Pharmacology of drugs used in bronchial asthma COPD

Pharmacology of drugs used in bronchial asthma & COPD By Profs. Abdulqader Alhaider @ Hanan Hagar 1435 H

Disorders of Respiratory Function Main disorders of the respiratory system are : 1. Bronchial asthma 2. Cough 3. Allergic rhinitis 4. Chronic obstructive pulmonary disease (COPD, also called emphysema)

Asthma is a chronic inflammatory disorder of bronchial airways that result in airway obstruction in response to external stimuli (as pollen grains, cold air and tobacco smoke).

Characters of airways in asthmatic patients : Airway hyper-reactivity: abnormal sensitivity of the airways to wide range of external stimuli. Inflammation • Swelling • Thick mucus production. Bronchospasm (constriction of the bronchial muscles).

http: //link. brightcove. com/services/player/bcpid 236059233? bctid=347806802

Symptoms of asthma Asthma produces recurrent episodic attack of § Acute bronchoconstriction § Shortness of breath § Chest tightness § Wheezing § Rapid respiration § Cough Symptoms can happen each time the airways are irritated by inhaled irritants or allergens.

Causes § § § § Infection Emotional conditions Stress Exercise Pets Seasonal changes Some drugs as aspirin, β bockers
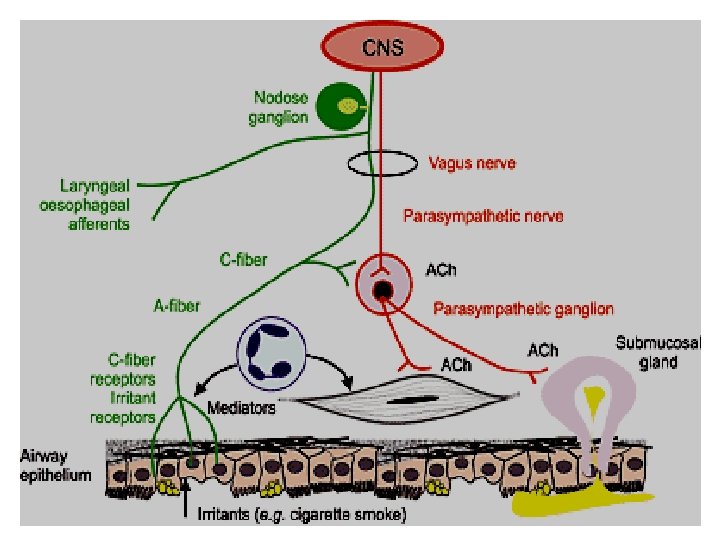
 Ø Irritant receptors in upper airways. Ø C-fiber receptors")
Airways Innervations Afferent nerves (sensory) Ø Irritant receptors in upper airways. Ø C-fiber receptors in lower airways. Stimulated by : Exogenous chemicals Physical stimuli (cold air) Endogenous inflammatory mediators
 Ø Parasympathetic supply M 3 receptors in smooth muscles and glands.")
Efferent nerves (motor) Ø Parasympathetic supply M 3 receptors in smooth muscles and glands. Ø No sympathetic supply but B 2 receptors in smooth muscles and glands

Aims of anti asthmatic drugs: • To relieve acute episodic attacks of asthma (bronchodilators, quick relief medications). • To reduce the frequency of attacks, and nocturnal awakenings (anti-inflammatory drugs, prophylactic or control therapy ).
 treat acute episodic attack of asthma •")
Anti asthmatic drugs Bronchodilators (Quick relief medications) treat acute episodic attack of asthma • • • Short acting 2 -agonists Antimuscarinics Xanthine preparations Anti-inflammatory Agents (control medications or prophylactic therapy) reduce the frequency of attacks • Corticosteroids • Mast cell stabilizers • Leukotrienes antagonists • Anti-Ig. E monoclonal antibody • Long acting ß 2 -agonists
 are used to relieve acute attack")
Anti asthmatic drugs Bronchodilators : (Quick relief medications) are used to relieve acute attack of bronchoconstriction 1. 2 - adrenoreceptor agonists 2. Antimuscarinics 3. Xanthine preparations

