Physical Examination Definition It is examination of the












































 Respiratory distress")

")






















")


- Slides: 82
Physical Examination
Definition: It is examination of the body from the head to the toes, it is a continuous process that begins the interview primarily by using inspection, palpation, percussion and auscultation
Objectives of physical assessment -To formulate nursing diagnosis -To evaluate the effectiveness of intervention
Suitable time for physical examination: • Each month during the first year of life • Each 3 months during the 2 nd and 3 rd years • Each 6 months during the 4 th and 5 th years • Yearly from the 6 th year throughout life
Sequence of the assessment In adult the physical examination proceeds in a head to toe direction and from general inspection to detailed investigation In pediatrics, the age of the child frequently alters this sequence of performance
Assessment skills Inspection
Assessment skills Palpation
Assessment skills Percussion
Assessment skills Auscaltaion
Out lines of a physical assessment 1. Growth measurements Length, weight, head circumference, chest and arm circumference 2. Physiological measurements Temperature, pulse, respiration and blood pressure
3. General appearance 4. Skin 5. Accessory appendages 6. Lymph nodes 7. Head 8. Neck 9. Eyes 10. Ears 11. Nose 12. Mouth and throat 13. Chest, lung 14. Heart 15. Abdomen 16. Genitalia 17. Anus 18. Back and extremities 19. Neurological assessment
