Physiology of Cardiac Muscle and Electrical Activity of






 K Threshold Potential")







![Ionic influences �Effect of elevated [K+]ECF ◦ dilation and flaccidity of cardiac muscle at](https://slidetodoc.com/presentation_image_h2/321d5476e39725cd17c1f5bd7ccb4ebe/image-16.jpg "Ionic influences �Effect of elevated [K+]ECF ◦ dilation and flaccidity of cardiac muscle at")


 (- decreases) ◦ Anything that affects heart rate �Dromotropic ◦")
 plateau 0 Na in m.")











 Klw siklusnya")




 �recorded in mm �positive or negative or")








- Slides: 47
Physiology of Cardiac Muscle and Electrical Activity of the Heart Denny Agustiningsih
Denny Agustiningsih
Cardiac muscle Denny Agustiningsih
Two Types of Cardiac Muscle Cells �Ordinary: make up 95%- 99% of all heart muscle cells. �Also called worker cells or contractile cells �Biochemically similar to red skeletal muscle �Slow to fatigue �Specialized: make up remaining 1%-5% �Also called autorhythmic or automatic cells �Responsible for initiation and/or transportation of electrical impulses through the heart �pacemaker potential Denny Agustiningsih
CONDUCTION SYSTEM Sinoatrial Node Atrioventricular Node Denny Agustiningsih
Electrical Conduction �SA node - 75 bpm ◦ Sets the pace of the heartbeat �AV node - 50 bpm ◦ Delays the transmission of action potentials �Purkinje fibers - 30 bpm ◦ Can act as pacemakers under some conditions
Ca ++ in symphathetic 0 K+ out Membrane Potential (m. V) K Threshold Potential -40 -60 Ca (T-type) Na Spontaneous Depolarization parasymphathetic Time (msec) Denny Agustiningsih
Denny Agustiningsih
HEART RATE �Normally : 60 -100 bpm �> 100 bpm : tachycardia �< 60 bpm : bradycardia Denny Agustiningsih
�Resting heart rate is about 60 -100 beats/min (lower in athletes because they have large stroke volumes) �The HR can be increased about 3 times in exercise �Above about 200 beats/min the heart would not have time to fill properly therefore nature limits the rate �Rate is controlled by the autonomic nervous system Denny Agustiningsih
Extrinsic Influences �Autonomic nervous system �Hormonal influences �Ionic influences �Temperature influences Denny Agustiningsih
Control of Heart by ANS �Sympathetic innervation- ◦ + heart rate ◦ + strength of contraction ◦ + conduction velocity �Parasympathetic innervation ◦ - heart rate ◦ - strength of contraction ◦ - conduction velocity Denny Agustiningsih
• Autonomic nervous system modulates the frequency of depolarization of pacemaker • Sympathetic stimulation (neurotransmitter = NE on the SA nodal membranes ); binds to b 1 receptors • Parasympathetic stimulation (neurotransmitter = ACh ); binds to muscarinic receptors on nodal membranes; increases conductivity of K+ and decreases conductivity of Ca 2+ How do these neurotransmitters get these results?