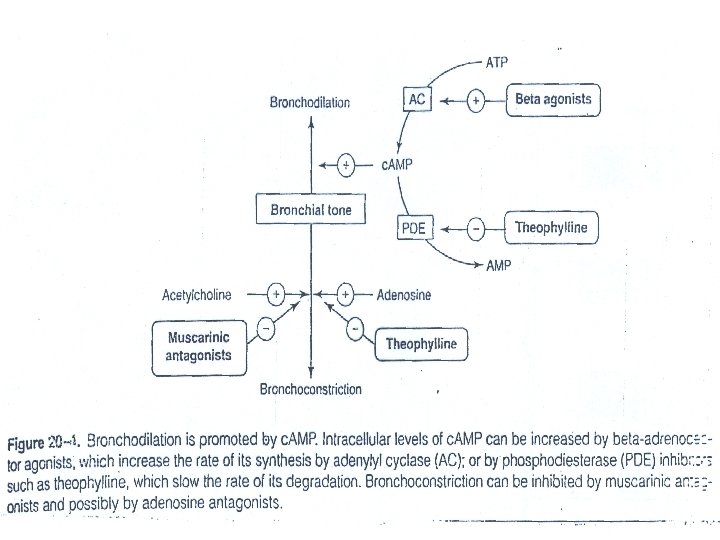
Sympathomimetics - adrenoceptor agonists Mechanism of Action Ø direct 2 stimulation stimulate adenyl cyclase Increase c. AMP bronchodilation Ø Inhibit mediators release from mast cells. Ø Increase mucus clearance by (increasing ciliary activity).

 Selective 2 –agonists")
Classification of agonists Ø Non selective agonists: Epinephrine – Isoprenaline (Obselete) Selective 2 –agonists (Preferable). Ø A. Short Acting Salbutamol (Albuterol) Terbutaline Ø B. Long Acting Salmeterol Formeterol

Non selective -agonists. Epinephrine • Potent bronchodilator • Rapid action (maximum effect within 15 min). • S. C. or by inhalation (aerosol or nebulizer). • Has short duration of action (60 -90 min) • Drug of choice for acute anaphylaxis (hypersensitivity reactions). • Note: Epinephrine good for both the hypotension and Bronchoconstriction.

Disadvantages Not effective orally. Ø Hyperglycemia Ø CVS side effects: tachycardia, arrhythmia, hypertension Ø Skeletal muscle tremor Ø Not suitable for asthmatic patients with hypertension or heart failure. Ø Contraindication: CVS patients, diabetic patients

Selective 2 –agonists Ø Ø Ø Drugs of choice for acute attack of asthma Are mainly given by inhalation (metered dose inhaler or nebulizer). Can be given orally, parenterally. Short acting ß 2 agonists e. g. Salbutamol (Ventoline. R), Terbutaline Long acting ß 2 agonists e. g. Salmeterol, Formeterol

Nebulizer Inhaler

Long acting selective ß 2 agonists Salmeterol & formoterol: Ø Long acting bronchodilators (12 hours) Ø have high lipid solubility (creates depot effect) Ø are given by inhalation Ø are not used to relieve acute episodes of asthma Ø used for nocturnal asthma (long acting relievers). Ø combined with inhaled corticosteroids to control asthma (decreases the number and severity of asthma attacks). Ø

Advantages of ß 2 agonists Ø Minimal CVS side effects Ø suitable for asthmatic patients with hypertension or heart failure. Disadvantages of ß 2 agonists Ø Skeletal muscle tremors. Ø Nervousness Ø Tolerance (ß -receptors down regulation). Ø Tachycardia over dose (ß 1 -stimulation).