3. General appearance A-Facial expression
3. General appearance B- Posture, Position
3. General appearance C- Hygiene
3. General appearance D- Nutrition
3. General appearance E- Behavior • Child's personality • Level of activity • Reaction to stress Requests • Frustration • Interactions with others and response to stimuli • Is the child's calm, anxious, tense, aggressive, stable, talkative or restless
3. General appearance F- Development An overall estimate of the child's speech development, motor skills, and degree of coordination and recent area of achievement
4. Skin
4. Skin A- Color such as, red, blue, yellow or orange, are abnormal Other abnormal colors as pallor and cyanosis, erythema, ecchymosis and petechiae or jaundice
Acne
B-Temperature
C-Turgor
5. Accessory organs A- Hair
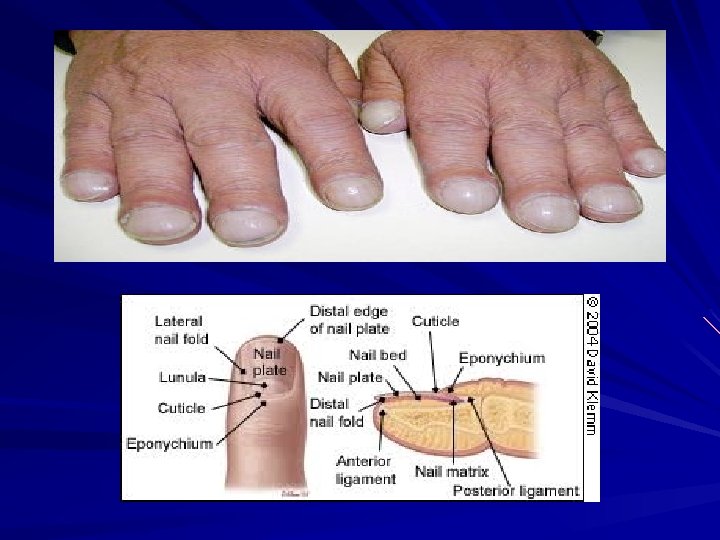
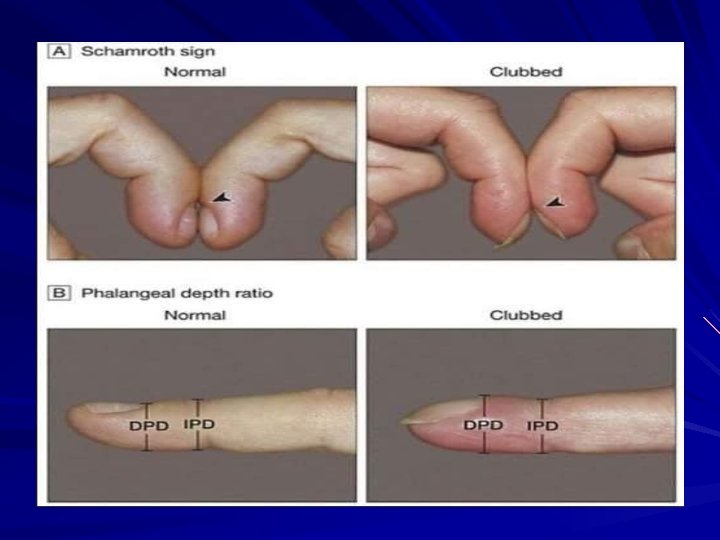
5. Accessory organs B- Nails
C- Dermatoglyphics
6. Lymph nodes
Inspect & palpate lymph nodes for size, location, temperature, tenderness, firmness & mobility
7. Head
Microcephalus Bulging anterior fontanelle Eyes deviated downward “Setting” Sun sign Hydrocephalus
8. Neck
Mumps
9. Eyes size color, symmetry, motility, inner canthus distance 3 cm. sclera, cornea, pupil, iris
Hypertelorism
Fixed and dilated pupil
Fundoscope Ophthalmoscope
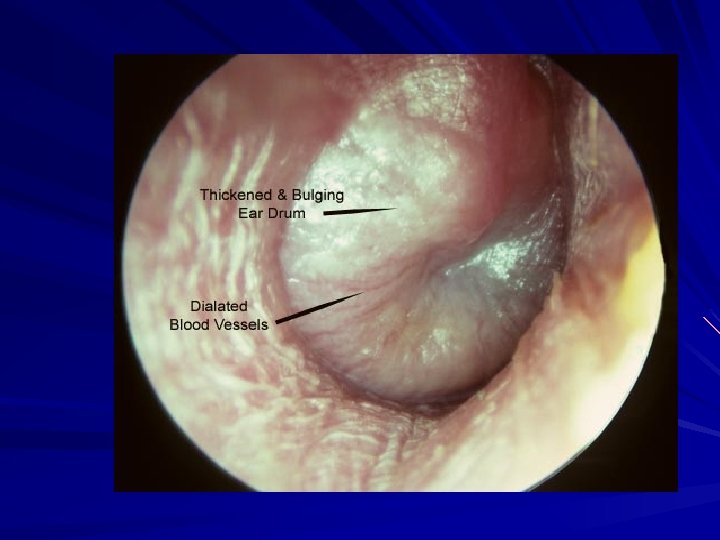
10. Ears
