Physiological Changes During Pregnancy The normal adaptations that







 15")






 +50% (4. 5 vs 3")


 Dietary craving:")

 Bladder tone Bladder capacity Residual volume")
: tingling to frank pain caused by")
 Linea alba——linea nigra")


















 What happens to these special structures after birth? - Umbilical arteries atrophy")







- Slides: 51
Physiological Changes During Pregnancy
The normal adaptations that a woman undergoes during pregnancy to better accommodate the embryo or fetus. They are physiological changes, that is, they are entirely normal, and include A. cardiovascular B. hematologic C. metabolic D. renal E. respiratory
To provide a suitable environment for the nutrition growth and development of the fetus and to prepare the mother for the process of parturition and subsequent support for the newborn infant
Hormonal changes Estrogen is mainly produced by the placenta and is associated with fetal well–being. Women also experience increased human chorionic gonadotropin (β-h. CG); which is produced by the placenta. This maintains progesterone production by the corpus luteum. The increased progesterone production, first by corpus luteum and later by the placenta, functions to relax smooth muscle. Elevated progesterone levels also contribute to an increase in minute ventilation to 50% greater than nonpregnant levels.
Hormonal changes Prolactin levels increase due to maternal pituitary gland enlargement by 50%. This mediates a change in the structure of the mammary gland from ductal to lobular-alveolar. Parathyroid hormone is increased which leads to increases of calcium uptake in the gut and reabsorption by the kidney. Adrenal hormones such as cortisol and aldosterone also increase. Human placental lactogen (h. PL) is produced by the placenta and stimulates lipolysis and fatty acid metabolism by the woman, conserving blood glucose for use by the fetus. It can also decrease maternal tissue sensitivity to insulin, resulting in gestational diabetes.
Hormonal changes
Hormonal changes Thyroid enlargment High level T 3, T 4 Normal TSH Subclinical hypothyrodism
Cardiovascular changes Position and size of heart ECG changes Increased heart rate (+15%) 15 -degree left axis deviation Inverted T-waves in lead III Q in lead III and AVF Unspecific ST changes
Cardiovascular changes Appear larger
Cardiovascular changes § Heart rhythms and murmurs: soft , transient Caution: How to interpret these murmurs § Inferior vena cava syndrome: In the supine position, the inferior vena cava is compressed by the enlarged uterus, resulting in decreased cardiac output. Some women may have symptoms that include dizziness, light-headedness, and syncope.
Cardiovascular changes blood volume slowly increases by 40 -50%. The increase is mainly due to an increase in plasma volume through increased aldosterone. It results in an increase in heart rate (15 beats/min more than usual), stroke volume, and cardiac output. Cardiac output increases by about 50%, mostly during the first trimester. The systemic vascular resistance also slightly decreases due to smooth muscle relaxation and overall vasodilation caused by elevated progesterone. Diastolic blood pressure consequently decreases If the blood pressure becomes abnormally high, the woman should be investigated for pre-eclampsia and other causes of hypertension.
Cardiovascular changes Stroke volume +30% Heart rate +15% Cardiac output +40% Oxygen consumption +20% SVR (systemic vascular resistance) -5% Systolic BP -10 mm. Hg Diastolic BP -15 mm. Hg Mean BP -15 mm. Hg
Cardiovascular changes Blood volume +30% Plasma volume +40% Red blood cell volume Dilutional anemia Increase cardiac output Vasodilatation +20%
Hematologic system Blood volume Dilutional anemia Leukocytosis Platelet Sedimentation rate +40% Hb 110 g/L 15, 000/ml not change increase, 100 m/h
Hematologic system Clotting factors: hypercoagulable, throboembolism Fibrinogen (factor I) +50% (4. 5 vs 3 g/L) Factor VIII increase Factors VII, IX, X and XII increase Prothrombin time, PT shortened activated partial thromoplastin time shortened Fibrinolytic activity decrease
