Pharmacology DENTALELLE TUTORING WHAT ARE AUTACOIDS OCCUR NATURALLY










 Ø Act primarily at the: peripheral nerve")

")


.")

 to block production of")
























 –")



 • used in PREVENTION of a gout")






 and Hydrocodone (in Vicodin) are some of the weakest")
 COMMENTS SCHEDULE FOR CONTROLLE D SUBSTANCE STRONGEST MORPHINE MERPERIDENE (Demerol)")

")

, INCLUDE: ENKEPHALINS ENDORPHINS DYNORPHINS")







? TRUE OR FALSE?")










 Not a problem with usual doses in normal patients")






")



















 or")








 v. Naloxone will block therapeutic and toxic actions of")

 AN ORALLY ADMINISTERED NON-OPIOID WITH WEAK ANALGESIC ACTIVITY")
 v. Few studies have confirmed its efficacy: v Binds with")





- Slides: 123
Pharmacology DENTALELLE TUTORING
WHAT ARE AUTACOIDS?
OCCUR NATURALLY IN THE BODY PRODUCED IN ONE ORGAN AND ARE TRANSPORTED VIA THE LYMPH SYSTEM ALL OCCUR (MADE) NATURALLY IN THE BODY. • •
Terms & Definitions Autacoids - Examples: Prostaglandins – lipids that are synthesized locally by inflammatory stimuli –↑↑ PAIN receptors Thromboxanes (a vasoconstrictor and a potent hypertensive agent, and facilitates platelet aggregation [clotting]). Leukotrienes (Inflammatory molecules; precursor of prostaglandins) “-kinins” - messengers
IS PAIN DIFFERENT FOR EVERYONE?
YES
WHAT ARE PLACEBOS?
‘’FAKE’ DRUGS FOR SOME PEOPLE, PAIN CAN ALSO BE EFFECTIVELY TREATED WITH INACTIVE PILLS (PLACEBOS)
WHAT ARE ANTIPYRETICS ALSO CALLED?
NON-OPIODS NON OPIOID ANALGESICS ARE ALSO CALLED: NONNARCOTIC, PERIPHERAL, MILD, AND ANTIPYRETIC (AGENTS THAT REDUCE FEVER) OPIOID ANALGESICS ARE ALSO CALLED: NARCOTIC, CENTRAL, OR STRONG ANALGESICS.
Classification of Analgesic Agents 1. Nonopioids (nonnarcotics) Ø Act primarily at the: peripheral nerve endings Difference is in their site of action Ø Inhibit prostaglandin synthesis (regulating the contraction and relaxation of smooth muscle tissue) Difference in their 2. Opioids (narcotics) ØAct primarily within the: central nervous system ØDepress the central nervous system mode of action Ø Not effective for severe pain ØEffective Ø 3 subgroups: • Salicylates (aspirin-like group) • NSAIDs • Acetaminophen pain for severe ØExamples: Morphine, Codeine, Agents in cough suppressants ØWe will discuss this area more in the next chapter
WHAT CATEGORY IS ASPIRIN UNDER?
SALICYLATES ASPIRIN IS THE MOST USEFUL AND COMMON SALICYLATE TO REDUCE PAIN (ANALGESIC ACTION) ACETYL SALICYLIC ACID (ASA) – THE CHEMICAL NAME FOR ASPIRIN
WHAT DOES NSAIDS STAND FOR AND WHAT DOES IT MEEAN?
NONSTEROIDAL ANTIINFLAMMATORY DRUGS
Salicylates • Aspirin belongs to a class of medications called nonsteroidal antiinflammatory drugs (NSAIDs). NSAIDs – Aspirin and other NSAIDs, for example, ibuprofen (eg. Motrin, Advil) and naproxen (eg. Aleve), are widely used to treat fever (antipyretic action), pain (analgesic action), and inflammatory (antiinflammatory action) conditions such as arthritis – Aspirin is also known for its anti-platelet action
Salicylates: ASA MECHANISM OF ACTION • Aspirin have: Whereas, Acetaminophen – anti-inflammatory, drugs have only – antipyretic, antipyretic & analgesic – analgesic, and actions. – antiplatelet actions. • These actions are related to the ability to inhibit prostaglandin synthesis
Salicylates: ASA MECHANISM OF ACTION • Aspirin inhibits cyclo-oxy-genase (COX) to block production of prostaglandins • Prostaglandins can sensitize pain receptors to substances such as BRADYKININ (SEE NOTE) – A reduction in prostaglandins results in a reduction in pain