· Hearing · Otoscope exam: pull auricle down & back for infants, toddlers, preschoolers. Pull auricle up & back for school aged & adolescents
11. Nose: location, symmetry, size, discharge, flaring nose.
12. Mouth and throat lips, gum, teeth, tongue, oral cavity, mucous membrane, palate, uvula, tonsils
Bacterial tonsillitis
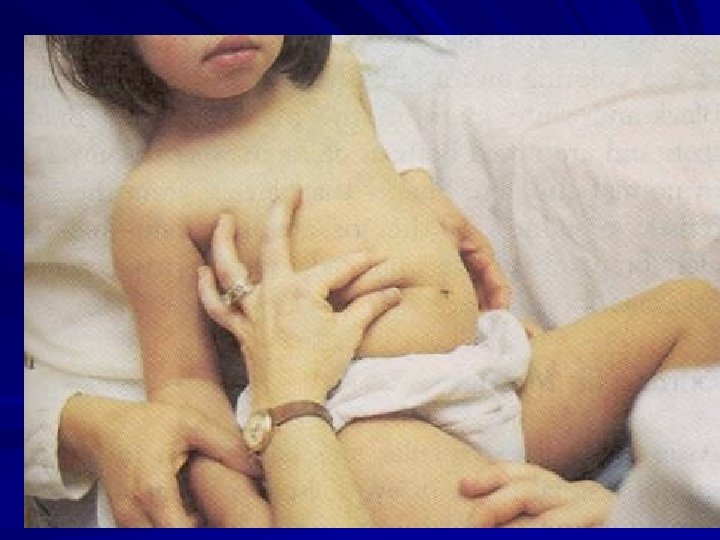
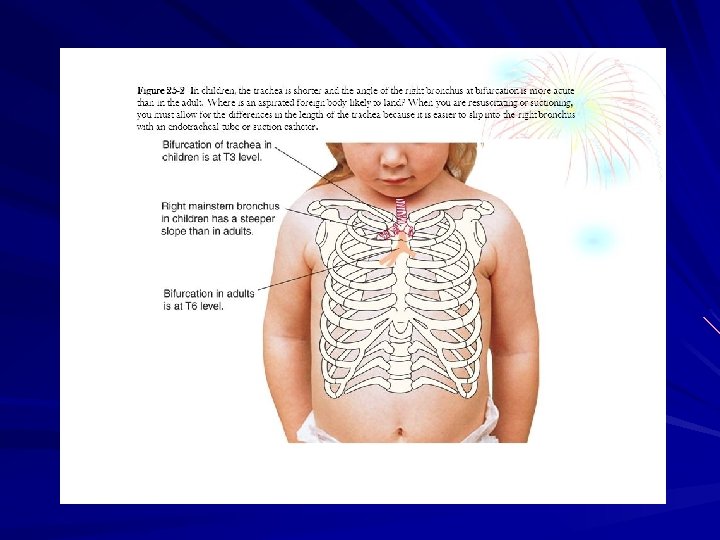
13. Chest and Lung
13. Chest and Lung Inspection Chest movement Rate and depth (tachypnea, hyperpnoea) Respiratory distress
13. Chest and Lung Palpation
Respiratory expansion (excursion)
Tactile fremitus
13. Chest and Lung Percussion The examination is usually. Initiated with percussion of posterior thorax. Ideally the patient is in a sitting position with the head flexed forward and the arms crossed on the lap
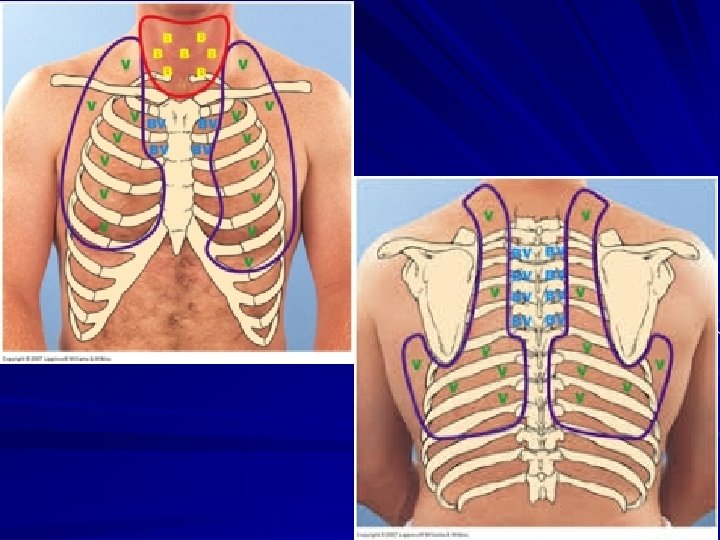
13. Chest and Lung Auscultation vesicular breath sounds Broncho-vesicular breath sounds bronchial breath sounds
Abnormal breathing sounds
14. Heart Inspection Inspect heart size, note obvious bulging, apical impulse some time appear in the thin child
14. Heart Palpation Point of maximum impulse Capillary filling time
14. Heart Percussion
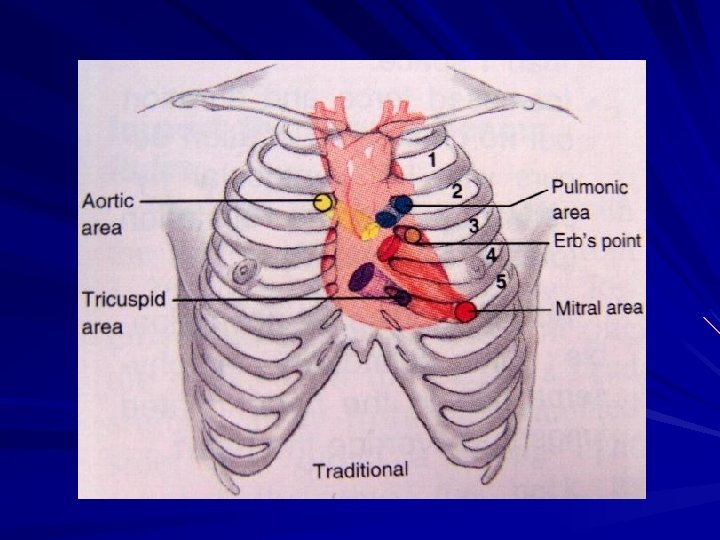
Auscultation
Auscultatory sites
The heart sounds are evaluated for: Quality: which should be clear and distant and not muffled or diffuse. Intensity: especially in relation to location or auscultatory site. Rate: which should be the same as the radial pulse. Rhythm: which should be regular
