to the skeleton, muscles, thoracic and abdominal viscera. § Growth is episodic or salutatory
Growth Curve
Specialized types A) Lymphoid type: § Grow rapidly in early childhood, and reach their maximum at puberty. § After this, it degenerates. B) Neural type: § Rapid initial increase in size, so that the brain, the spinal cord and organs of special senses together with skull reach 90% of adult size at the age of 6 years. § No increase in number of neurons. § Increase in mass by elongation, ramification and myelination-rich in RNA synthesizes cytoplasm which runs in nerve fibers.
Specialized types C) Reproductive type: - Gonads and accessory organs of reproduction remain undeveloped till puberty when very rapid growth begins and continues throughout adolescence. D) Different type: - The adrenal gland, the uterus - Large at birth, then lose weight rapidly. Then, regain birth weight at adolescence.
Factors influencing growth and development 1) Genetic factors. 2) Role of nutrition. 3) Season. 4) Diseases. 5) Exercise. 6) Emotional disturbances. 7) Hormonal factors.
Genetic factors v Children of tall heavy parents are likely to have the same stature. v Identical twins have the same stature. v Racial differences. v The time of adolescence spurt is genetically determined by the hypothalamus.
Role of nutrition v The combined effects of a diet deficient in mass and energy, in proteins, in vitamins and minerals inhibit growth profoundly. And if the lack is sufficiently prolonged, the stunting of growth is irreversible. v Malabsorption leads to undernutrition, resulting in decrease growth. v Injury and illness lead to stunted growth because of excess protein catabolism. v Undernutrition affects muscle and fat more than bone. Teeth are affected more than bone.
Season v Growth in height is more in spring than in autumn. v Increase in weight is more in autumn than spring [hormonal]
Diseases v Congenital cardiac defects lead to hypoxia and finally to stunted growth if not treated before adolescence.
Exercise v Increase the mass of skeletal muscles. v This hypertrophy is favored by anabolic steroids.
Emotional disturbances v Can decrease the rate of growth inspite of taking an adequate diet.
Hormonal factors v Growth hormone, somatomedins (growth factors), thyroid hormone, androgen, estrogens, glucocorticoids and insulin.
Hormonal factors Ø In utero growth is independent of fetal growth hormone. It depends on IGF-II and thyroxine. Ø Growth hormone is elevated in newborns, but subsequently falls to adult levels. Spikes are larger at puberty (mean/24 hours is increased). Ø IGF-I (Somatomedin C) rises during childhood, reaching a peak between 13 -17 years of age. Ø IGF-II is constant throughout postnatal growth.
Hormonal factors ØSpurt of growth hormone at puberty is due to the anabolic effect of androgens (secretion of adrenal steroids), and also increases growth hormone responses to stimuli such as insulin and arginine. Ø They increase plasma IGF-I, only in presence of growth hormone. ØThey initially stimulate growth, and then terminate it by causing fusion of epiphysis Ø Also, estrogen causes fusion of epiphysis e. g. - precocious puberty is associated with stunted growth - Castration is associated with tall stature.
Hormonal factors Ø Thyroid hormone action is permissive to growth hormone, possibly via potentiation of somatomedins. It is needed for normal rate of secretion of growth hormone. ØThyroid hormones have effects on ossification of cartilage, growth of teeth, and contour of the face and the proportions of the body. ØCretins are dwarfs, mentally retarded and have infantile features. The reduction in growth is disproportionate. ØThe action of thyroid hormones is permissive to growth hormone.
Hormonal factors Ø Insulin causes growth when large amounts of carbohydrates and proteins are supplied with insulin (anabolic). ØGlucocorticoids are inhibitors of growth due to their direct catabolic action on cells.
Growth hormone Human growth hormone (h. GH) Ø A protein hormone bearing a structural resemblance to prolactin and human chorionic somatomammatropin hormone (h. CS). They are evolved from the same common single hormone. Ø Levels: basal levels in adult humans measured by RIA is normally less than 3 ng/ml.