HOW LONG BEFORE ASPIRINS PEAK EFFECT?
30 MINUTES REMEMBER NOT TO APPLY TOPICALLY TO ORAL MUCOSA!!!!
Salicylates: ASA ADVERSE REACTIONS 3. Reye’s Syndrome • Associated with use of aspirin in children & adolescents who took it when they had the chickenpox or influenza • Fatal disease that causes numerous detrimental effects to many organs, especially the brain and liver. • ACETAMINOPHEN and NSAIDs are now used for fever (antipyretic action) or pain (analgesic action) in pediatric and adolescents to reduce the chances of Reye’s Syndrome
WHAT DRUG SHOULD YOU NOT TAKE WITH ASPIRIN?
WARFARIN A DRUG INTERACTION BETWEEN ASPIRIN AND WARFARIN CAN RESULT IN SIGNIFICANT BLEEDING
NSAIDs • A rapidly growing group with important application in dentistry – Mechanism of action and many of their pharmacologic effects and adverse reactions resemble aspirin • Many authors agree that the NSAIDs are the most useful drug group for the treatment of dental pain. – Most are available without a prescription.
WHEN IS THE PEAK PERIOD FOR MOST NSAIDS?
1 -2 hours
NSAIDs PHARMACOKINETICS • Most NSAIDs peak in about 1 -2 hours – Well absorbed orally and food reduces the rate but not the extent of absorption • Metabolized in liver, excreted in kidneys
NSAIDs PHARMACOLOGIC EFFECTS • have a significant anti-inflammatory effect • Similar as aspirin: – analgesic – antipyretic – anti-inflammatory • They inhibit prostaglandin synthesis
ARE NSAIDS ADDICTING?
NO! NSAIDS ARE NOT ADDICTING, TOLERANCE DOES NOT DEVELOP, AND NO WITHDRAWAL SYNDROME CAN BE INDUCED.
NSAIDs ADVERSE REACTIONS 7. Pregnancy and Nursing • Contraindicated in pregnancy; • Like aspirin, NSAIDs given late in pregnancy can prolong gestation • IBUPROFEN is drug of choice for nursing
DENTAL PAIN IS BEST MANAGED BY HOW MUCH MG OF IBUPROFEN?
400 MG IN USUAL PRESCRIPTION DOSES, NSAIDS CAN BE SHOWN TO BE STATISTICALLY SIGNIFICANTLY BETTER THAN CODEINE ALONE, ASPIRIN, ACETAMINOPHEN, OR PLACEBO.
NSAIDs CONTRAINDICATIONS & CAUTIONS • NSAIDs should be used with caution in patients with: Contraindicated in 1. asthma pregnancy 2. cardiovascular disease 3. Renal diseases with fluid retention 4. coagulation problems 5. peptic ulcer disease 6. ulcerative colitis
WHAT IS THE MOST COMMONLY USED NSAID?
IBUPROFEN
WHAT HAS NO ANTIINFLAMMATORY EFFECT?
ACETAMINOPHEN
Acetaminophen • Used as an analgesic and antipyretic in children and adults when aspirin is contraindicated • Has no anti-inflammatory action
Acetaminophen PHARMACOKINETICS • Rapidly and completely absorbed from the GI tract • Peak plasma level in 1 – 3 hours • Half life of 1 to 4 hours • Metabolized by the liver • Excreted by the kidneys in 24 hours • When large doses are ingested, an intermediate metabolite is produced that is thought to be hepatotoxic and possibly nephrotoxic.
AN ACUTE OVERDOSE OF ACETAMINOPHEN CAUSE WHAT?
LIVER DAMAGE
Acetaminophen USES • Acetaminophen is used as an: – Analgesic agent (↓ pain) – Antipyretic agent (↓ fever)
Acetaminophen USES • Used when hypersensitivity to aspirin or for patients experiencing aspirin-gastric induced irritation. • Used as an antipyretic instead of aspirin for young children; children due to aspirin’s association with Reye’s syndrome. • Can be used in all stages of pregnancy (always ask doctor)
WHAT DRUGS ARE USED TO TREAT GOUT?
