PHYSICAL THERAPY IN CARDIOTHORACIC SURGERY By Prof Naguib

PHYSICAL THERAPY IN CARDIOTHORACIC SURGERY By Prof Naguib Salem Cairo University

Cardio-thoracic surgeries n Cardio-thoracic surgery is a long established surgical specialty which deals with operations on the heart and the lungs. These are major operations which involve opening the chest and require highly specialised medical staff and a dedicated intensive care unit.

Cardiothoracic Surgeries n There has been an increase in the number of coronary artery bypass operations and lung operations in the past years and this increase will continue as this type of surgery is a national priority for the results of PULLOTION

The heart and the lung
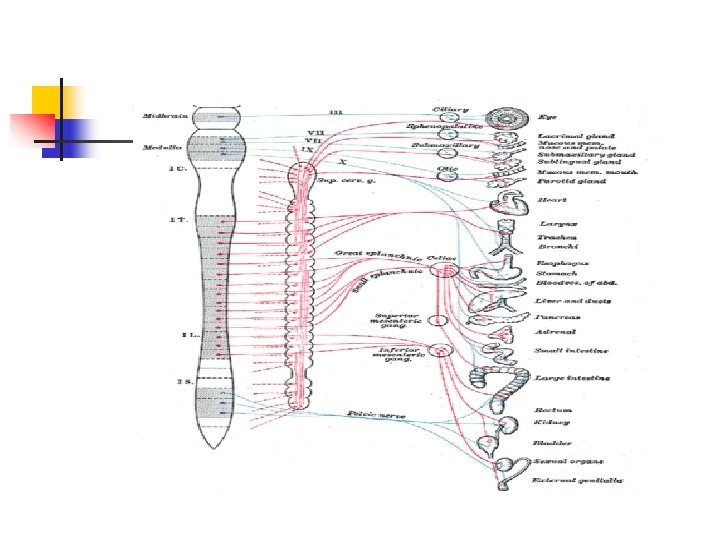

Capillaries and Veins

Lung Volume Reduction Surgery Why do I need physiotherapy for this surgery? n n How do I prepare for this surgery? How do I know this surgery is right for rehabilitation?

Emphysema

Diseased Lung

Cardiothoracic Management n Preoperative n Intra operative n Postoperative

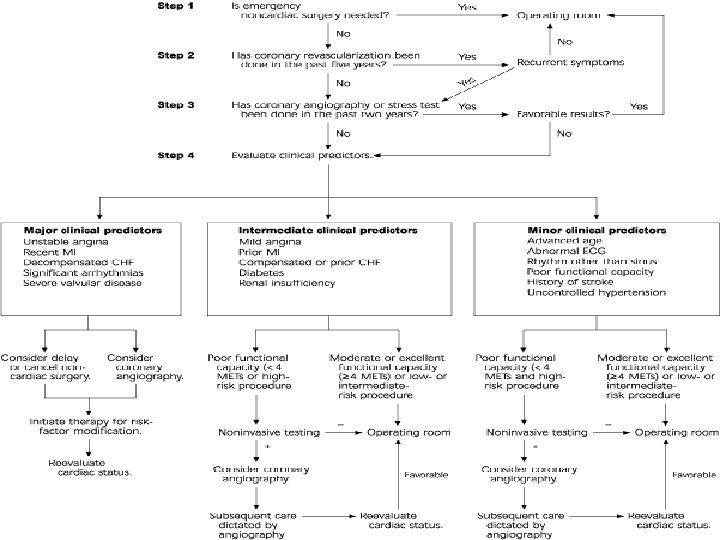
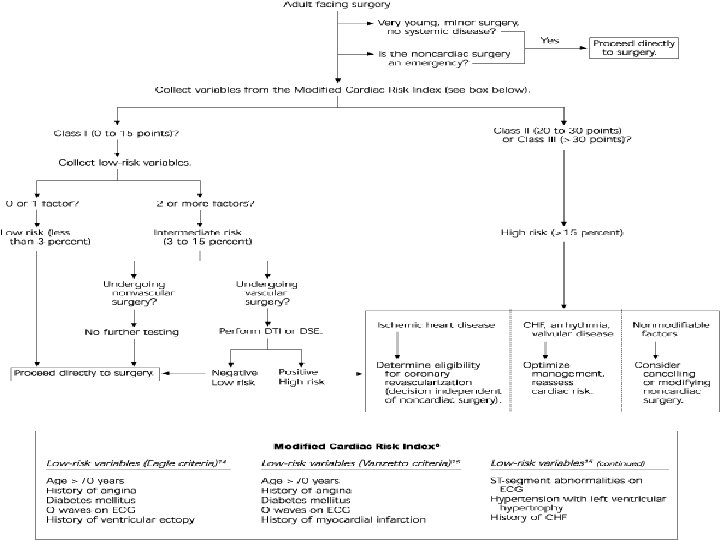
Cardiothoracic Management Screening and preparation 1 - Functional capacity to tolerate operation. A- Functional pathology. Preoperative impairment of vital functions and physiologic insult produced by the planed operative procedure together form the principle basis for postoperative morbidity and mortality. n