Growth hormone Human growth hormone (h. GH) Ø Bound to two proteins in plasma. Ø One of them has a high affinity and is a fragment of growth hormone receptors. Its concentration is an index of the number of growth hormone receptors in the tissues. Ø The other protein is of low affinity. ØThe high affinity binding protein is present at low levels in African pygmies, and absent in Laron dwarfs. (0. 2 -1 mg/day in adults)
Somatomedins Ø Polypeptide growth factors, secreted by the liver, cartilage and other tissues in response to stimulation by growth hormone. Ø IGF-I (somatomedin C) and IGF-II. Ø IGF-I is stimulated by growth hormone and it has a pronounced growth stimulating activity. Ø Its concentration rises during childhood, peaks at puberty. Ø IGF-II is much less affected by growth hormone, and may play a role in growth of fetus before birth.
Mechanism of action of growth hormone Ø Growth hormone acts on cartilage to convert stem cells into cells that respond to IGF-I. Ø Then, locally produced IGF-I from cartilage cells and circulating IGF-I make the cartilage grow.
Dwarfism Can be due to: GHRH deficiency, GH deficiency or IGF-I deficiency. Laron dwarfism: § The plasma growth hormone concentration is normal or elevated but, there is end-organ unresponsiveness to growth hormone and consequently, a deficiency in circulating growth factors [decrease high affinity growth hormone binding protein, receptor deficiency, decrease IGF-I]
Dwarfism v African pygmies: have normal plasma growth hormone levels, and normal IGF-I & II levels before puberty. But, there is no increase in IGF-I during puberty, and no pubertal spurt. v Pygmies have also slight reduction in high affinity growth hormone binding protein.
Other causes of stunted growth v Cretinism causes stunted growth. v Precocious puberty (due to closure of epiphysis) v Gonadal dysgenesis: XO chromosomal pattern instead of XY or XX development (the gonads are rudimentary and external genitalia) v Many bone and metabolic diseases.
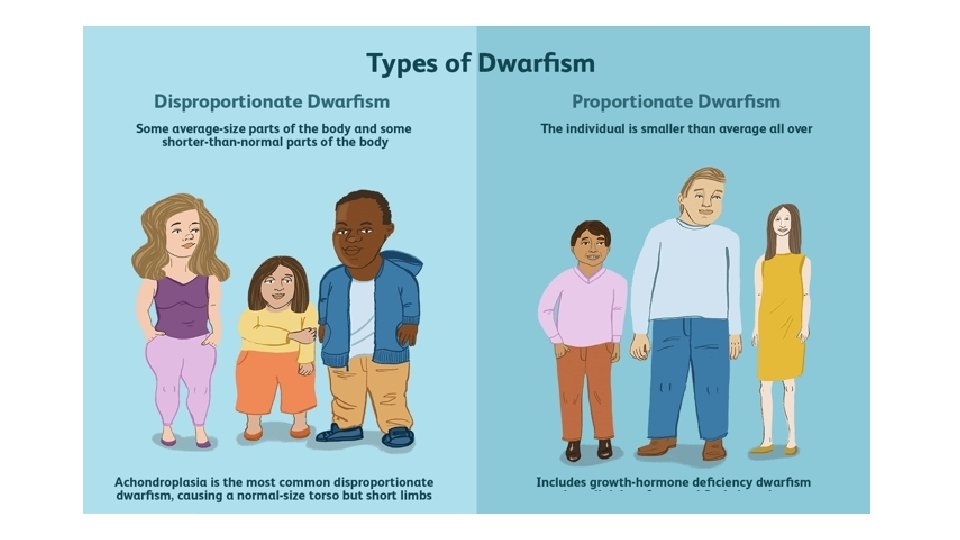
Other causes of stunted growth v Constitutional delayed growth (no cause) v Chronic abuse and neglect can cause dwarfism called psychosocial dwarfism or Kaspar Hauster syndrome (emotional). v Achondroplasia: normal trunk and short limbs. Occurs by a mutation in the gene for fibroblast growth factor receptor-3 (FGFR-3) in brain and cartilage.
Cretinism