Allopurinol AND Probenecid
Drugs Used to Treat Gout Allopurinol (Zyloprim) • used in PREVENTION of a gout attack. – Inhibits the synthesis of uric acid – Also used in patients receiving either chemotherapy or irradiation – If a pruritic rash should occur, the drug should be promptly discontinued Probenecid (Benemid) • used in PREVENTION of a gout attack. – Is an uricosuric drug that increases uric acid excretion in the urine
CHAPTER 6
WHAT ARE OPIODS USED TO TREAT?
MODERATE TO SEVERE PAIN AT FIRST REFERRED TO DRUGS THAT ARE DERIVATIVES OF OPIUM POPPY OPIOID OR NARCOTIC ANALGESICS ARE USED TO MANAGE DENTAL PAIN IN PATIENTS IN WHOM NSAIDS ARE CONTRAINDICATED
CLASSIFICATION -THREE GROUPS 1. Mechanism of action at the receptor site: site GROUP SUBGROUP EXAMPLE Ø OPIOID AGONISTS Ø MIXED OPIOIDS morphine, codeine pentazocine Ø AGONISTANTAGONISTS Ø PARTIAL buprenorphine AGONIST Ø ANTAGONISTS Naloxone 53
CLASSIFICATION: CHEMICAL STRUCTURE BOX 6 -1 OPIOD ANALGESIC AGENTS BY STRUCTURE GROUP MORPHINE AND CODEINE (Largest Group) • • hydromorphone (Dilaudid) agonist hydrocodone (in Vicodin) agonist dihydrocodeine (in Synalgos-DC) oxycodone (in Percodan, Percocet, Tylox) agonist METHADONE • • methadone (Dolophine) agonist propoxyphene (Darvon) agonist MORPHINAN • • butorphanol (Stadol) agonist-antagonist pentazocine (in Talwin-NX) agonist-antagonist MEPERIDINE • • • meperidine (Demerol) agonist fentanyl (Sublimaze) agonist diphenoxylate (in Lomotil) OTHER • buprenorphine (Buprenex, Subutex) partial agonist Do not give any of these drugs if the patient has an allergy to morphine or codeine 54
WHAT ARE WEAKER FORMS OF OPIODS?
Codeine (in Tylenol#3) and Hydrocodone (in Vicodin) are some of the weakest
DRUG NAME (SOME EXAMPLES) COMMENTS SCHEDULE FOR CONTROLLE D SUBSTANCE STRONGEST MORPHINE MERPERIDENE (Demerol) Standard agent; prototype II Abused by professionals II INTERMEDIATE OXYCODONE (in Percocet) Popular with addicts ‘shopping’ for opioids II WEAKEST HYDROCODONE (in Vicodin) 57 CODEINE (in Tylenol#3) III #2=15 mg; #3 -30 mg; #4=60 mg III
WHERE DO NONOPIODS ACT?
PERIPHERAL NERVE ENDINGS OPIOIDS BIND TO RECEPTORS IN BOTH THE CENTRAL NERVOUS SYSTEM (CNS) AND THE SPINAL CORD, PRODUCING AN ALTERED PERCEPTION OF REACTION TO PAIN
WHAT ARE NATURAL OPIODS?
RELIEVE PAIN AND RELAXATION NATURAL OPIOIDS (ALSO CALLED ENDOGENOUS OPIOIDS), INCLUDE: ENKEPHALINS ENDORPHINS DYNORPHINS THESE ARE THE CHEMICALS THAT MAKE SURE WE CAN FUNCTION DURING ACCIDENTS, LIKE AFTER BREAKING OUR LEG…
MECHANISM OF ACTION The Discovery of 3 Groups of Endogenous Substances Enkephalins stimulates delta( ) receptor 2. Endorphins reduces pain & positively affects mood. 3. Dynorphins stimulates the kappa ( )receptor 1. v. All 62 Probably function as neurotransmitters, although their exact function has not been elucidated. 3 have opioid-like action and are found in the body. v. They are naturally occurring peptides that possess analgesic action and addiction potential
WHEN DO OPIODS START WORKING?
WITHIN 1 HOUR THE DOSING INTERVALS OF MOST OPIOIDS ARE BETWEEN 4 -6 HOURS; THE USUAL DOSE DEPENDS ON THE DRUG. DURATION – NECESSITATES DOSING EVERY 4 -6 HOURS
WHAT IS THE FIRST PASS EFFECT?
REDUCES THE BIOAVAILABILITY UNDERGOES FIRST PASS METABOLISM IN THE LIVER AND INTESTINE, REDUCING ITS BIOAVAILABILITY.