Cardiothoracic Management n B- Pathological Anatomy The functional pathology and operative plan must be established from the diagnostic studies. Safe and effective thoracic surgery cannot be performed without accurate reliable and unmistakable diagnostic studies.

Cardiothoracic Management n I-Controllable factors affecting operative morbidity and mortality. 1 - Impaired output. To facilitate the needs during surgery by drugs or assistance instrumentations. 2 - Arrhythmias. Use of transvenous pacemaker

Cardiothoracic Management 3 - DRUG MANAGEMENT A- Cardiac dysfunction. a-Cardiac glycosides should be withheld 24 hours preoperatively for open heart surgery. b-Anticoagulant To control preoperative throboembolism. c- Aspirin To diminish platelet adhesiveness d- Diuretics to avoid hypovolumic effects especially in heart failure.

Cardiothoracic Management B-Pulmonary dysfunction. Ventilatory capacity evaluation a- Measurements of percent predicted vital capacity (MIF-MVV- FEV 1 -) B- Exercise tolerance. Measure of ventilatory volume C- Blood gas determinations. (Respiratory acidosis-Co 2 retention-hypoxia. Arterial co 2 tensions D- Ventilation perfusion. To maintain postoperative functions. E-Pulmonary artery pressure will reveal pulmonary hypertension.

Types of operations In Cardiac surgery
")
Angiography( Catheterization)