Short acting ß 2 agonists Salbutamol, inhalation, orally, i. v. Terbutaline, inhalation, orally, s. c. Ø Have rapid onset of action (15 -30 min). Ø Short duration of action (4 -6 hr) Ø Used for symptomatic treatment of acute episodic attack of asthma.

Muscarinic antagonists Ipratropium – Tiotropium Ø Act by blocking muscarinic receptors. Ø Given by aerosol inhalation Ø Quaternary derivatives of atropine therefore, Does not diffuse into the blood and do not enter CNS, minimal systemic side effects. Ø Delayed onset of action Ø Ipratropium has short duration of action 3 -5 hr Ø Tiotropium has longer duration of action (24 h).
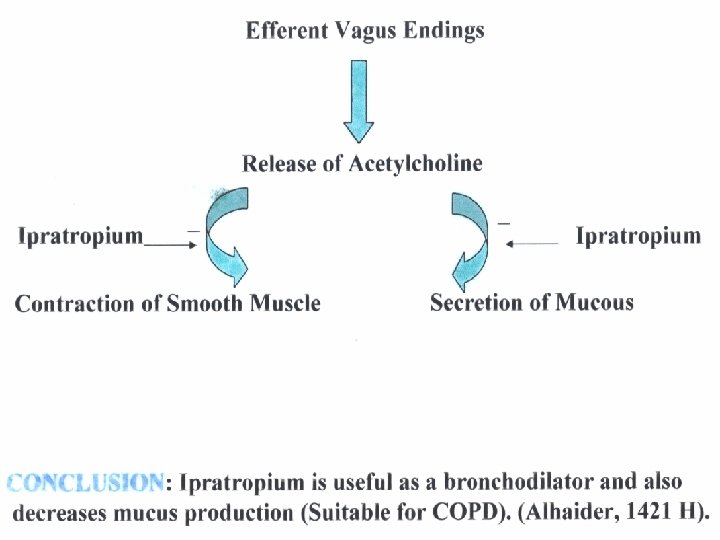

Pharmacodynamics Ø Ø Ø Inhibit bronchoconstriction and mucus secretion Less effective than β 2 -agonists. No anti-inflammatory action Uses Ø Ø Main choice in chronic obstructive pulmonary diseases (COPD). Why? In acute severe asthma combined with β 2 agonists & steroids.
. Mechanism of")
Methylxanthines Ø Theophylline – Aminophylline (theophyline with ethylenediamine in 2: 1 ratio). Mechanism of Action Ø are phosphodiestrase inhibitors Ø c. AMP bronchodilation Ø Universal Adenosine receptors antagonists (A 1) Ø Increase diaphragmatic contraction Ø Stabilization of mast cell membrane
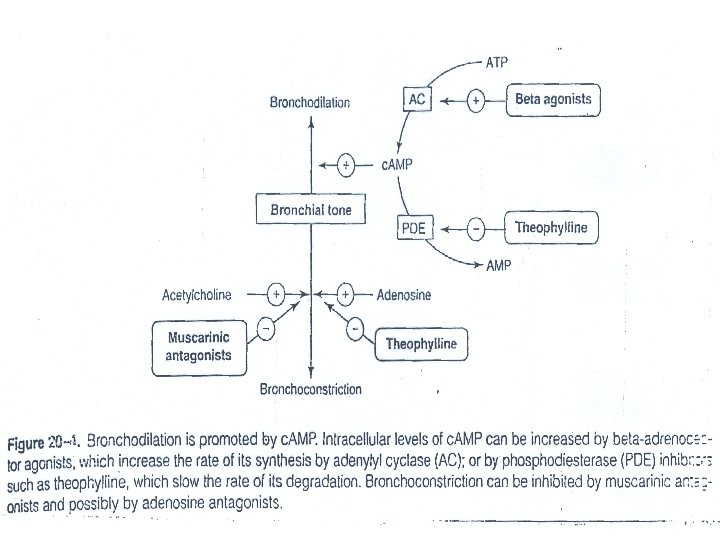