PHARMACOKINETICS v. Distribution: v. Oral bioavailability of opioids is primarily limited by first pass metabolism. v. Undergoes first pass metabolism in the liver and intestine, reducing its bioavailability. v. Degree of first pass differs among individuals. v. May cause respiratory depression in fetus when mother is given opioids near term. 67
PHARMACOKINETICS A. D. M. E v. Excretion: v. Most opioids are excreted through the kidneys, but this action does not selectively affect their availability after oral administration. Metabolized opioids and the unchanged drug are excreted in the urine. 68
severity of side effects is proportional to the efficacy (strength)? TRUE OR FALSE?
TRUE A PHARMACOLOGIC EFFECT MAY ALSO BE AN ADVERSE REACTION, DEPENDING ON THE CLINICAL USE OF THE AGENT.
IS MORPHINE THE STRONGEST OR WEAKEST OPIOD?
THE STRONGEST • MORPHINE IS THE OPIOID AGONIST BY WHICH ALL OTHERS ARE MEASURED. STRONGEST CAN RELIEVE SEVERE PAIN WHILE WEAKER AGENTS MIXED WITH NONOPIOIDS ARE EQUIVALENT TO NSAIDS. •
PHARMACOLOGIC EFFECTS Analgesia What do aspirin, acetaminophen, ibuprofen, and codeine have in common? ØAspirin (ASA) and ibuprofen (NSAID) are analgesic, analgesic antipyretic, and antiinflammatory, and they inhibit platelet aggregation. Ø Acetaminophen is analgesic and antipyretic. ØCodeine is analgesic. 73
WHAT IS AN ANTITUSSIVE?
SUPRESSES A COUGH DEXTROMETHORPHAN
PHARMACOLOGIC EFFECTS Gastrointestinal Effects ØOpioid analgesics ↑ smooth muscle tone and ↓ propulsive contractions and motility (some opioids have constipation as a side effect). ØUseful for treating diarrhea. Opioids are not used for depression, infections, or hypertension ØExample: diphenoxylate (in Lomotil) 76
ADVERSE REACTIONS TRUE or FALSE Combining an opioid with a nonopioid analgesic produces an additive analgesic effect with fewer adverse reactions. TRUE These agents work at two different levels on pain and produce an additive analgesic effect. In combination products, lower doses of each analgesic may be used, and a potential exists for a reduction in adverse reactions. 77
DO OPIODS INCREASE OR DEPRESS THE RESPIRATORY CENTRE?
DEPRESS THE RESPIRATORY CENTER IN A DOSE RELATED MANNER THE RATE AND DEPTH OF BREATHING ARE REDUCED. THE DEPRESSION IS RELATED TO A DECREASE IN THE SENSITIVITY OF THE BRAINSTEM TO CARBON DIOXIDE.
ADVERSE REACTIONS Respiratory Depression (RP) Not a problem with usual doses in normal patients 80 RP is usually the cause of death with an overdose
ADVERSE REACTIONS Nausea and Emesis v. Analgesic doses of opioids often produce nausea and vomiting. v. Result of their direct stimulation of the chemoreceptor trigger zone (CTZ) located in the medulla. v. Repeated administration of regular doses can prevent vomiting at the vomiting center (VC). 81
WHAT IS A VERY COMMON SIDE EFFECT OF OPIOD USE?
CONSTIPATION THEIR DURATION OUTLASTS THEIR ANALGESIC EFFECT
WHAT IS A SIGN IN RECOGNIZING AN OPIOD ADDICT?
MIOSIS – ‘PINPOINT PUPILS’. RESPIRATORY DEPRESSION
HOW DO YOU TREAT AN OVERDOSE TO OPIODS?
AN ANTAGONIST SUCH AS NALOXONE (IN NARCAN)
ADVERSE REACTIONS Biliary Tract Constriction v. Opioids may constrict the biliary duct, causing biliary colic (bile duct obstruction leading to gall stones). v. Importance in patients passing gallstones who are being treated with opioids. 88
A MOTHER ON OPIODS – WHAT CAN HAPPEN TO THE BABY?
THE INFANT MAY HAVE DEPRESSED RESPIRATION AND WITHDRAWL SYMPTOMS NOT TERATOGENIC, BUT MAY PROLONG LABOR OR DEPRESS FETAL RESPIRATION IF GIVEN NEAR TERM. . NOT USUALLY A PROBLEM WITH MOTHER’S MILK WITH THERAPEUTIC DOSES.