Hematologic system Iron : active transplacental transfer Requirement 1000 mg increase maternal red cell mass 500 mg fetal development 300 mg compensate for normal iron loss 200 mg To supply, 300 mg of ferrous sulfate is needed, and twice the dose for anemic patients.
Pulmonary changes Mucosal hyperemia Subcostal angle Chest circumference and diameter Tidal volume +30 -40% PO 2 is increased, PCO 2 is decreased. Total lung capacity decrease Minute ventilation Mild respiratory alkalosis -15% +30 -40%
Gastrointestinal change Morning sickness hyperremesis gravidarum (weight loss, ketonemia and electrolyte imbalance) Dietary craving: pica Decreased gastrointestinal motility: reflux and heartburn Gallbladder function, cholestasis Hyperemia and softening of the gums (epulis) Hemorrhoid Appendix displaced
Renal changes Kidney Renal plasma flow Glomerular filtration rate Serum creatinine, uric acid urea and nitrogen Renin, angiotensin I and II Renin substrate Glucosuria slightly enlarged +35% +50% (50%) +
Renal changes renal pelvis Ureters (esp. right side) Bladder tone Bladder capacity Residual volume Chance of pyelonephritis dilated reduced increased increaased
Breasts Engorgement and venous prominence Mastodynia (breast ternderness): tingling to frank pain caused by hormonal responses of the mammary ducts and alveolar system Montgomery’s tubercles: enlargement of circumlacteal sebaceous glands of the areola Colostrum secretion
Skin changes Vascular spiders Striae gravidarum Hyperpigmentation (estrogen and melanocyte-stimulating hormone) Linea alba——linea nigra Chloasma ( Face Mask) Skin nevi
Reproductive tract Uterus: from <2%- 15 50 g - 1100 g < 10 ml – 5 L 20% of cardiac output Isthmus uteri —— lower segment of the uterus
Reproductive tract Braxton Hicks contraction: sporadic, irregular, asymmetrical, and painless, low pressure, lasting < 30 sec
Characteristics of True and False Labor Regular Contractions Stronger, longer, closer together Bloody show often present Cervix effaced and dilated Head is fixed between contractions Sedation does not stop true labor Irregular No change in contraction characteristics No show No cervical change Head may be ballotable Sedation stops false labor
Reproductive tract Cervix and vulva , Chadwick’s sign congestion of the pelvic vasculature, cause bluish or purplish discoloration of the cervix and vulva Leukorrhea: increase in vaginal discharge, rich in glucose, lactic acid, low vaginal p. H Ovary: slightly enlarged, corpus luteum regresses after 10 12 weeks’ gestation
Metabolism Basal metabolism rate, BMR +15 -20% Weight gain 12. 5 kg Fetus 3400 g Placenta 650 g Amniotic 800 g Uterus 960 g Plasma, red cells 1450 g Mammary glands 405 g Extracellular, extravascular water 1480 g Deposition of fat and protein 3345 g Insulin resistance
1. Musculoskeletal qa woman's foot can grow by a half size or more during pregnancy, the increased body weight of pregnancy, fluid retention, and weight gain lowers the arches of the foot, further adding to the foot's length and width. q. The influences of increased hormones such as estrogen and relaxin initiate the remodeling of soft tissues, cartilage and ligaments. Certain skeletal joints such as the pubic symphysis and sacroiliac widen or have increased laxity.
Lumbar lordosis
Immune system the immune system significantly changes during pregnancy and these changes are essential for normal placentation and maintenance of a healthy pregnancy pregnant women are more sensitive to certain infections This raises questions on the safety of vaccination during pregnancy
placenta & fetal circulation
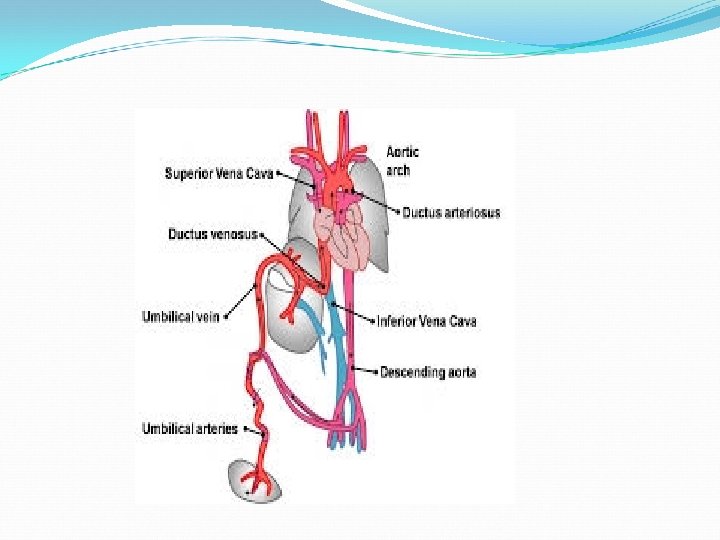
Anatomy And Physiology - Fetus depends on placenta to meet O 2 needs while organs continue formation -oxygenated blood flows from the placenta to the fetus via the umbilical vein - After reaching fetus the blood flows through the inferior vena cava