Coronary Balloon

Stent Of Coronaries

In Theater

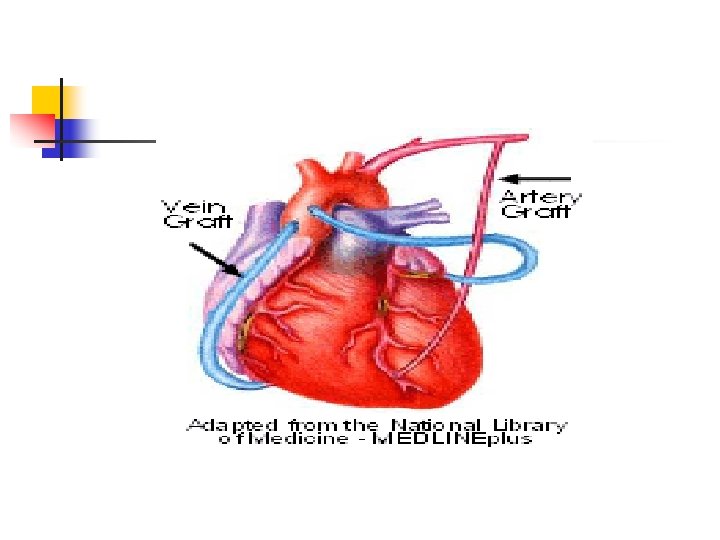
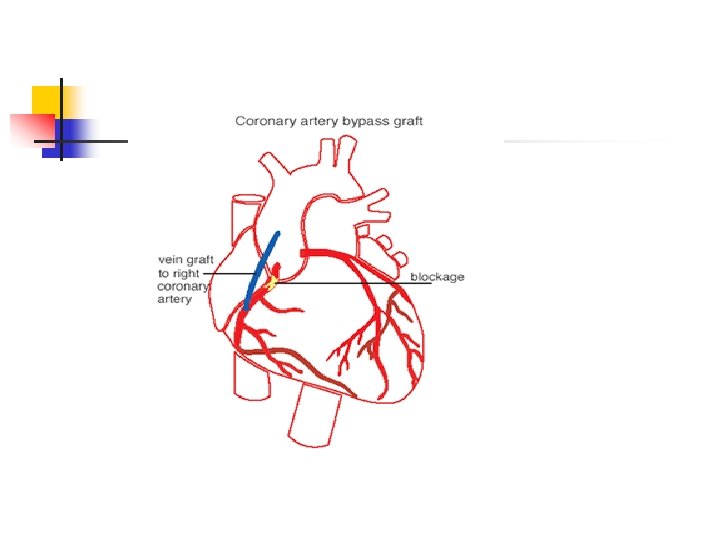
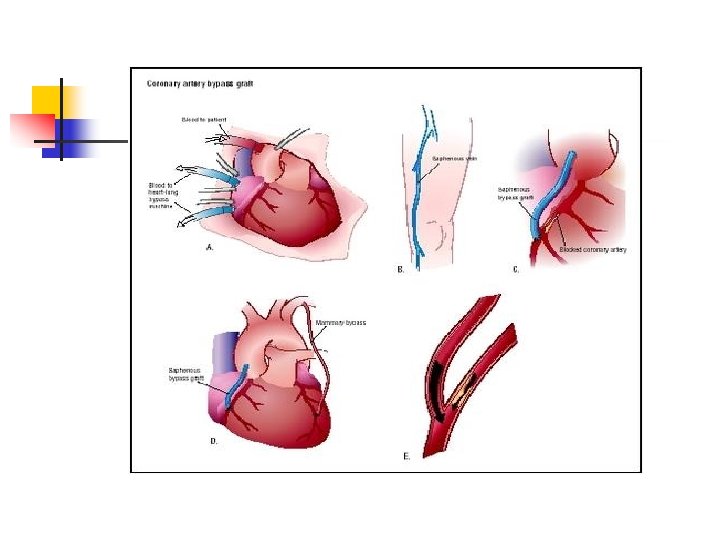
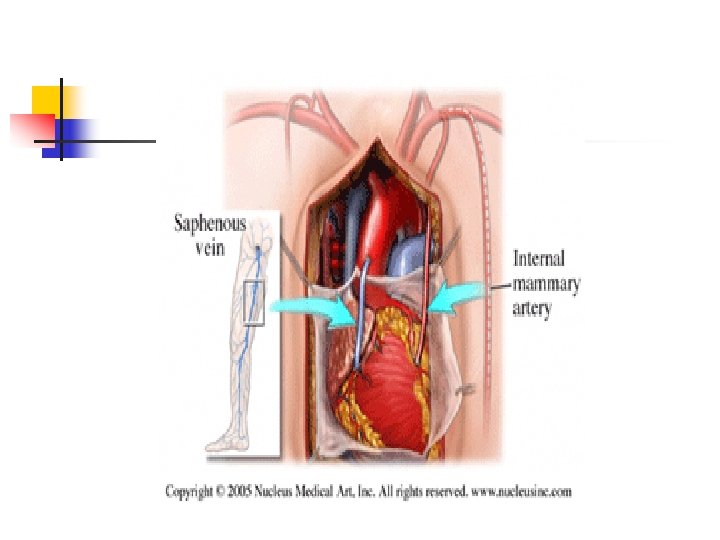
Outcomes Of CTS: n n CABG significantly improves symptoms of angina and quality of life, exercise capacity and reduces the need for anti-anginal therapy compared with medical treatment. Over 75% of patients are free of ischaemic events at 5 years and nearly 50% at 10 years. There is less limitation of physical activity. At 10 years the benefit of CABG over medical therapy is lost in those who had only saphenous vein grafts but after arterial grafts it remains.

Survival improvement n n Survival is improved with the greatest relative benefit going to those with left main stem stenosis of >50%. Patients with angina triple vessel disease or two vessel disease including proximal LAD stenosis also survive longer but those with two vessel disease excluding proximal LAD stenosis or with single vessel disease gain no survival advantage. Patients with abnormal left ventricular function or strongly positive exercise tests derive greater absolute survival benefit from coronary artery bypass surgery than from medical therapy. In summary, results are best with: n n significant left main stem stenosis of 50% or more triple vessel disease two vessel disease including a significant proximal LAD stenosis impaired left ventricular function or strongly positive exercise test

The outcomes of operative mortality rate in CTS n It is around 1 to 3% but varies according to case type. Both operative mortality and outcome are more likely to be adverse in the following: n n n n n Increasing age Smoking Being female (the reason for this is debated but is probably multifactorial) Diabetes Overweight or obesity Being short Other illness LMS disease, poor LV function and multivessel disease If the operation was an emergency for unstable angina or shortly after myocardial

Physical therapy In Cardio thoracic Surgery PHYSICAL THERAPY IN CARDIOTHORACIC SURGERY IS A PREMATIVE PROTOCOL FOR THE SACK OF THE PATIENTS IN THESE DEPARTMENTS

n . Understanding of the feeling , attitude concerns of the members of the profession. The patient served , and the public in general is necessary when therapist evaluate, planes and implement the practice of physical therapy.