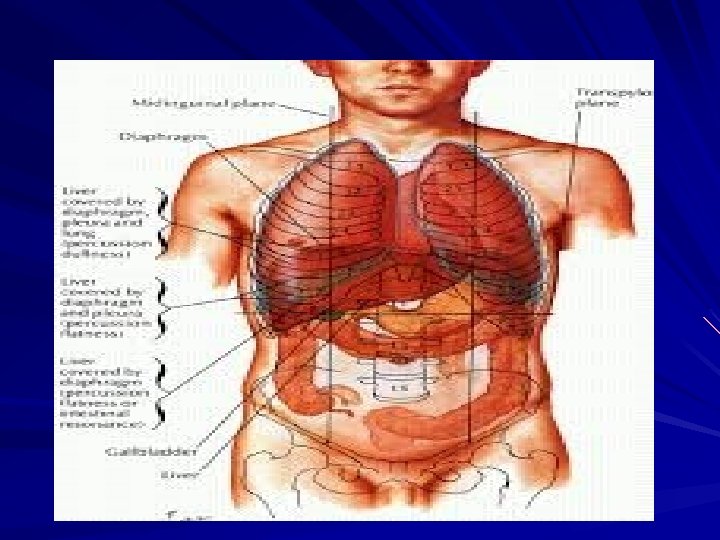
15. Abdomen
Abdomen The child is positioned in supine position during examination with pillow under the Head and the knee flexed to enhance abdominal relaxation. The abdomen is divided into four quadrants that correlate with underlying anatomical structures.
Umbilical Hernia
Measuring Abdominal Circumference
Palpation • • • Warm hands Distraction Light palpation Painful areas last Let child help you in palapation
16. Genitalia
Inguinal Hernia
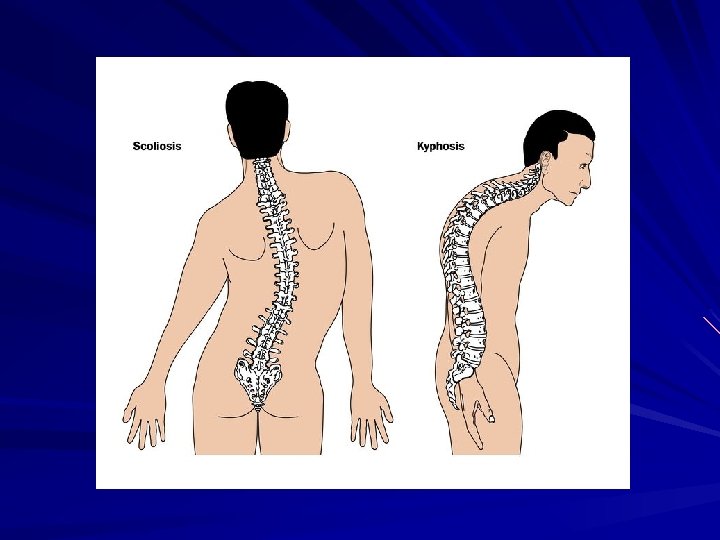
17. Musculoskeletal system Back & extremities is concerned of the spine , legs , hands , feet , joints & muscles
A. Spine: Newborn, infant: rounded or Cshaped Toddler : S shape
B. Extremities Bowlegs normal in infant and toddler Knock knee normal in preschool
C. Joints: Joints are evaluated for range of motion , heat tenderness & swelling. D. Muscles: Symmetry and quality of muscle development , tone & strength are noted. - Development is observed by looking at the shape of the body in both a related a tense state.
18. Nervous system Assess mental status Assess sensory intactness and discrimination
Assess reflexes for the new born and infants Blinking reflex Rooting reflex (4 months) Sucking (6 months) Swallowing Sneezing and coughing Gagging Grasping (6 months) Moro/startle (4 months) Tonic neck (5 months) Dancing (4 weeks)