ATP Bronchodilation Adenyl cyclase B-agonists c. AMP Bronchial tree Adenosine Bronchoconstriction Phosphodiesterase Theophylline 3, 5, AMP

Pharmacological effects : ØBronchial muscle relaxation Ø contraction of diaphragm improve ventilation CVS: ↑ heart rate, ↑ force of contraction GIT: ↑ gastric acid secretions Kidney: ↑renal blood flow, weak diuretic action CNS stimulation * stimulant effect on respiratory center. * decrease fatigue & elevate mood. * overdose (tremors, nervousness, insomnia, convulsion)

Pharmacokinetics Ø metabolized by Cyt P 450 enzymes in liver ØT ½= 8 hours Øhas many drug interactions Ø Enzyme inducers: as phenobarbitone- rifampicin → ↑metabolism of theophylline → ↓ T ½. Ø Enzyme inhibitors: as erythromycin→ ↓ metabolism of theophylline → ↑T ½.
 Ø For status asthmatics (aminophylline, is")
Uses Ø Second line drug in asthma (theophylline) Ø For status asthmatics (aminophylline, is given as slow infusion). Why not theophylline? ) Side Effects Ø Low therapeutic index narrow safety margin monitoring of theophylline blood level is necessary. Ø CVS effects: hypotension, arrhythmia. Ø GIT effects: nausea & vomiting Ø CNS side effects: tremors, nervousness, insomnia, convulsion

2. Anti-inflammatory Drugs: • Since airway hypersensitivity is related the degree of inflammation; anti-inflammatory drugs are considered one of the most effective drugs in the treatment of chronic and acute types of asthma?
 reduce the number of inflammatory")
Anti - inflammatory Agents: (control medications / prophylactic therapy) reduce the number of inflammatory cells in the airways and prevent blood vessels from leaking fluid into the airway tissues. By reducing inflammation, they reduce the spasm of airways & bronchial hyper-reactivity.

Anti - inflammatory agents include: Glucocorticoids Ø Leukotrienes antagonists Ø Mast cell stabilizers Ø Anti-Ig. E monoclonal antibody (omalizumab) Ø

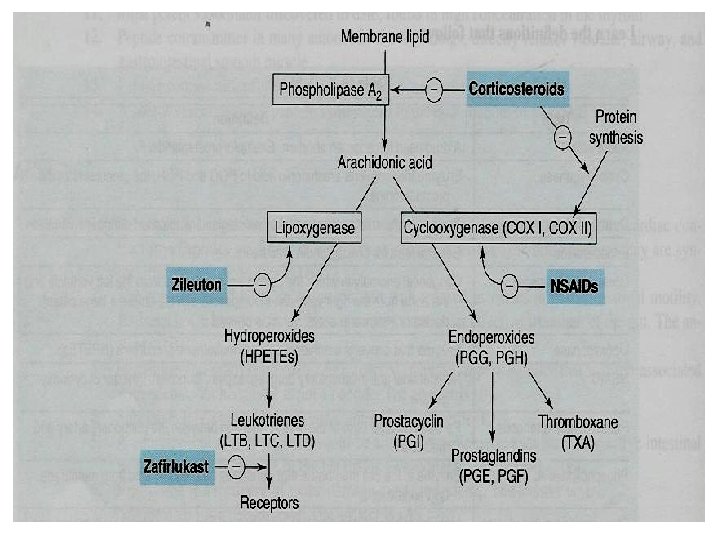
Glucocorticoids Mechanism of action Ø Ø Ø Inhibition of phospholipase A 2 therefore, ↓ prostaglandin and leukotrienes ↓ Number of inflammatory cells in airways. Mast cell stabilization →↓ histamine release. ↓ capillary permeability and mucosal edema. Inhibition of antigen-antibody reaction. Upregulate β 2 receptors (have additive effect to β 2 agonists).
 Immunosuppressant effects (useful")
Pharmacological actions of glucocorticoids Ø Ø Ø Anti-inflammatory actions (useful effects) Immunosuppressant effects (useful effects) Metabolic effects (Side Effects) – Hyperglycemia – ↑ protein catabolism, ↓ protein anabolism – Stimulation of lipolysis - fat redistribution Ø Mineralocorticoid effects (Aldosterone) – Sodium/fluid retention (hypertension) – Increase potassium excretion (hypokalemia) – Increase blood volume (hypertension)
 due to – Inhibit bone formation")
Ø Ø Behavioral changes: depression Bone loss (osteoporosis) due to – Inhibit bone formation – ↓ calcium absorption.