Introduction n Chest physical therapy is used in the intensive care unit to minimize pulmonary secretion retention and strength the inside muscles with improving the pulmonary oxygenation. n 3

. n Management of cardiothoracic surgery was to reduce the post operative complications.

Introduction Up to 15% of patients suffer from respiratory complications because of general anaethesia The role of prevention by encouragement of breathing exercises cough and lower limb exercises. .

Causes Of Pulmonary complications 1 - Pherenic nerve injury. n 2 - Rib cage mechanical changes. . n 3 - Wound infections. n 4 - Anaesthia n

Factors of increasing the incidence of pulmonary complications Smoking. n Pain due to sympathetic activation and endocrine stress. n Obesity n Pre-existing pulmonary disease. . n

Physical Therapy Program n Physical therapy role starts at the day before operation and continued to the seventh day after operation in hospital. Avoidance of the aggression, aniexity , emotional disturbances and personality changes which forms 15% of the postoperative complications is the major aim.

Preoperative Physical therapy n Education. 1 -Explain the importance of post operative breathing exercises. 2 - Explain the importance of diet control. 3 -Teach the patient Shoulder and leg exercises.

Preoperative Physical therapy n Tests n Objective n n 1 - Cardiac catheterization in cardiac problems. 2 - Pulmonary functions. 3 - Arterial blood gases. 4 - E. C. G. and Echocardiography.

Analysis

Preoperative Physical therapy n Tests n Subjective 1 n 2 n 3 n 4 n Respiratory rate Exercise tolerance Chest and heart sounds. Sputum examination

1 -The immediate postoperative Ph Th goals related to excubation , oxygen transport and airway closure are: n n a- Maximize alveolar volume and ventilation b- Maximize lung volumes and capacities (FRC) c- Optimize lung compliance d- Optimize mucous clearance e- Maximize chest wall mobility f- Maximize EFR g- Minimize undue work of the heart h- Promote optimal lymphatic drainage

2 - Other important goals are: a- Maximize joint range of motion b- Maximize muscle length and ligament integrity c- Maximize patient ability to perform ADL d- Maintain or increase general muscle strength and endurance e- Maintain normal cognitive function to avoid disorientation and hospitalrelated psychoses

3 - Preventive goals Preventing or minimizing the effect of restricted mobility and recumbence on all organ system such as: - Risk of DVT - Pulmonary embolism - Pressure points - Skin breakdown - Delay healing processes (chestlimbs

4 - Beneficial effects of early mobilization 1 - Augments cardiopulmonary function 2 - Enhances three dimensional chest wall motion and decreases atelectasis 3 - Reduces intra abdominal pressure 4 - Enhances ventilation and perfusion matching of the lungs 5 - Relaxed upper body musculature 6 - Enhances oxygen transport pathway 7 - increases peripheral blood flow and decreases DVT

Postoperative Physical therapy n n n The exercise therapy as a rehabilitation process divided into four phases : 1 -Phase I : Hospital inpatient period. 2 -Phase II : Convalescent after hospital discharge. 3 -Phase III : Supervised ongoing rehabilitation. 4 - Phase IV: Unsupervised ongoing rehabilitation. n ( AACPR)

Postoperative Physical therapy n n Criteria's For Post-operative Physical therapy 1 - P. T. starts after 6 -12 hours after operation. 2 - Keep systolic blood pressure below 150/90 mm. Hg. 3 - Activity should be slowly increased and include graduated exercise and mobilization

Postoperative Physical therapy n n Program Of Physiotherapy 1 -Mobilization: It should be considered a primary intervention to stimulate deep breathing , secretion removal and efficient myocardial performance and oxygen transport.

Postoperative Physical therapy n n Program Of Physiotherapy 2 -Ambulation. n It is required for normal physiological functioning of the human body to stimulate exercise stress and gravitational stress and thereby optimize oxygen transport.

Postoperative Physical therapy n n n Program Of Physiotherapy 3 -Chest Therapy It is prescribed for prophylaxis or treatment of the pulmonary complications A- Breathing exercise. B- Incentive Spiro meter. Intermittent positive pressure breathing.

Postoperative Physical therapy n n n Program Of Physiotherapy Breathing exercise in form of Quite breathing Huffs. Forced expiration(Pursed lip) Active cycle of breathing techniques.

Postoperative Physical therapy n n n Program Of Physiotherapy: 4 - Transcutaneous Electrical Nerve Stimulation(TENS). It is a useful method of gaining pain relief in the context of a physical therapy department and could facilitate the other physical therapy modalities. It was demonstrated at the 1 st 3 days of post thoracotomy for ten minutes by improving the ventelatory measures.

Advises n n n 1 - Medications: Must follow the surgeons advises. 2 - Diet : Low fat diet and care of body weight. 3 - Smoking: must be stopped. 4 - Temperature: Avoid very cold or hot. 5 - Activities : Do not hurry or compete. Warm up and cool down.

Advises n n n 6 - Tension : Avoid tension 7 - Exercise: A-Increased gradually. B- Not less than 15 minutes C-Minimum of 2 -3 times/week. D-Must be of 2 hours after meal 8 - Walking: A-Increase distances slowly. B-Wear lose clothes and comfortable shoes. C-Must be rhythmical and prevent blood from pooling by sudden stop.

Advises n n n SPECIALLY IN CARDIAC SURGERY 9 - Sexual activity: After doing 2 -3 flight of stairs because it will cost 5 -6 Met /kg. 10 - Work : After 3 months by light office work , heavy work by consultation. 11 -Driving: After 2 months. 12 - Travel : After Phase 1(10 days) and avoid long travel.

Problem list postoperative: The problems that may arise after surgery can be listed as: IPain 2 Decreased air entry 3 Retained secretions 4 Reduce arm and leg movement 5 Decrease mobility

Post Operative Complications: n n 1 - Thrombosis: Thrombosis of the deep veins of the leg, which may lead to a fatal pulmonary embolism, is always a postoperative danger. The physiotherapist may be the person who discovers this during an exercise period, so must be always watchful for the symptoms.

2 - Wound infections n These are due the prevalence of bacteria, particularly resistant types. Infections occur even in clean, cold surgery despite the existence in most hospitals of towns whose task it is to combat infection.

3 - Pressure sores: n Any patient confined to bed must be watched constantly by all who care for him to prevent pressure sores occur-ring. These may have been precipitated by pressure while on the operating table or they may occur later. Pressure can be caused also from within the tissues by edema. Vigilance is especially needed when the patient is old, unconscious, immobile, incontinent, or diabetic.

4 - Hemorrhage: n Another complication' is hemorrhage. This can be primary, occurring within the first 24 hours, or secondary, when it can take place up to three weeks postoperatively

5 - Muscle wasting and impairment of function: n Incisions are very extensive and divide, or in extreme cases damage, muscle or nerve tissue, there may be resultant muscle wasting and impairment of function. This can lead to faulty posture, deformities and, occasionally, stiff joints.

6 - Cardiac arrest: n Cardiac arrest requires immediate action to prevent irreversible brain damage. It is vital that it should be recognized at once by everyone who comes in contact with the patient, and that the appropriate action is known and instantly followed.

7 - Respiratory Problems: n Respiratory complications are liable to follow any operation in which general anesthesia is used. They are most common in thoracic surgery since, , in many cases, the lung function may be impaired already. After thoracic surgery the highest incidence is probably in abdominal operations, particularly those which require a supraambilical incision.

8 - Neurological Damage: n Disorders of the central nervous system frequently follow thoracic surgery. The pathological mechanisms causing these cerebral syndromes are not clearly established. The most likely cause is impaired perfusion causes dysfunction or infarction of the neurons.

9 - Renal failure: n n Renal failure is a common complication of open-heart surgery. Factors to post operative renal failure include preoperative renal dysfunction, nephrotoxic drugs, transfusion, low cardiac output and cardiopulmonary bypass.

Recommendations 1 -More attentions to preoperative and post operative physical therapy cardiothoracic surgery. n 2 -Care of breathing exercises for pre and post operative management. n

Recommendations 3 - Assessment of the patients must be carefully done. n 4 -Develop of more programs in cardiothoracic rehabilitation for surgeries and disease. n
 that enters the pleural space, thus providing")
PLEURAL DRAINAGI n Any operation (or trauma) that enters the pleural space, thus providing the basis for collection of air or fluid that can impair pulmonary expansion, must be accompanied by effective measures to keep that space evacuated postoperatively and to maintain appropriate negative pressure within that potential space. Pleural drainage is, therefore, a cardinal adjunct to thoracic surgery.

PHYSIOLOGIC PRINCIPLES n A slight negative pressure of 3 to 5 mm Hg is maintained in the normal "nonexistent" pleural space because the inflated elastic lung is prevented from collapsing within its semirigid chest cage container [4]. Pleural drainage, therefore, requires an air-tight seal to prevent losing that vacuum and some mechanism for maintaining negative pressure, even with normal anatomy and physiology.

PHYSIOLOGIC PRINCIPLES n n n Vacuum requirements to obtain and maintain full pulmonary inflation, and thus to achieve adequate pleural drainage, may be increased considerably above normal values when there is: 1. Ingress of air or fluinto the pleural space tending to neutralize the vacuum 2. Loss (by resection) of available lung volume to fill the space 3. Atelectasis resulting in effective reduction of lung volume 4. Obstruction of the endobronchial airway preventing full expansion of the lung to fill the space

PHYSIOLOGIC PRINCIPLES n n n When obliteration of the pleural space is impaired by one or more of the above conditions, there are mechanisms that help to reduce the space and correct the discrepancy: 1. Shift of a flexible mediastinum toward the side with collapsed or deficient lung volume. 2. Elevation of the hemidiaphragm.

PHYSIOLOGIC PRINCIPLES n n 3. Compensatory of residual lung tissue. 4. Surgical measures to obliterate residual space. 5. Fusion between the visceral and parietal pleura so as to seal and permanently obliterate the pleural space can be promoted by introduction of reactive agents to promote pleural scarring. Nitrogen mustard, colloidal gold, arabrine, and retracycline are among those, which have been use

MANAGEMENT OBJECTIVES OBLITERATION OF THE PLEURAL SPACE n n n When the lung is fully expanded and there is total apposition of the visceral and parietal pleural surfaces, there will be no space. This state is the cardinal objective of pleural drainage EVACUATION OF FLUID All fluid must be removed to achieve full expansion of the lung and to remove the potential source of subsequent empyema.

CLOSURE OF AIR LEAKS n When all of the lung surfaces (from which the air may be leaking) are in apposition with the parietal tissue, most surface air leaks will seal and cease. Air leaks of a magnitude which exceeds the capacity of the pleural drainage system to maintain an effective vacuum must be treated by alternative methods:

CLOSURE OF AIR LEAKS n n 1. Re-operation within the first 2 or 3 days is likely to reveal a defect large enough for effective surgical closure. 2. Some surgeons (with whom I disagree) believe that the higher vacuum worsens the leak and, therefore, they allow the lung to collapse temporarily to promote scaling the air leak. This method, moreover, may lose the opportunity to obliterate the space and thus increase the chance of either subsequent empyema or encapsulated and permanently unexpanded lung

PERSISTENT AIR LEAK n A broncho-pleural fistula in the presence of a potentially obliteratable pleural space can usually be converted into a bronchocutaneous fistula with merely a narrow fistulous tract traversing the picural space to the drainage tube; such a tract, if sealed from communication with the main pleural space, will always close spontaneously, no matter how long it has been functioning. This objective, however, can be accomplished only if adequate uninterrupted pleural vacuum is maintained to keep the pleural surfaces in constant apposition long enough for total and permanent adhesions to develop (1014 days).

FREE AIRWAY n Airway communication to all segments of the underlying lung is obviously essential for the full inflation required to obliterate the pleural space. Meticulous tracheobronchial toilet and encouragement of coughing are essential adjuncts to the mechanics of pleural space obliteration
 n A wide variety of tubes have been used for")
DRAINAGE PATHWAYS (THORACOSTOMY TUBES) n A wide variety of tubes have been used for pleural drainage. Nearly all of them have some practical or theoretical disadvantage and experience reveals that none function with total reliability. Certain physical characteristics and principles of use arc worthy of consideration.

LOCATION OF THE TUBE'S n n n ACCESS TO THE PLEURAL SPACE COMFORT OF THE PATIENT MEDIUM TO BE EVACUATED COSTOPHRENIC SULCUS DURATION OF PLEURAL DRAINAGE Thoracostomy tube drainage should be continued only as long as it. appears to be effective
- Slides: 80