Use of opioids is NOT contraindicate d in hypertensive patients.
ADVERSE REACTIONS Addiction v. The degree of addiction potential is proportional to analgesic strength. v. An addict will develop tolerance to the effects of opioids, EXCEPT for miosis and constipation. 92
ADVERSE REACTIONS Addiction v. Since the duration of use in dentistry is usually short – addiction for dentistry does not pose a problem v. NSAIDs should be used to control dental pain in the addict. AN ADVANTAGE OF NSAIDs OVER OPIOIDS: NSAIDs are not addictive, tolerance does not develop, and no withdrawal syndrome can be induced. 93
IF A CLIENT CLAIMS ALLERGIES TO NSAIDS, WHAT COULD THIS MEAN?
OPIOD ADDICT TERMED ‘SHOPPERS’ THE CLIENT IS LOOKING FOR A SPECIFIC OPIOD. KEEP IN MIND – THIS ISNT ALWAYS THE CASE…LOOK FOR OTHER SIGNS NOT JUST ONE
ADVERSE REACTIONS v. The Addiction: Identification of an Addict “shoppers” - What to look for: v Asks for the opioid analgesic by name and says that this is the only drug that works for them. v Claims allergies to NSAIDs. v Cancels dental appointment but still requests the opioid analgesic even though they will be “out of town on business”. v Experiences pain for days after scaling and root planing v Moves from office to office because “others don’t understand”. v Claims a “low pain threshold”. v Needs refills several days after a procedure without complications. v Calls with a request for an opioid analgesic just as the office is closing or after hours. 96
WHAT IS METHADONE?
USED TO TREAT OPIOD ADDICTION AND WITHDRAWL MAINTAINING PATIENTS ON HIGH DOSES OF METHADONE (METHADONE MAINTENANCE).
ADVERSE REACTIONS Addiction: 4 Treatment Options v. Addiction, overdose, and withdrawal can be treated with opioid antagonists 1. 2. 3. 4. 99 Substituting addict with oral opioid (methadone). methadone Going cold turkey and using medication such as phenothiazines, clonidine or benzodiazepines (to alleviate symptoms of withdrawal). Maintaining patients on high doses of methadone (methadone maintenance). Administering an orally effective, long-acting antagonist Naltrexone (Trexan).
ADVERSE REACTIONS Addiction: Treatment Options Example: The Heroin Addict v. The following drugs can be used to treat heroin addiction ØMETHADONE, METHADONE is used by substituting methadone for heroin and then tapering off or maintaining the addict on oral methadone. ØNALTREXONE, NALTREXONE a long-acting opioid antagonist, is used to block the action of usual doses of opioid administered illegally 100
IS TRUE OPIOD ALLERGY COMMON?
NO MOST COMMON TYPES OF TRUE ALLERGIC REACTIONS TO OPIOIDS IS DERMATOLOGIC IN NATURE. DUE TO THE HISTAMINE-RELEASING PROPERTIES OF OPIOID ANALGESICS. INCLUDES SKIN RASHES AND URTICARIA. GI SIDE EFFECTS ARE OFTEN REPORTED.
This includes: A patient with a true allergy to codeine should NOT be given an analgesic in that group 103 Ø oxycodone Ø hydromorphone, Ø hydrocodone, and Ø dihydrocodone Because they are all members of the same morphine and codeine group.
WHAT IS THE PROTOTYPE OPIOD AGONIST WHICH OTHER OPIODS ARE MEASURED?
MORPHINE
SPECIFIC OPIODS Agonists: Morphine v. The prototype opioid agonist which other opioids are measured v. Parenterally: used to control postoperative pain v. Orally: 107 used primarily in the treatment of cancer