Routes of administration Inhalation: e. g. Budesonide & Fluticasone, Beclometasone – Given by inhalation, given by metered-dose Ø inhaler 0 – Best choice in asthma, less side effects Orally: Prednisone, methyl prednisolone Ø Injection: Hydrocortisone, dexamethasone (Note : Both have first pass metabolism) Ø

Glucocorticoids in asthma § Are not bronchodilators § Reduce bronchial inflammation § Reduce bronchial hyper-reactivity to stimuli § Have delayed onset of action (effect usually attained after 2 -4 weeks). § Maximum action at 9 -12 months. § Given as prophylactic medications, used alone or combined with beta-agonists. § Effective in allergic, exercise, antigen and irritant -induced asthma,
. Inhaled steroids should")
Systemic corticosteroids are reserved for: – Status asthmaticus (i. v. ). Inhaled steroids should be considered for adults, children with any of the following features • using inhaled β 2 agonists three times/week • symptomatic three times/ week or more; • or waking one night/week.
. 2. Treatment")
Clinical Uses of glucocorticoids 1. Treatment of inflammatory disorders (asthma, rheumatoid arthritis). 2. Treatment of autoimmune disorders (ulcerative colitis, psoriasis) and after organ or bone marrow transplantation. 3. Antiemetics in cancer chemotherapy

Side effects due to systemic corticosteroids – Adrenal suppression – Growth retardation in children – Osteoporosis – Fluid retention, weight gain, hypertension – Hyperglycemia – Susceptibility to infections – Glaucoma – Cataract – Fat distribution, wasting of the muscles – Psychosis
. – Dysphonia (voice hoarseness)")
Inhalation has very less side effects: – Oropharyngeal candidiasis (thrush). – Dysphonia (voice hoarseness) Withdrawal – Abrupt stop of oral corticosteroids should be avoided and dose should be tapered (adrenal insufficiency syndrome).
 - Nedocromil Ø act by stabilization of")
Mast cell stabilizers e. g. Cromolyn (cromoglycate) - Nedocromil Ø act by stabilization of mast cell membrane. Ø given by inhalation (aerosol, microfine powder, nebulizer). ØHave poor oral absorption (10%)

Pharmacodynamics § are Not bronchodilators § Not effective in acute attack of asthma. § Prophylactic anti-inflammatory drug § Reduce bronchial hyper-reactivity. § Effective in exercise, antigen and irritant-induced asthma. § Children respond better than adults

Uses Ø Ø Ø Prophylactic therapy in asthma especially in children. Allergic rhinitis. Conjunctivitis. Side effects Ø Ø Bitter taste Minor upper respiratory tract irritation (burning sensation, nasal congestion)