The Placenta - The circulatory system of the mother is not directly connected to that of the fetus, so the placenta functions as the respiratory center for the fetus - As well as a site of filtration for plasma nutrients and wastes. Water, glucose, amino acids, vitamins, and inorganic salts freely diffuse across the placenta along with oxygen. - The uterine arteries carry oxygenated blood to the placenta, and permeates the sponge like material there.
Fetal Circulation : - Facilitates gas and nutrient exchange between maternal and fetal blood. Umbilical cord - 2 umbilical arteries: - Return non-oxygenated blood, fecal waste, CO 2 to placenta - 1 umbilical vein : brings oxygenated blood and nutrients to the fetus
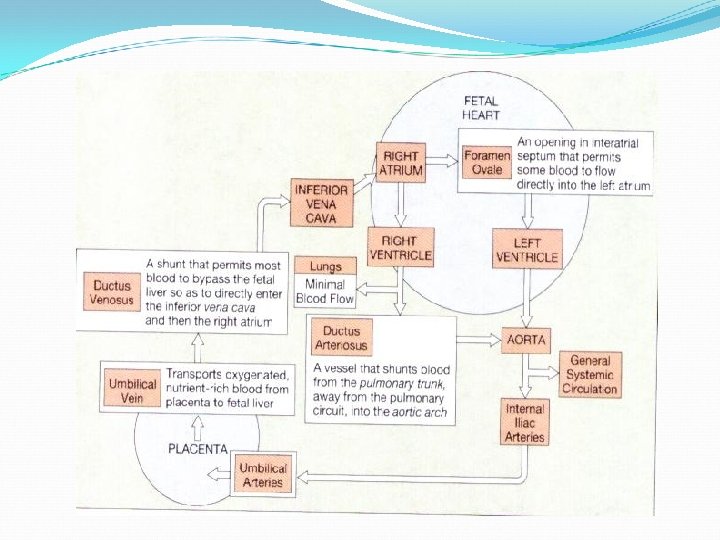
How does the blood move? ? - Umbilical vein carries oxygenated blood and nutrients from the placenta to the fetus. How is the blood dispersed? ? - ½ Of the blood enters the liver while the other half comes into the ductus venosus and then into the inferior vena cava
Foramen Ovale - Blood is shunted from right atrium to left atrium, skipping the lungs. - More than one-third of blood takes this route. - a valve with two flaps that prevent back-flow.
What is happening further down? ? - Common iliac arteries branch into the external and internal iliacs. - The blood in the internal iliacs come into the umbilical arteries and flow back to the placenta to gather oxygen and to get rid of the waste products - Some of the blood moves from the aorta through the internal iliac arteries to the umbilical arteries, and reenters the placenta, the maternal circulation
FETAL CIRCULATION - Low pressure system - Lungs are closed - Most oxygenated blood flows between the atria of the heart through the foramen ovale - This oxygen rich blood flows to the brain through the ductus arteriosus
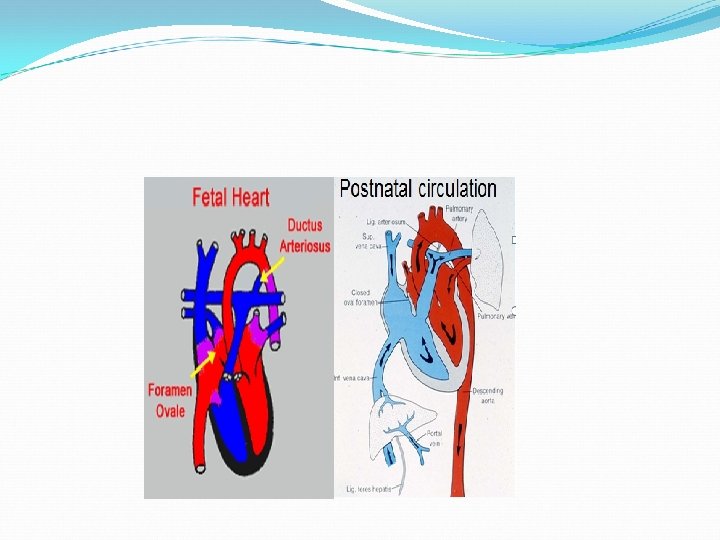
What happens after birth? Once the baby is born and the lung, renal, digestive and liver functions are working the fetal circulation undergoes some changes since they are no longer needed
Conversion Of Fetal To Infant Circulation Ø At birth - Clamping the cord shuts down low-pressure system - Increased atmospheric pressure(increased systemic vascular resistance) causes - Lungs to inflate with oxygen - Lungs now become a low-pressure system - Pressure from increased blood flow
Conversion (cont) What happens to these special structures after birth? - Umbilical arteries atrophy - Umbilical vein becomes part of the fibrous support ligament for the liver - The foramen ovale, ductus arteriosus, ductus venosus atrophy and become fibrous ligaments
Overview Of Conversion - Umbilical cord is clamped - Loose placenta - Closure of ductus venosus ductus arteriosus, foramen ovale - Blood is transported to liver and portal system
Fetal vs. Infant Circulation Fetal - Low pressure system - Right to left shunting - Lungs non-functional - Increased pulmonary resistance - Decreased systemic resistance Infant - High pressure system - Left to right blood flow - Lungs functional - Decreased pulmonary resistance - Increased systemic resistance
q A 25 year old patient presents with a 4 cm ovarian cyst on exam, she is 10 weeks pregnant, Management may includes A. Laparoscopy B. laparotomy C. Reassurance, and repeat scan in 3 -4 weeks D. Cancer screening
q In a normal singleton pregnancy, maternal blood volume A. increases by 10 -15% B. increases by 45% C. decreases by 10 -15% D. decreases by 45%
q Which of the following is not characteristic of a normal pregnancy? A. A. cardiac volume increases by 10% B. B. the rest pulse rate increases by approximately 10 -15% beats per min C. C. arterial blood pressure and vascular resistance increases D. D. The heart is displaced upward and to the left
q. A pregnant lady was told by her physician that she has Epulis, which is a pregnancy-related vascular swelling of the: A. A. Gums B. B. Nail bed C. C. Larynx D. D. Nares