Physiology of Autonomic Nervous System Dr Ahmed AlSehli


 Autonomic N. S (involuntary) 1) Innervate skeletal muscles 1) Supply")






 Distributing center: Sympathetic Parasympathetic 1 : 32 1: 9 or 1:")
 CERVICAL DIVISION: Origin : It arises from lateral")
 SALIVARY GLANDS : a) Secretion of small amount of saliva, rich in organic")

 CARDIQ-PULMONARY DIVISION : Segments and end in 3 rd cervical and upper 4")

 Greater Splanchic Nerve : it supplies the abdomen e. g : (From T")
. The circulating catecholamin have")

 Lesser splanchnic nerve: From LI - L 3, relays in inferior mesentric ganglion")
 It is sympethetic supply of limbs, upper limbs")
. 2 - Skin")

 Oculomotor nerve ( III N ):")
 Contraction of")
 Fascial Nerve (VII N): It arises from superior salivary nucleus, relays in sphenopalatine")
 Vagus Nerve (XN): 75% of parasympathetic fibers of the body are the vagus")
 ON HEART * Inhibits all cardiac roperties, but")

 It is 82 , 3,")



 CHOLINERGIC (ac. Choline) I ) Cholinergic neurotransmission")


 Muscarinic receptors Sites : In cardiac muscles, smooth muscle and exocrine glands. Subtypes")

 Function of Nicotinic Receptors It has short timed receponse only exitatory : 1")
 OF AC CHOLINE. By choline-estrase enzyme 2 types. True - present in")
 Direct : on tissues")
 Reversible : short acting e. g Eserine")
 Persistent depolarization 2) Competitive inhibition as curare.")


. Dopa")

 α 1 : STIMULATORY a) V. C b) stimulation of sphincters.")

![RECEPTOR STIMULANTS α Receptors stimulated by : nor - adrenaline ]adrenaline} isoproterenol β Receptors](https://slidetodoc.com/presentation_image_h/ab65d0e0d7f1c33a673a5b9831a4bc61/image-50.jpg "RECEPTOR STIMULANTS α Receptors stimulated by : nor - adrenaline ]adrenaline} isoproterenol β Receptors")


 Mechanism Of Action: 1 - stimulate release of catecholamines")






