Physiology BIO 240 Lecture No 12 Renal Nephron

Physiology BIO 240 Lecture No. 12 Renal –Nephron, Filtration, Reabsorption, Secretion, Renal Compensatory Mechanisms Fall 2013 Dr. Ana M Jimenez

Thinking About Body Fluid – How much water does my body have? – What happens to my blood pressure if I have to much water? – What happens to my blood pressure if I urinate too much fluid? – What happens to my blood pressure if I eat too much salt?

How much Water is there in the Human Body?

Body Fluid • Fluid in body – 60% of body weight – Intracellular fluid (ICF) – 40% of body weight, – Extracellular fluid (ECF) – 20% of body weight, • Interstitial fluid (IF) – 15% of body weight, • Blood plasma (BP)– 5% of body weight, • If your weight is 70 Kg, your fluid is: – ICF = 70 Kg X 0. 40 = 28 Liters, – ECF = 70 Kg X 0. 20 = 14 Liters, • IF = 70 Kg X 0. 15 = 10. 5 Liters, • BP = 70 Kg X 0. 05 = 3. 5 Liters. • Fluid in BP – determines blood pressure!
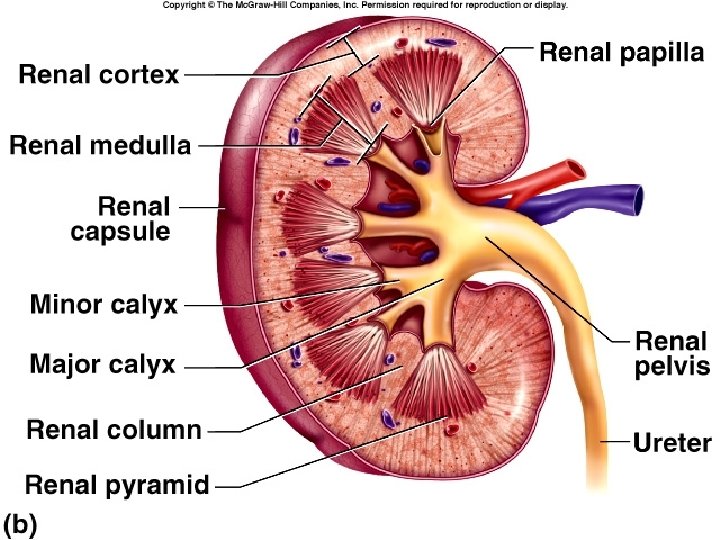

• Functional unit of the kidney, • Made of: Nephron – Renal Corpuscle – Proximal Convoluted tubule – Loop of Henle – Distal Convoluted tubule – Collecting duct Renal Cortex – is isosmolar to blood 300 m. Osm/L Renal Medulla – is hyperosmolar to blood can range from 600 m. Osm/L – 1400 m. Osm/L (depends on ADH levels)

Substance Movement Renal Corpuscle Blood Filtration Proximal Tubule Reabsorption Distal Tubule Secretion Loop of Henle Filtrate fluid and substances inside the nephron’s lumen Fox, Fig 17 -25, pg 572 Urine Fluid and substances excreted out of body

Renal Corpuscle blood plasma is filtered through the glomerulus-capsule membrane, the fluid that moves into the Bowman’s space is called filtrate. Visceral Wall Parietal Wall Fig 17 -8, pg 556

Cross-section through glomerular capillary. What membrane does fluid and small solutes have to cross to enter Bowman’s space? Glomerular-Capsule membrane

Filtration • First step in blood processing, occurs in the renal corpuscles: • Water and solutes filter into bowman’s capsule, through glomerular-capsular membrane. – Occurs due to existence of a pressure gradient. – Glomerular capillary filtration occurs rapidly due to the increased number of fenestrations (holes), • Glomerular hydrostatic pressure and filtration are directly related to systemic blood pressure: ↑blood pressure ↑hydrostatic pressure ↑filtration
 • Glomerular Hydrostatic Pressure (GHP) determined by")
Factors that determine Glomerular Filtration Rate (GFR) • Glomerular Hydrostatic Pressure (GHP) determined by amount of fluid in cardiovascular system – affected by changes in blood pressure - increased GHP increases filtration fluid in urine • Glomerular Oncotic Pressure (GOP) determined by amount of albumin (protein) in blood plasma – affected by changes in [albumin] – increased GOP decreases filtration less fluid in urine • Bowman’s Hydrostatic Pressure (BHP) determined by amount of fluid in Bowman’s Space – affected by changes in blood pressure – increased BHP decreases filtration less fluid in urine