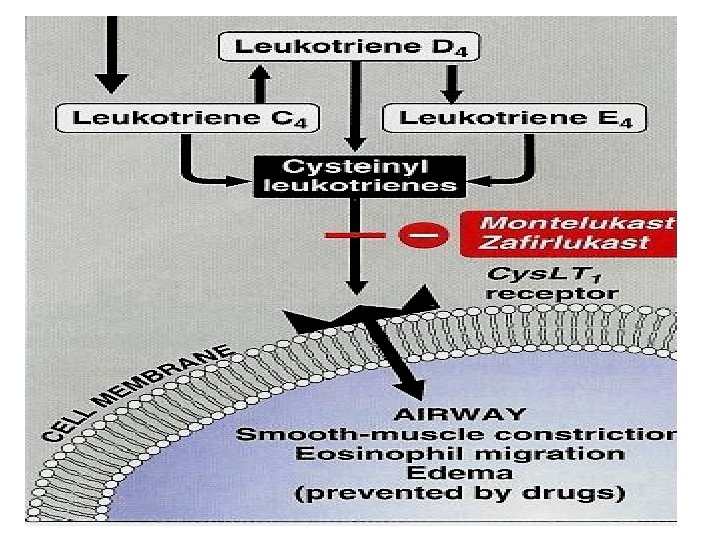
Leukotrienes antagonists Leukotrienes Ø produced by the action of 5 -lipoxygenase on arachidonic acid. Ø Synthesized by inflammatory cells found in the airways (eosinophils, macrophages, mast cells). Ø Leukotriene B 4: chemotaxis of neutrophils Ø Cysteinyl leukotrienes C 4, D 4 & E 4: – bronchoconstriction – increase bronchial hyper-reactivity – mucosal edema, mucus hyper-secretion
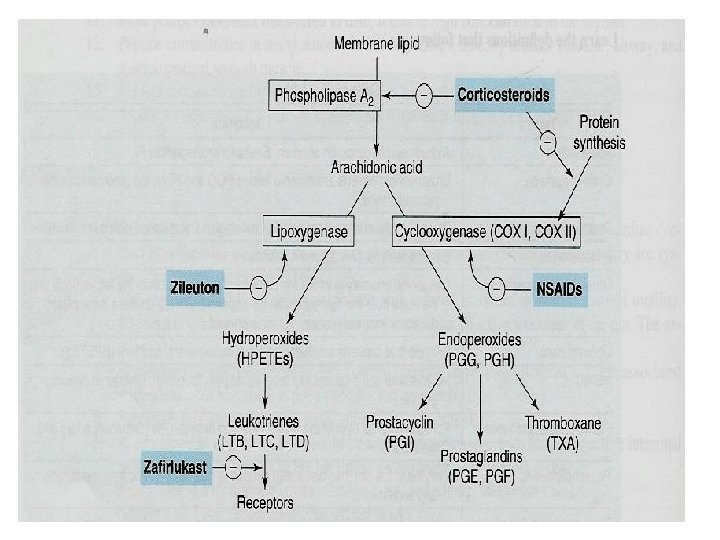

Leukotriene receptor antagonists e. g. Zafirlukast, Montelukast, Pranlukast Ø are selective, reversible antagonists of cysteinyl leukotriene receptors (Cys. LT 1 receptors). Ø Taken orally. Ø Are bronchodilators Ø Have anti-inflammatory action Ø Less effective than inhaled corticosteroids Ø Have glucocorticoids sparing effect (potentiate corticosteroid actions).

Uses of leukotriene receptor antagonists Are not effective to relieve acute attack of asthma. Ø Prophylaxis of mild to moderate asthma. Like: - Aspirin-induced asthma - Antigen and exercise-induced asthma Can be combined with glucocorticoids (additive effects, low dose of glucocorticoids can be used). Ø Side effects: Elevation of liver enzymes, headache, dyspepsia