SPECIFIC OPIODS Agonists: Oxycodone v. Used alone or combined with aspirin (in Percodan) or acetaminophen (in Percocet, Tylox) with fewer adverse reactions. v. For v. It moderate to severe pain. is located in the middle of the chart for strength value. 108
SPECIFIC OPIODS Agonists: Hydrocodone v. Weak opioid analgesic with fewer adverse reactions. v Less potential for abuse. v Combination of Hydrocodone (5 mg) with acetaminophen (500 mg) is recommended for the majority of dental patients with pain v. In Vicodin, it has been reported as being safe to use when breastfeeding 109
WHAT IS THE MOST COMMON OPIOD IN DENTISTRY?
CODEINE MOST COMMONLY USED OPIOID IN DENTISTRY AND IS OFTEN COMBINED WITH ACETAMINOPHEN (TYLENOL #3) FOR ORAL ADMINISTRATION
Agonists: Meperidine SPECIFIC OPIODS v. Favorite drug of abuse for medical personnel; 100 mg meperidine=10 mg morphine. v. For acute management of moderate to severe pain. v. Poor choice for oral use because it has a high first pass effect; short duration of action. v. Less constipating, and without miosis or cough suppression. v. EXAMPLE: 112 meperidine HCl (Demerol)
WHAT IS HYDROMORPHINE USED FOR?
MANAGEMENT OF SEVERE PAIN, MORE POTENT THEN MORPHINE
Agonists: Hydromorphone SPECIFIC OPIODS v. An orally effective opioid, reserved for management of severe pain. v. More potent than morphine v. Similar adverse reactions to morphine. v. Favourite of the addicts because of its high strength; requires careful monitoring. v. EXAMPLE: Dilaudid 115
SPECIFIC OPIODS Slower onset and longer duration of action. Similar to morphine. EXAMPLE: Dolophine Used primarily to treat any opioid addicts (eg. Heroin addicts) 116 Agonists: Methadone is used either to withdraw the patient gradually or for methadone maintenance. Because it has a longer duration of action, withdrawal from methadone is easier than from heroin. Because it is an opioid analgesic, however, the risk for dependence still exists.
SPECIFIC OPIODS Antagonists naloxone (Narcan) v. Naloxone will block therapeutic and toxic actions of opioids v Methadone is an opioid used in treatment of addiction, but will exacerbate symptoms of an opioid overdose. v. An pure opioid antagonist that is active parenterally. v. Drug of choice for treating agonist or mixed opioid overdoses. 117
WHAT IS TRAMADOL?
(ULTRAM) AN ORALLY ADMINISTERED NON-OPIOID WITH WEAK ANALGESIC ACTIVITY
SPECIFIC OPIODS Tramadol (Ultram) v. Few studies have confirmed its efficacy: v Binds with mu (μ) opioid receptors; inhibits reuptake of serotonin and norepinephrine, and modifies ascending pain pathways. v. Its analgesic efficacy is equivalent to that of codeine. v. Side effects can include: miosis and CNS effects, such as dizziness, headache and stimulation and GI tract effects include nausea, diarrhea, constipation and vomiting. v. Is moving up the top 200 most prescribed drugs. 120
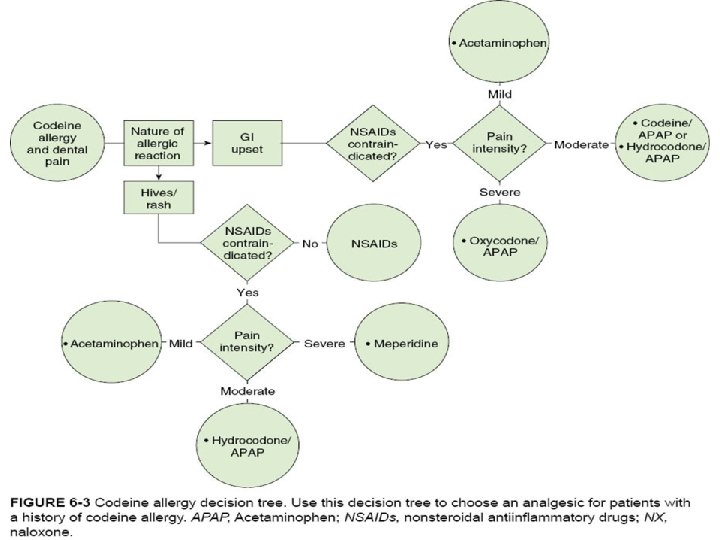
DENTAL USE OF OPIODS v. Most dental pain can be managed with NSAIDs. v. If NSAIDs are contraindicated - the DDS has a wide variety of opioids to choose from. v. Eg. Beginning with codeine or hydrocodone combinations, and progressing to oxycodone combinations. v. Only in rare cases and for short periods of time (approx. 1 -2 days) should stronger opioids be prescribed for outpatient dental pain. 121
ARE OPIODS USED FOR CHRONIC OR ACUTE PAIN?
ACUTE IS PREFERRED* BUT CAN BE USED FOR CHRONIC PAIN
REVIEW: USE OF OPIODS v. Opioids for: are considered first-line therapy v. Pain associated with procedures (bone marrow biopsy) v. