PHRENIC NERVE PACER Bethany Jerabek DNP ARNP Maida

PHRENIC NERVE PACER Bethany Jerabek, DNP, ARNP Maida Lynn Chen, MD Director, Sleep Disorders Program Seattle Children’s Hospital

Objectives • Describe motives for transition to a phrenic nerve pacer • Identify how to transition to a phrenic nerve pacer • Focus: Eligibility for placement *The following are only suggested guidelines. Each individual case may require a different approach.

Why do you want Pacers? • • Freedom from positive pressure ventilation? Tracheostomy decannulation? Decrease amount of equipment? Decrease daily monitoring? Decrease hospital admissions or office visits? Increase mobility? Improve quality of life?

Myth 1: Phrenic nerve pacer placement is a surgery on the lungs.

BUSTED! • Phrenic nerve pacer placement is NOT a surgery on the lungs • Thoracoscopic placement approach used to to attach electrodes on the phrenic nerves bilaterally and implant a connected receiver below abdominal skin • Lungs must be deflated, one at a time, during surgery to attach electrodes • Recovery after surgery is related to deflated lungs

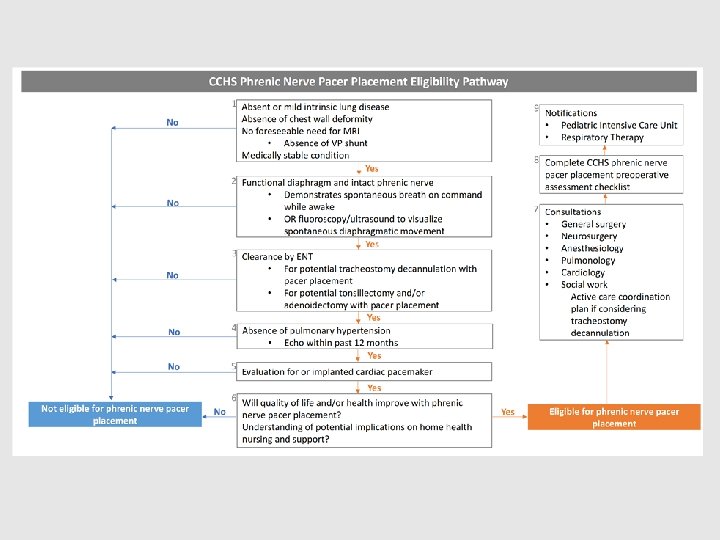
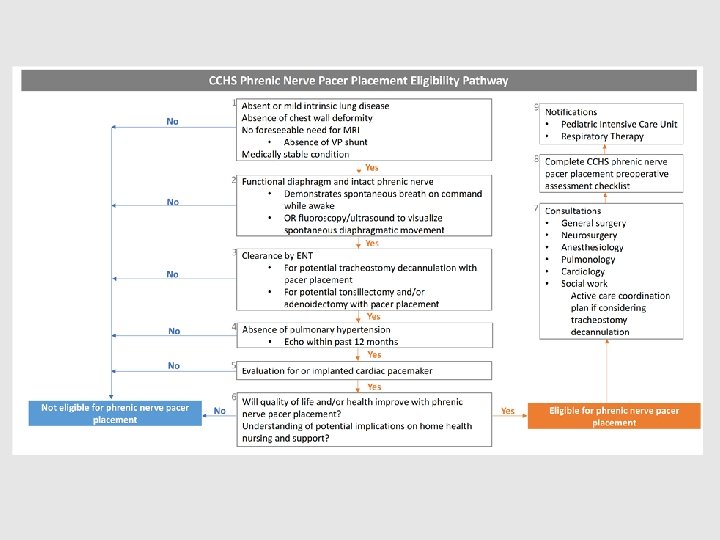
CCHS Phrenic Nerve Pacer Placement Eligibility Pathway 2 Functional diaphragm and intact phrenic nerve • Demonstrates spontaneous breath on No command while awake • OR fluoroscopy/ultrasound to visualize spontaneous diaphragmatic movement Yes

Myth 2: Phrenic nerve pacer placement guarantees tracheostomy decannulation.

BUSTED! • Phrenic nerve pacer placement does NOT guarantee tracheostomy removal • Difficult to predict until the pacer is in place • Tracheostomy may not be decannulated for several months following pacer placement • Tracheostomy cannot always be removed • Full-time ventilatory support vs. night-time ventilatory support • A backup plan for acute illness or pacer failure must still be in place • Positive pressure ventilation via mask or tracheostomy • Intubation

CCHS Phrenic Nerve Pacer Placement Eligibility Pathway 3 Clearance by ENT • For potential tracheostomy decannulation No with pacer placement • For potential tonsillectomy and/or adenoidectomy with pacer placement 3 Yes No 4 Absence of pulmonary hypertension • Echo within past 12 months Yes

Myth 3: An implanted cardiac pacemaker is required before phrenic nerve pacer placement.