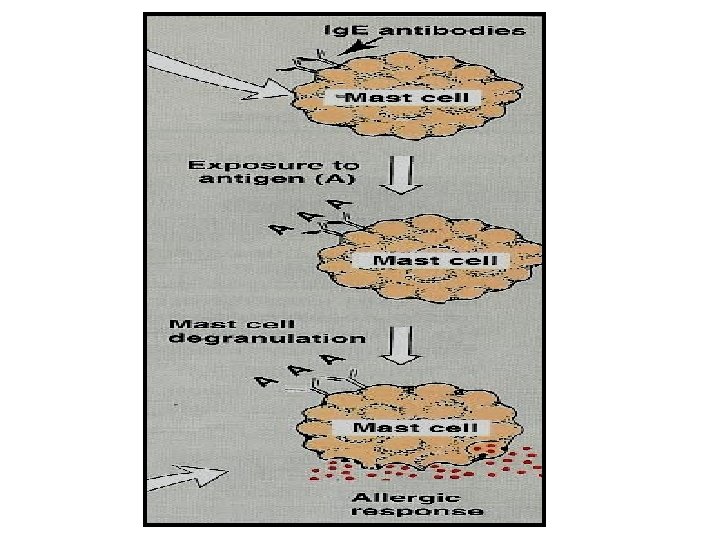
Omalizumab § is a monoclonal antibody directed against human Ig. E. § prevents Ig. E binding with its receptors on mast cells & basophiles. § ↓ release of allergic mediators. § used for treatment of allergic asthma. § Expensive-not first line therapy.
 MOA: • Selective anti-Ig. E monoclonal antibody that binds")
Anti-immunoglobulin E (e. g. Omalizumab) MOA: • Selective anti-Ig. E monoclonal antibody that binds to Ig. E and prevents its association with Ig. E receptors, thus preventing allergen from activating mast cells or basophiles • Decreases serum Ig. E • Due to the above effects, omalizumab decreases the numbers of eosinophils, T and B lymphocytes • Uses: for resistance type of asthma and allergic rhinitis. • Side effects and Limitations: – Infusion side effects and very expensive.

Drugs used in COPD • COPD is a chronic irreversible airflow obstruction, lung damage and inflammation of the air sacs (alveoli). • Smoking is a high risk factor • Treatment: – Inhaled bronchodilators – Inhaled glucocorticoids – Oxygen therapy

– Antibiotics specifically macrolides such as azithromycin to reduce the number of exacerbations. – Lung transplantation

Treatment of COPD Inhaled bronchodilators Ø Inhaled antimuscarinics (are superior to β 2 agonists in COPD) Ø β 2 agonists Ø these drugs can be used either alone or combined – salbutamol + ipratropium – salmeterol + Tiotropium (long acting-less dose frequency).
 Antimuscarenic drugs like Ipratropium is")
Does treatment of COPD differs from bronchial Asthma? 1) Antimuscarenic drugs like Ipratropium is preferred for COPD Why? 2) Short acting b 2 -adrenergic agonist is used like for Asthma. 3) However, oral or inhaled corticosteriods are only used for severe form of COPD. Why? 4) Mucolytics like Acetylcysteine may be used. 5) Routine administration of Oxygen may be included for advanced cases.

Summary
 Drugs B 2 agonists Salbutamol, terbutaline Salmeterol, formoterol Antimuscarinics Ipratropium")
Bronchodilators (relievers for bronchospasm) Drugs B 2 agonists Salbutamol, terbutaline Salmeterol, formoterol Antimuscarinics Ipratropium (Short) Tiotropium (long) Xanthine derivatives Theophylline Aminophylline – Short acting – main choice in acute attack of asthma – Inhalation Long acting, Prophylaxis Nocturnal asthma Main drugs For COPD Inhalation (orally) (parenterally) denyl A cyclase c. AMP Blocks M receprtors • Inhibits phosphodi esterase c. AMP
 Corticosteroids (Inhibits phospholipase A 2) Dexamethasone, Fluticasone, budesonide prednisolone Hydrocortisone Mast")
Anti-inflammatory drugs (prophylactic) Corticosteroids (Inhibits phospholipase A 2) Dexamethasone, Fluticasone, budesonide prednisolone Hydrocortisone Mast stabilizers Cromoglycate (Cromolyn), Nedocromil Inhalation Orally parenterally Inhalation, prophylaxis in children Cysteinyl antagonists (Cy. LT 1 antagoist) Zafirlukast orally Omalizumab (Anti Ig. E antibody) Injection, SC
- Slides: 64