Major Hormonal Influences �NE/E �Thyroid hormones ◦ + inotropic ◦ + chronotropic ◦ also causes an increase in CO by BMR �Estrogen/ Testosteron Denny Agustiningsih
Ionic influences �Effect of elevated [K+]ECF ◦ dilation and flaccidity of cardiac muscle at concentrations 2 -3 X normal (8 -12 meq/l) �Effect of elevated [Ca++] ECF ◦ spastic contraction Denny Agustiningsih
Effect of body temperature �Elevated body temperature ◦ HR increases about 10 beats for every degree F elevation in body temperature ◦ Contractile strength will increase temporarily but prolonged fever can decrease contractile strength due to exhaustion of metabolic systems �Decreased body temperature ◦ decreased HR and strength Denny Agustiningsih
Direct Stretch on SA node �Stretch on the SA node will increase Ca++ and/or Na+ permeability which will increase heart rate Denny Agustiningsih
Terminology �Chronotropic (+ increases) (- decreases) ◦ Anything that affects heart rate �Dromotropic ◦ Anything that affects conduction velocity �Inotropic ◦ Anything that affects strength of contraction �eg. Caffeine would be a + chronotropic agent (increases heart rate) Denny Agustiningsih
K out +20 K out ∞ Ca in (L-Type) plateau 0 Na in m. V Ca, -90 Denny Agustiningsih K
AP of Contractile Cardiac cells � Action potentials of cardiac contractile cells exhibit prolonged positive phase (plateau) accompanied by prolonged period of contraction ◦ Ensures adequate ejection time ◦ Plateau primarily due to activation of slow L-type Ca 2+ channels
Refractory period
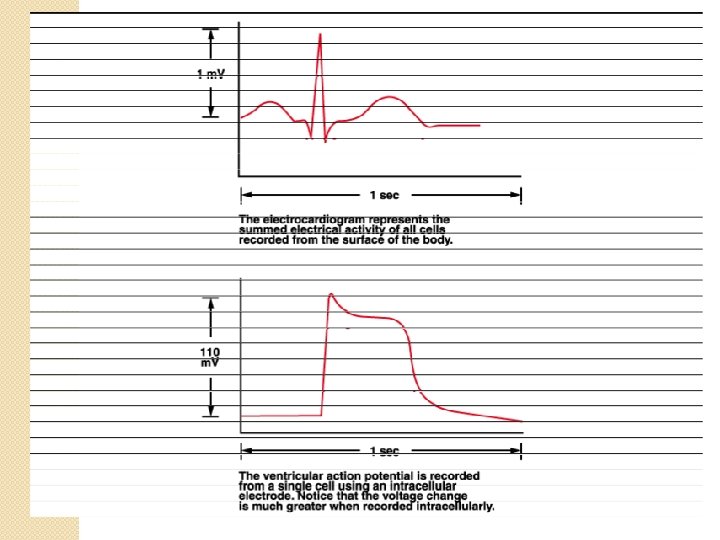
Action Potential Skeletal Cardiac
Mechanism of Cardiac Muscle Excitation, Contraction & Relaxation Denny Agustiningsih
Relative Refractory period 1 +20 2 m. V 0 -90 0 3 Period of Supranormal excitability Absolute Refractory period 4 0 100 200 300 Time (msec) Denny Agustiningsih 400
Denny Agustiningsih
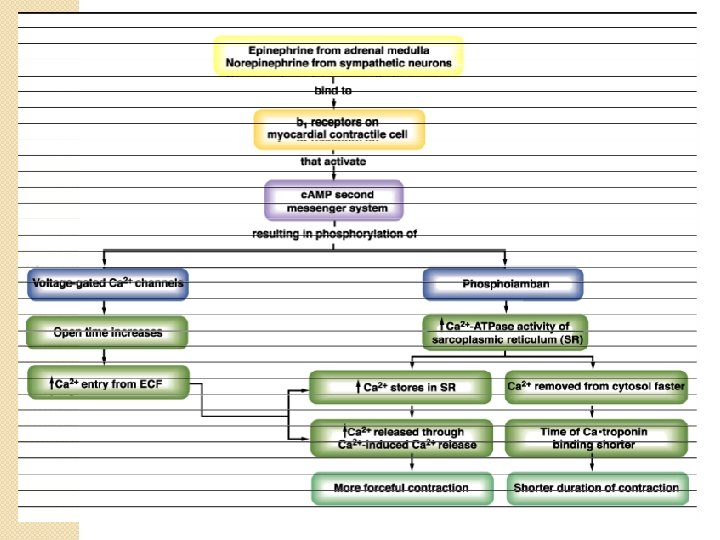
Modulation of Contraction Denny Agustiningsih
RECORDING Denny Agustiningsih
The Body as a Conductor This is a graphical representation of the geometry and electrical current flow in a model of the human thorax. The model was created from MRI images taken of an actual patient. Shown are segments of the body surface, the heart, and lungs. The colored loops represent the flow of electric current through the thorax for a single instant of time, computed from voltages recorded from the surface of the heart during open chest surgery.
The Modern ECG Machine
ECG examines how depolarization events occur in the heart • If a wavefront of depolarization travels towards the electrode attached to the + input terminal of the ECG amplifier and away from the electrode attached to the terminal, a positive deflection will result. • If the waveform travels away from the + terminal lead towards the terminal, a negative going deflection will be seen. • If the waveform is travelling in a direction perpendicular to the line joining the sites where the two leads are placed, no deflection or a biphasic deflection will be produced.
Serabut purkinje – ventrikel Nodus SA – atrium Atrium (ototnya lebih sedikit) Klw siklusnya atrium - atrial cyte Sirkulasi-peredaran darah Siklus-kontraksi dan relaksasi R T P Q S Denny Agustiningsih
R T P Q S Denny Agustiningsih
R 1 sec T P Q S 0. 5 Sec Denny Agustiningsih
ECG Complexes
Kontraksi – sistol Ventrike kaknan-memoma darah ke paru Ventrikel kiri-memompa darah keseluruh jantung Pintu masuk – katub yang menghubgungkan dengan atrium (valam atrioventricualr) Pintu keluar kiri - aorta Pintu keluar kanan – katub pulmuonal Tujuan awal kontraksi untuk membuka pintu keluar (aorta) ECG Complexes
ECG Description �ECG description ◦ amplitude (voltage) �recorded in mm �positive or negative or biphasic ◦ width (duration)
ECG in Perspective 1. ECG recording of electrical activity not the mechanical function 2. ECG does not depict abnormalities 3. ECG does not record all the heart’s electrical activity
Excitation-Contraction Coupling in Cardiac Contractile Cells � Ca 2+ entry through L-type channels in T tubules triggers larger release of Ca 2+ from sarcoplasmic reticulum ◦ Ca 2+ induced Ca 2+ release leads to cross-bridge cycling and contraction
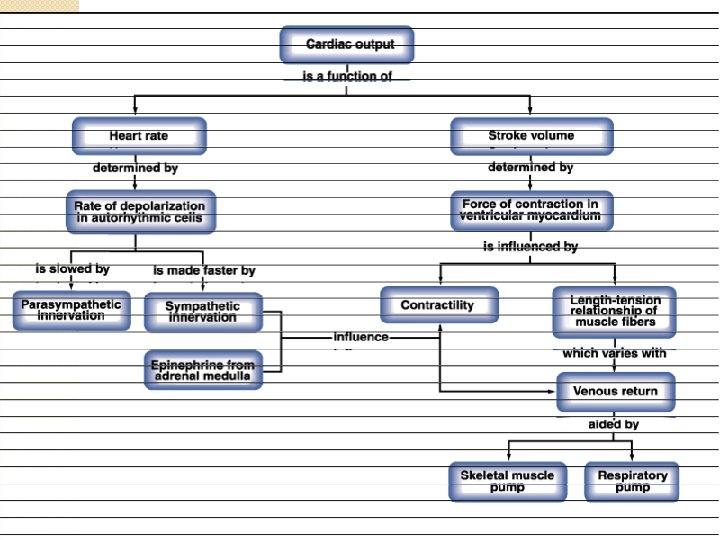
Frank-Starling Law � Preload, or degree of stretch, of cardiac muscle cells before they contract is the critical factor controlling stroke volume
Extrinsic Factors Influencing SV �Contractility is the increase in contractile strength, independent of stretch and EDV �Increase in contractility comes from ◦ ◦ Increased sympathetic stimuli Hormones - epinephrine and thyroxine Ca 2+ and some drugs Intra- and extracellular ion concentrations must be maintained for normal heart function
Modulation of Cardiac Contractions Figure 14 -30
Reflex Control of Heart Rate
Regulation of Cardiac Output Figure 18. 23
Depolarisasi mendahului kontraksi � Repolarisasi mendahului relaksasi � Kontraksi jantung tidak melalui otak � Listrik-otot atrium-kontraksi--ketika sampai di ventrikelventrike berkontraksi � Gap junction � Kontraksi otot jantung-otot pekerja � Otot pekerja memiliki aktin & myosin � Mendapat rangsang sehingga ion � Repolarisasi = fase istrahat � Kontraksi & relaksasi-aktin & myosin � Sebagian kalsium pergi ke aktin & myosin untuk berikatan dengan troponin C, sebagian ke retikulum sarkoplasma � Retikulum sarkoplasma-tempat penyimpanan ion calsium (ada pintu yang disebut. . , hanya terbuka untuk kalsium)masuk ke sitosol � Denny Agustiningsih