 2 - Anhydrosis 3 -")
- Slides: 60
Physiology of Autonomic Nervous System Dr. Ahmed Al-Sehli
AUTONOMIC NRVOUS SYSTEM Definition : It is the system for involuntary subconscious functions , it controls the internal environment to maintain homeostasis. DIVISION OF NERVOUS SYSTEM : 1 - Central nervous system : a) Brain b) Spinal cord 2 - Peripheral nervous system : a) Cranial nerves Autonomic (involuntary) Somatic (voluntary) b) Spinal nerves Autonomic Somatic
Somatic N. S (voluntary) Autonomic N. S (involuntary) 1) Innervate skeletal muscles 1) Supply smooth muscles, Cardiac and Glands 2) One neurone between C. N. S and effector organ 2) Has 2 neurons connected by synapse between C. N. S & organ 3) Efferent arises from ventral horn cell. 3) Efferent preganglionic arises from lateral horn cells. 4) Chemical transmitter Acetyl choline 4) Either acetyl cholin or norepinephrine.
123 - A. N. S differs from Somatic N. S in : -In A. N. S there is : Autonomic ganglia Connector neurone is outside CNS It regulates smooth muscles Q: Discuss and differentiate the two divisions of A. N. S ?
A. N. S Sympathetic Parasympathetic 1 - ORIGIN: Thoraco-Lumber (Tl - T 12 , LI, 2, 3) Cranio - sacral 3, 7, 9, 10 S 2 , 3 , 4 1 - ORIGIN: Thoraco-Lumber Cranio - sacral (Tl - T 12 , LI, 2, 3) 3, 7, 9, 10, s 2, 3, 4, 2 -FUNCTION: Stress muscular exercise - Digestion and sleep, fear fight flight - Catabolic (energy lost from the body) 4 - DISTRIBUTION: widspread 5 - DISCHARGE : as one unit (most actions) at the same time ( Empting micturation defication - Anabolic (energy preserved) Localised To each system separetly
RELATIONSHIP BETWEEN SYMP ATHETC AND PARASYMPATHETIC 1 - RECIPROCAL : once sympathetic is stimulated, parasympaethetic is inhibited and vise - versa 2 - COMPLEMENTAL : e. g micturation and defication reflex. sympathetic for FILLING and parasympathetic for EVACUATION N. B both sympathetic and parasympathetic together help acurate control over an organ's activity.
AUTONOMIC GANGLIA DEFINITION : It is the site of physiological contact between pre and post ganglionic fibers. TYPES: a) lateral (sympathetic) b) collateral (mixed) or pure sympathetic c) terminal ( parasympathetic ) Lateral ( paravertebral) 23 ganglia: 3 = cervical sympathetic chain 12 = thoracic 4 = lumber 4 = sacral
Collateral: Around large. B. V as: - Caeliac ganglion - Superior mesentric ganglion - Inferior mesentric ganglion Terminal (in the wall of organ, no postganglionic as vagus or may be present very short post-ganglionic fiber
Pathway of pre-ganglionic sympathetic fibers: 1 - May synapse in first sympathetic chain ganglion, it enters. 2 - Synapsing in other sympathetic chain ganglia up or down. 3 - Synapse in collateral ganglia. 4 - Synapse in substance of adrenal medulla itself.
Function : 1) Distributing center: Sympathetic Parasympathetic 1 : 32 1: 9 or 1: 2 ? ? 2) Relay station between pre and post ganglionic fiber Localization : To diagnose site of relay, by Nicotine test: (Langlay's test) painting the ganglia with large doses of nicotine to block the site of relay, after that if it gives no post ganglionic response = relay Cervical Division of sympathetic
DESTRIBUTION OF SYMPATHETIC NERVOUS SYSTEM 1) CERVICAL DIVISION: Origin : It arises from lateral horn cell of Ti and T 2 and end in superior cervical ganglion I) EYE : a) dilatorpupilllary muscels = pupillary dilatation = Mydriasis b) Tarsal m. =elevation of eye lid = widening of eye superior inferior c) Muller's m. = Exophthalamos = Protrusion of eye ball in animals d) Blood vessels of eye = V. C e) relaxation of the ciliary muscle for vision
II) SALIVARY GLANDS : a) Secretion of small amount of saliva, rich in organic matters (enzymes) i. e viscus saliva. b) Squeezing around acinin of salivary glands push saliva outside III) SKIN : a) Erector pilae m = erection of hairs b) Vaso-conistriction of blood vessels = pallor c) Sweat : Secretion = mental sweat. IV) Cerebral blood vessels = vaso-conistriction
HORNER'S SYNDROME It Is Cerviacl Sympathectomy : characterized by : 1 -PTOSIS : drop of upper eyelid. 2 - MIOSIS : pupillary constriction. 3 - ANHYDROSIS : dryness of skin 4 -Emrophthalamos 5 - Flushing of the face ALL THESE EFFECTS ARE AT SAME SIDE OF LESHON
2) CARDIQ-PULMONARY DIVISION : Segments and end in 3 rd cervical and upper 4 thoracic ganglia I) HEART : increase all cardiac prosperities as: - positive inotropic effects = ↑ contractility - positive chronotropic effect = ↑ Heart rate. - = ↑ Conductivity - = ↑ Excitability II) CORONARY BLOOD VESSELS vasodilatation III) LUNG : a) bronco-dilatation. b) inhibits bronchial glands secretion of mucous IV) PULMONARY BLOOD VESSELS: vasoconstriction.
3 - SPLANCHIC DIVISION: To Abdomen and pelvis
A) Greater Splanchic Nerve : it supplies the abdomen e. g : (From T 5–T 9, relay in caeliac ganglion) a) wall of G. I. T → relaxation of its walls = retention ↓ motility. b) sphincters → its contraction e. g pyloric sphincter of stomach c) liver → glycogenolysis = glycogen converted to glucose. d) adrenal medulla → release of epinephrin and nor epinephrine. e) spleen → contraction & release of RBCs in case of heamorrhage f) adipose tissues → lipolysis. g) inhibite the intestinal juice secretion h) relaxation of gall bladder and contraction of its sphincter. N. B Stimulation of greater splanchic nerve causes two peaks rise in blood pressure : a) First rise due to V. C of visceral blood vessel b) Second peak due to release of catecholamin into blood.
ADRENAL MEDULLA: Supplied by pre-ganglionic sympathetic fibers (greater splanchnic nerve). The circulating catecholamin have same effects of direct sympathetic stimulation, but more prolonged , So body organs can be stimulated by 2 ways, Nervous (direct) & Hormonal (indirect), Also catecholamines can stimulate sites not supplied by direct sympathetic nerves.
N. B adrenal meddulla is modified by sympethetic ganglion because : 1 - No post-ganglionic fibers 2 - Causes release of 80% epinephrin. 20% nor epinephrin. N. B Selective secretion of adrenal medulla: a) More epinephrine in unexpected stresses as haemorrhaege b) More nor-epinephrine in familiar stresses as hypoxia
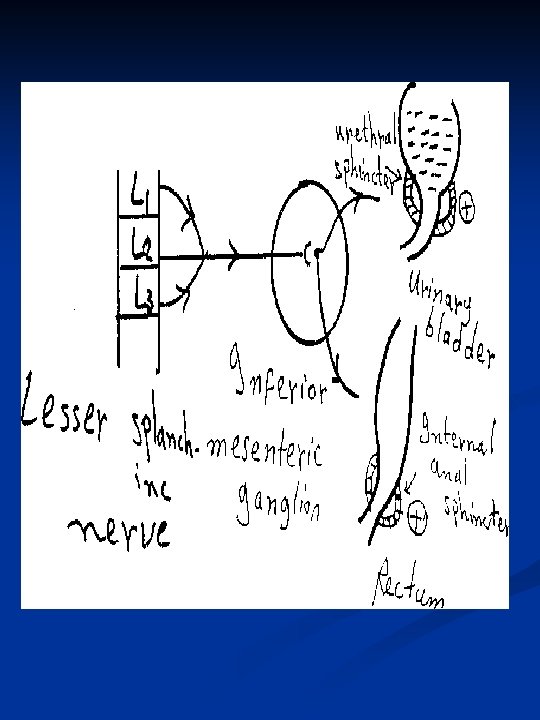
B) Lesser splanchnic nerve: From LI - L 3, relays in inferior mesentric ganglion It supplies the pelvis e. g-: a) Rectum → retention of stool (+) of internal anal sphincter b) Urinary bladder → retention of urine by relaxation of its wall and contraction of internal uretheral sphincter. c) Sex organs → ejaculation. External genitalia: In males : Inhibition of erection (v. c of erectile tissue) -Ejaculation of semen (contraction of vas deferens, prostate and ejaculatory duct) In females: Contraction or relaxation of female genital organ according to the stage of menstrual cycle and level of hormones in blood. N. B Small splanchnic nerve (from T 10 – T 12, relayes in caeliac and superior mesentric ganglion)
4 -SOMATIC DIVISION : (Orbelli phenomenon) It is sympethetic supply of limbs, upper limbs (T 4 - Ts) lower limbs (T 10 T 12), both relay in sympathetic chain = Sympethetic stimulation delays fatigue of muscle due to vasodilatation of skeletal blood vessels
ORGANS SUPPLIED BY SYMPATHETIC ONLY : 1 - Ventricles (vagal escape). 2 - Skin structures 3 - Skeletal B. V. 4 - Dilator pupillary muscles. 5 - Adrenal medulla
ORGANS SUPPLIED BY PARASYMPATHETIC 1 - Constrictor pupillary muscle. 2 - Oesophagus. 3 - Gastric glands. 4 - Erectile tissue. N. B Sympethetic → causes V. C of all blood vessels, except 1. Coronaries. 2. Skeletal blood vessels.
DISTRIBUTION OF PARASYMPATHETIC I- CRANIAL DIVISION : A) Oculomotor nerve ( III N ): It arises from occulomotor nucleus , relays in ciliary ganglion ble for near visions
During fixation of eyes to near object, III nerve causes : 1) Contraction of ciliary muscle → Increases convexity of the eye lens. 2) Contraction of medical rectus muscle → medial convergence of both eyes together. 3) Contraction of constrictor pupillae muscle → papillary constriction
B) Fascial Nerve (VII N): It arises from superior salivary nucleus, relays in sphenopalatine ganglion. FUNCTION : secretion of tears and saliva which is watery, poor in enzymes and big in amount. C) Glossopharyngeal Nerve (IX N): It arises from inferior salivary nucleus 9 relays in optic ganglion. FUNCTION : secretion of saliva
D) Vagus Nerve (XN): 75% of parasympathetic fibers of the body are the vagus nerve. It arises from dorsal nucleus, relays in terminal ganglia. FUNCTION : 1 - Inhibition (supression) of heart rate and contractility. 2 - Broncho-constriction and inhibition of inspirartory center and secretion of mucous from bronchial glands. 3 - Stimulation (excitation) of G. I. T motility and secretions.
EFFECT OF VAGUS NERVE 1 -) ON HEART * Inhibits all cardiac roperties, but it does not supply the ventricles (vagus escape). * Tonic (continuous) effect on the heart , which is more marked in athelets. * Coronary vaso-constriction (V. C ). 2) ON LUNGS: Mentioned before. 3) ON G. I. T: * Evacuation of food (stimulation of G. I. T. motility ). * Evacuation of gall bladder. * Stimulates secretion of: gastric juice , bile , pancreatic juice and mucus (Brunner's glands) * Increased hepatic blood flow. N. B Vagus nerve has no post-ganglionic fibers
WHY IT'S CALLED VAGUS ? Because it has : 1 - Afferent & efferent 2 - Stimulatory & inhibitory 3 - Widely distributed
II- SACRAL DIVISION OF PARAS YMPATHETIC ( nerve erigentis) It is 82 , 3, 4 and called pelvic nerve and relays in hypogastric ganglia. FUNCTION : 1 - It supplies urinary bladder → causes micturation 2 - distal 2/3 of large intestine and rectum → causes defecation 3 - Male and female sex organs → erection by vasodilatation of blood vessels of penis (♂) or clitoris (♀)
MICTURATION: Pelvic nerve causes contraction of wall of urinary bladder and relaxation of internal uretheral sphincter → passage of urine
DEFECATION : pelvic nerve causes contraction of wall of rectum and relaxation of internal anal sphincter → passage of stool N. B External uretheral or anal sphincters are not under autonomic control but under somatic control via pudendal nerve. N. B Internal sphincter is more important than external sphincter because it is smooth muscle i. e fatigue resistant, while external sphincter is skeletal muscle i. e fatigable.
CHEMICAL TRANSMITTERS DEFINITION : it is the substance which transmits the nerve impulse from pre - synaptic to post - synaptic membrane. MECHANISM : Arrival of nerve impulse to Pre-synaptic membrane → causes Ca+ uptake by acetyl choline vesicles → causes swelling and rupture of vesicles → causes release of acetyle choline which can cross the synaptic cleft → formation of acetylcholin - receptor complex → Increase Na permeability → Depolarisation Action potential This Causes Propagation of Nerve Impulse
TYPES OF NERVE ENDINGS ADRENERGIC (nor adrenaline) CHOLINERGIC (ac. Choline) I ) Cholinergic neurotransmission : - ( six steps ) 1 - Synthesis of acetyl choline : -( In cytoplasm) choline + acetyl Co. A CAT Ach + Co. A. ( choline - acetyl - transferase) 2 - Storage of acetyl choline in vesicles In the synaptic vesicles. 3 - Release of Acetyl choline : Ca++ channels in the presynaptic membrane opens → Ac. ch. Release by exocytosis 4 - Binding to receptors. 5 - Degradation of Ac. choline Ac. ch. choline + acetate esterase 6 - Recycling of choline Into the neurone for resynthesis of Ac. ch.
SITES OF RELEASE OF ACETYL CHOLINE 1 - Autonomic ganglia (i. e all preganglionic fibers) 2 - All parasympathetic post ganglionic fibers. 3 - Some sympathetic post gangljpnic as sweet glands and blood vessels of skeletal muscles. 4 - M. E. P = motor end plate (i. e neuro - muscular junction) 5 - Adrenal medulla (pre ganglionic ) 6 - C. N. S.
TYPES OF CHQLINERGIC RECEPTORS MUSCARINIC NICOTINIC 1 -This name from muscarine, a substance which has a same action as ac. choline in these sites: 1 - Name from nicotine which in small dose has the same action of ac. choline in a) M. E. P B) autonomic ganglia c) adrenal medulla d) C. N. S a) parasympathetic b) sympathetic post (ganglionic 2 - Blocked by atropine by comopetitive Inhibition, not blocked by cholinestrase, so they have longer duration of action than ac. choline 2 -Blocked by large dose of nicotine (autonomic)or by curare ( in MEP )
A) Muscarinic receptors Sites : In cardiac muscles, smooth muscle and exocrine glands. Subtypes : Ml , M 2 , M 3 and M 4. -Some sympathetic post-ganglionic as sweet glands and blood vessels of skeletal muscles. - M. E. P = motor end plate (i. e neuro muscular junction) - Adrenal medulla (pre ganglionic ) - C. N. S. Ml : in autonomic ganglia, CNS and gastric mucosa M 2 : in cardiac cells and smooth muscles. M 3 : in smooth muscles and secretory glands. M 4 and M 5 : unknown sites.
Functions of muscarinic receptors It has prolonged reseponse, lasts for seconds, either exitation or inhibition : 1 - Cardiac inhibition ( slow heart rate. ) 2 - Broncho-constriction. 3 - Salivary secretion 4 - Increases G. I. T secretion and motility. 5 - Pupillary constriction. 6 - Contraction of ciliary muscle. 7 - Contraction of urinary bladder and rectum.
B) Function of Nicotinic Receptors It has short timed receponse only exitatory : 1 - Help ganglion transmission. 2 - Secretion of epinephrine and nor-epinephrine from Ad. Medulla. 3 - Stimulates N. M. J (MEP) to produce skeletal muscle contraction
FATE (REMOVAL) OF AC CHOLINE. By choline-estrase enzyme 2 types. True - present in nerve –endings specific only for Ac - highly potent (strong) pseudo (false) - present in plasma. - non specific, can act on any ester - less potent.
PARASYMPATHOMI M ETIC DRUGS Acts By Two Ways : A) Direct : on tissues as muscarine, nicotine in small dose and carbachol. B) Indirect : anticholinesterases as DFP and Eserine (war gas)
Anti cholinesterases : Two types : a) Reversible : short acting e. g Eserine : generalized i. e. ↑ both muscarinic and nicotinic actions. Prostigmine: Nicotinic i. e ↑ skeletal muscles MEP activity = used in treatment of myasthenia gravis. b) Irreversible : long acting drugs i. e toxic, called nerve gases, or insecticides as DFP which causes paralysis of motor functions → difficulty in breathing → death
PARASYMATHOLYTIC DRUGS Mechanism of action : 1) Persistent depolarization 2) Competitive inhibition as curare. Types : A) ganglion blockers -Nicotine in large doses - Hexamethonium They cause paralysis of autonomic ganglia by persistant depolarization. B) post - ganglionic blockers -Atropine C) MEP blockers - Curare - Botulinum - Flexidil - Succinyl cholin. ( persistent depolarization)
Curare : - acts by competitive inhibition to Ac. ch. It can be used together with succinyl choline as muscle relaxants ATROPINE (anti-muscarinic drug ): ACTION : a) ON THE EYES : - Mydriasis and cycloplegia(loss of ability for near vision) b) ON SALIVARY GLANDS : - Dryness of mouth c) ON G. I. T : - Decrease motility = antispasmodic d) ON RESPIRATION : - Block secretions in respiratory tract e) ON C. V. S : - Tachycardia = ↑ heart rate. f) ON URINARY TRACT : - ↓ motility of urinary bladder.
Effect of injection of Ac. ch. after Atropine on A. B. P Nicotinic receptors in adrenal medulla unblocked rise in A. B. P CLINICAL USES OF ATROPINE 1 - Fundus examination → Mydriasis 2 - Bronchial asthma → Bronchodilatation. 3 - Treatment of colic →↓ motility of G. I. T. 4 - pre anaethetic drugs to prevent cardiac arrest. 5 - Befor surgery → to block respiratory secretions
ADRENERGIC TRANSMISSION 5 STEPS : Hydroxylase enz. 1 - Tyrosine DOPA (In cytoplasm). Dopa dopamine. 2 - Storage of nor epinephrine in vesicles : OH Dopamine N. B Nor. epinephrine ( In synaptic vesicles. ) In adrenal medulla only: CH 3 Nor - epinephrine. 3 - Release of nor-epinephrine : - Into the synapse. 4 - Binding by receptors : either post-synaptic ( on the effector organ) or pre- synaptic receptors ( on nerve endings. ) 5 - Removal of nor- epinephrine ( Fate ).
SITES OF RELEASE OF CATECHOLAMINES 1 - Adrenergic endings : - only nor - adrenaline. 2 - Adrenal medulla : causes release of : 80% epinephrine 20% nor-epinephrine FATE OF CATECHOLAMINES 1 - Active reuptake = 80 -90% back into ad. vesicles. (Na-k Atpase sys. ) 2 - Destruction = 7 % by MAO (oxidation) COMT (methylation) 3 - Excretion as such = 3 %
ADRENERGIC RECEPTORS (ALQUISTE) α 1 : STIMULATORY a) V. C b) stimulation of sphincters. α 2 : - INHIBITORY 0 a) relaxation of walls of G. I. T b) pre - synaptic inhibition of release of nor epinephrine (-ve feedback) βl : - STIMULATORY (+) a) heart +ve increase H. R & contraction b) adipose tissue = lipolysis c) renin - angiotensin. system = ↑ ABP. β 2 : -INHIBITORYO (–) relaxation of smooth muscles 1 - bronchi = bronchodilatation. 2 - blood vessels = V. D in skeletal blood vessels & coronaries. in :
N. B β 1 receptors are stimulated equally by epinephrine and nor-epinephrine B 2 receptors stimulated more by epinephrine than N. E β 2 adrcnoreceptors : tow groups α 1 & α 2: αl receptors have high affinity for phenyl-ephrine present on post. synaptic membrane of effector organ. α 2 receptors have high affinity for clonidine. present on Pre-synaptic nerve endings to control release of norepinephrine (causes its inhibition). N. B β 2 pre-synaptic receptors stimulate NE release, both a 2 and β 2 receptors are called pre - synoptic receptors.
RECEPTOR STIMULANTS α Receptors stimulated by : nor - adrenaline ]adrenaline} isoproterenol β Receptors stimulated by : isoproterenol J. adrenalin]- nor - adrenaline N. B nor - adrenaline, has a more pressor effect because it acts mainly on α due to receptor sensitivity. RECEPTOR BLOCKERS : α β Blockers : ergot alkaloids. Blockers : inderal. (Propranolol. ) N. B In G. I. T inhibition of the wall is by α 2 and may be β 2 receptors. While stimulation of sphincters only by al receptors (not β 1 ). N. B α is stimulatory except on G. I. T, it is inhibitory While β is inhibitory except on heart, it is stimulatory.
COMPARISON BETWEEN α & β RECEPTORS α – RECEPTOR 1 - papillary dilatation 2 - vasoconstriction 3 - intestinal relaxation 4 - contraction of G. I. T sphincters 5 - pilomotor contraction 6 - contraction of spleen capsule 7 - inhibition of insulin secretion 8 - contraction of internal uretheral sphincter 9 - salivary secretion 10 - ejaculation stimulated by : N. E , epinephrine and phenyl -ephrine Blocked by: Ergot alkaloids β - RECEPTOR 1 - far vision (ciliary muscle relaxation) 2 - vasodilatation 3 - intestinal relaxation 4 - gastric wall relaxation 5 - increase heart rate 6 - increase heart contractility 7 - stimulation of insulin secretion 8 - Broncho-dilatation. 9 - glycogenolysis. 10 - Liplysis 11 - Renin secretion. stimulated by: Isoproterenol, adrenaline , N. adrenalin Blocked by : Propranolol.
MECHANISM OF ACTION OF ADRENERGIC RECEPTORS αl Increases intra-cellular C-AMP. α 2 Inhibit adenyl cyclase enzyme, so it decreases cyclic AMP so interfering between the combination between the transmitter and its receptor βl receptors stimulates adenyl cyclase , increases cyclic AMP β 2 receptors → unknown mechanism but may also act by increasing C-AMP
Sympathomimetic drugs (adrenergic Agonists ) Mechanism Of Action: 1 - stimulate release of catecholamines e. g Tyramine ↓ (indirect acting agonist ) 2 - inhibit reuptake e. g Cocaine 3 - α stimulants Direct acting agonist 4 - β stimulants
SYMPATHOLYTIC DRUGS 1 - Inhibit synthesis and storage e. g reserpine. 2 - Inhibit release of catecholamines e. g guanithidine. 3 - Recepor blockers a & B receptors 4 - False transmiters e. g a methyl dopa( aldomet ). 5 - Ganglion blockers e. g hexamethonium and arfonad
DIFFERENCE BETWEEN EPINEPHRIN 1 - sites of release 2 - receptor sensetivity 3 - on heart 4 - pressor effect (peripheral resistance) 5 - metabolic 6 - systolic pressure 7 - diastolic pressure 8 - G. I. T motility NOR EPINEPHRE - adrenal medulla & - α and β equal adrenergic nerve - increase cardiac ending output and heart - mainly a & β rate slightly - decrease both - increase -glycogenolysis, - no effect lipolysis - little effect - increase - decrease
PHEOCHROMOCYTOMA Tumour of adrenal medulla resulting in attacks of hypertension in emergency states, discharge of sympathetic leading to: 1 - increased arterial pressure 2 - increased blood flow to active muscles 3 - increased blood glucose level 4 - increased rate of blood coagulation. 5 - increased mental activity 6 - increased glycogenolysis in liver and muscles. 7 - increased rate of cellular metabolism.
Control of A. N. S by Higher centers 1 - Some autonomic reflexes as micturation, defecation and erection are under inhibitory control of centers in C. N. S. 2 - Cardio-vascular, respiratory and digestive activity are under control of medulla within the brain stem. 3 - Stimulation of anterior nucleus of hypothalamus is accompanied by parasympathetic effects, while stimulation of posterior nucleus is accompanied by sympathetic effects.
1 - Cardiovascular autonomic reflexes : High arterial pressure → baro-receptors → pressure fall back toward normal. 2 - Gastrointestinal autonomic reflexes : a) Un-conditioned reflex e. g. presence of food in mouth causing salivary secretion. b) Defecation reflex. c) Micturation reflex. d) Sexual reflexes : Erection (parasympathetic function, followed by ejaculation (sympathetic function) N. B biofeedback research demonstrate that the A. N. S is not autonomic, it can be voluntary.
DISORDERS OF AUTONOMIC FUNCTIONS SYMPATHETIC QVERACTIVITY: 1 - HYPERTENSION : sympathetic increases peripheral resistance 2 - ANGINA PECTORIS : sympathetic increases myocardial O 2 3 - Hyperthyroidism: Thyroid hormone increases sensitivity or number of adrenergic receptors
GENERALISED AUTONOMIC INSUFFICIENCY 1 - Male impotence (no erection) 2 - Anhydrosis 3 - Orthostatic hypotention. 3 - No pupillary control 4 - Urinary retention. N. B all these may accompany diabetes mellitus THE ENTERIC SYSTEM: Neural plexuses within walls of the oesophagus , stomach small intestine and colon , Functioning independent of A. N. S so sympathetic and parasympathetic innervation alters the intrinsic activity of the enteric neural network.