BUSTED! • An implanted cardiac pacemaker is NOT mandatory for phrenic nerve stimulator placement • Phenotype dependent • History with prior anesthesia is important • Discretion of the surgeon, pulmonologist, pre-anesthesia evaluation • One-time ECG not necessarily helpful • More important to have well versed and prepared anesthesiologist (pediatric specific, experienced)

CCHS Phrenic Nerve Pacer Placement Eligibility Pathway No 5 Evaluation for or implanted cardiac pacemaker Yes

Myth 4: Home nursing care will remain the same.

BUSTED! • May have reduced home nursing care • Possible loss of daytime and school nursing care • More of a challenge to get support services • All children are individualized

CCHS Phrenic Nerve Pacer Placement Eligibility Pathway 6 Will quality of life and/or health improve with phrenic nerve pacer placement? No Understanding of potential implications on home health nursing and support? Yes

Myth 5: Phrenic nerve pacers make all future medical care easier.

BUSTED! • Phrenic nerve pacers will NOT always make future medical care easier • Not well known at all health care facilities • Without trach, looks no different than anybody else to EMS • Not MRI compatible • Require frequent attention and tinkering • Biannual or annual comprehensive evaluation • Cause artifact on transthoracic cardiorespiratory monitors • Costly system • Back-up pacer transmitter • Back-up Bi. PAP • No external alarms

CCHS Phrenic Nerve Pacer Placement Eligibility Pathway No 1 Absent or mild intrinsic lung disease Absence of chest wall deformity No foreseeable need for MRI • Absence of VP shunt Medically stable condition Yes

CCHS Phrenic Nerve Pacer Placement Eligibility Pathway 9 Notifications • Pediatric Intensive Care Unit • Respiratory Therapy 8 Complete CCHS phrenic nerve pacer placement preoperative assessment checklist 7 Consultations • • • Yes General surgery Neurosurgery Anesthesiology Pulmonology Cardiology Social work Active care coordination plan if considering tracheostomy decannulation Eligible for phrenic nerve pacer placement

Myth 6: Phrenic nerve pacers are the same as diaphragm pacers.

BUSTED!

References 1. Chen ML, Tablizo MA, Kun S, Keens TG. Diaphragm pacers as a treatment for congenital central hypoventilation syndrome. Expert Rev. Med. Devices. 2005; 2(5): 577 -585. doi: 10. 1586/17434440. 2. 5. 577 2. Trang H, Brunet J, Rohrer H, et al. Proceedings of the fourth international conference on central hypoventilation. Orphanet J Rare Dis. 2014; 9(194): 1 -24. doi: 10. 1186/s 13023 -014 -0194 -5 3. Rand CM, Carroll MS, Weese-Mayer DE. Congenital Central Hypoventilation syndrome a neurocristopathy with disordered respiratory control and autonomic regulation. Clin Chest Med. 2014; 35(3): 535 -545. doi: 10. 1016/j. ccm. 2014. 06. 010 4. Weese-Mayer DE, Berry-Kravis EM, Ceccherini I, Keens TG, Loghmanee DA, Trang H. An official ATS clinical policy statement: congenital central hypoventilation syndrome genetic basis, siagnosis, and management. Am J Respir Crit Care Med. 2010; 181(6): 626 -644. doi: 10. 1164/rccm. 200807 -1069 ST 5. Vanderlaan M, Holbrook CR, Wang M, Tuell A, Gozal D. Epidemiologic survey of 196 patients with congenital central hypoventilation syndrome. Pediatr Pulmonol. 2004; 37(3): 217 -229. doi: 10. 1002/ppul. 10438 6. Nicholson KJ, Nosanov LB, Bowen KA, et al. Thoracoscopic placement of phrenic nerve pacers for diaphragm pacing in congenital central hypoventilation syndrome. J Pediatr Surg. 2015; 50(1): 78 -81. doi: 10. 1016/j. jpedsurg. 2014. 10. 002 7. System information. Avery Biomedical Devices, Inc. website. http: //www. averybiome dical. com/diaphragm-pacing -systems/system-information/. Accessed November 25, 2017. 8. Basu SM, Bchir MB, Chung FF, Abdel. Hakim SF, Wong J. Anesthetic consideration for patients with congenital central hypoventilation syndrome: a systematic review of the literature. Anesth & Analg. 2017; 124(1): 169 -178. doi: 10. 1213. ANE. 0000001470 *Mythbusters logo property of Discovery Communications, LLC. Used for educational purposes only.
- Slides: 24