Peritubular capillaries Efferent arteriole Distal tubule S R Glomerulus F Afferent arteriole R S Bowman’s capsule Proximal tubule R S R KEY F = Filtration: blood to lumen R = Reabsorption: lumen to blood S = Secretion: blood to lumen E = Excretion: lumen to external environment Conztanzo, Fig 19 -2, pg 619 R Loop of Henle To renal vein Collecting duct E To bladder and external environment Note direction of substance movement in/out of blood for each process.

What happens if there is fluid imbalance? Emma wants to know! – Too much fluid in BP? – Too little fluid in BP? – Too much fluid in IF? – Too little fluid in IF? – Too much fluid in cells (ICF)? – Too little Fluid in cells (ICF)?

Proximal Convoluted Tubule • First part of renal tubule nearest to Bowman’s capsule, • Follows a winding, convoluted course, • Reabsorption: movement of molecules OUT of the tubule and INTO blood, – Called reabsorption because it goes back to blood, – Primarily water, electrolytes and glucose are reabsorbed through secondary active transport dependent on Na+ gradient set-up by Na+/K+ATPase pump.

Reabsorption of MOST substances takes place in the Proximal Tubule

Renal Cortex ~ 300 m. Osm Isotonic to blood Figure 23. 6 Renal Medulla ranges from ~300 - 1400 m. Osm hypertonic to blood

Loop of Henle • Water conservation process – Counter-current mechanism filtrate concentration • Separates reabsorption of water and solutes, • Descending loop – Permeable to water, but NOT to salts Na. Cl, – initial segment (300 m. Osm/L), close to ECF renal cortex • Ascending loop – Permeable to Na. Cl, but NOT water, – Last segment hypotonic (100 m. Osm/L) to ECF

Cortex Osmorlity ~300 m. Osm Medulla Osmolarity Increases from 300 m. Osm – 1400 m. Osm Ascending limb permeable to salt but not water Descending limb permeable to water but not salts The renal counter-current multiplier system establishes the osmotic gradient required for the formation of hyperosmotic urine. Figure 14 -17

Figure 23. 19 Water is conserved to compensate for dehydration or hypotension, water is excreted to compensate for hypertension

Reabsorption by DT and CD • • • Function in water conservation, solute and p. H balance A small amount of solute reabsorption, Not usually permeable to water, Water and Na+ permeability highly regulated hormones Principal cells have receptors for the hormones: – Aldosterone functions in Na+ reabsorption, – Antidiuretic hormone (ADH) functions in water reabsorption – Natriuretic peptides function in decreasing Na+ reabsorption • Intercalated cells – Function in p. H balance – in acidosis secrete H+ in alkalosis conserve H+.

Tubular Secretion • Substances are secreted from blood to filtrate • Distal Tubule – most secretion by mass – Primarily K+ to maintain [K+] in blood normal, – Also H+ dependent on p. H of blood • Proximal tubule – small amount – Cellular transporters – transport blood hormones, metabolites, medications, toxins, etc – Cellular transporters can be saturated by [substance] in blood, – Medication renal clearance (getting rid from blood) is dependent on rate of secretion

Overview of absorption from nephron to blood and secretion from blood to nephron of different substances Urea is only reabsorbed from collecting duct in the presence of ADH
 is in solution")
Ammonia Fig. 23. 2 is a gas Ammonium ion (NH 4+) is in solution 23

Why does someone with hypertension have to restrict salt intake? Emma wants to know! – All salts? – What is the difference between Na. Cl & KCl? – How does a diuretic decrease blood pressure? – Why does someone with untreated diabetes mellitus excrete so much urine?
")
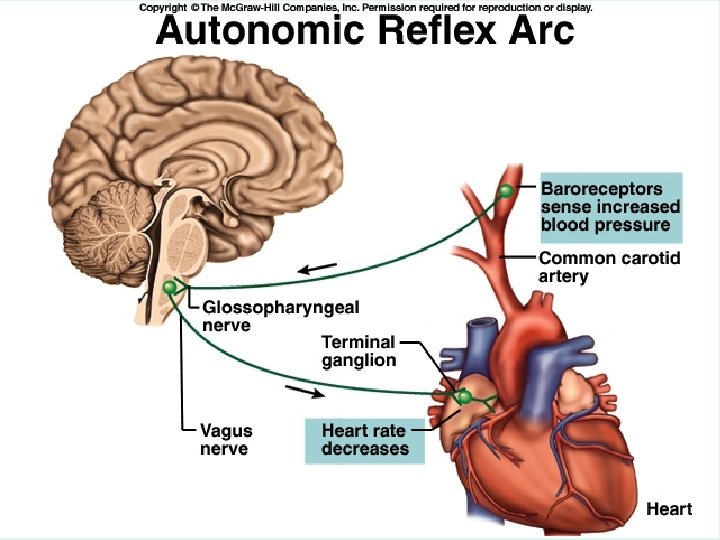
Compensation for Changes in Blood Pressure • Neural Reflex - first to respond (milliseconds) – Involves detection of blood pressure and activation of the baroreceptor reflex – Compensation for hypertension – decreased heart rate, – Compensation for hypotension – increased heart rate and strength of ventricular systole. • Neural Hormonal Reflex – responds within 24 hours – Involves detection of blood pressure changes by • detecting amount of fluid in blood plasma • concentration of Na+ in blood plasma and/or cerebrospinal fluid – Compensation for hypertension – diuresis (↑urine volume) – Compensation for hypotension – water conservation

Cardiac Control Brainstem – Neural Reflex • Negative feedback loop – functions within seconds and coordinates autonomic stimulation by activating: – Sympathetic: to heart (cardiac plexus) and to medulla oblongata to increase respiratory rhythm compensates for hypotension or hypercapnia or hypoxia. – Parasympathetic: to heart (CN 10, Vagus) and to medulla oblongata to decrease respiratory rhythm to compensate for hypertension or hypocapnia.

Baroreflex • Baroreceptors in carotid arteries and aorta, – stretch receptors - detect increased arterial diameter during hypertension, – Detect changes in blood pressure (baro=pressure), • Most sensitive to hypertension than hypotension, • Afferent neuron (glosophryngeal nerve, CN IX) – Sends information to nuclei in pons and medulla, • Integrator – pons and medulla (CNS) • Efferent neuron (CN X - parasympathetic), • Effector - postganglionic neuron releases ACh to decrease heart rate.

Hormonal Reflex - Regulation of Urine Volume Compensates for Changes in Blood Pressure • Functions through hormones, takes ~24 hours: • Compensation for Hypertension – Atrial natriuretric hormone (ANH) - secreted by specialized cardiac atrial and ventricular muscle fibers, • Promotes ↑[Na+] in urine ↑H 2 O in urine ↑urine volume ↑H 2 O loss, (opposes Aldosterone). • Secreted in response to ↑blood pressure or ↑blood volume. • Compensation for Hypotension – ADH secreted by hypothalamus influences water reabsorption: • ↑H 2 O reabsorption ↓urine volume preventing water loss. – Aldosterone: activated by the RAAS (renin-angiotensinaldosterone system) mechanism • ↑Na+ reabsorption in distal tubule ↑[Na+] in blood ↑ H 2 O reabsorption into blood.
 Inhibitors - prescribed for hypertension")
RAAS Renin Angiotensin Aldosterone Angiotensin-converting enzyme (ACE) Inhibitors - prescribed for hypertension

What happens to me when Emma wants to I drink alcohol and eat know! salty chips? – Initial edema, – Compensatory mechanisms kick-in, – Increase urination, – Increased thirst, – Ethanol decreases ADH, what does that do to urine volume? – Is alcohol a diuretic?
- Slides: 31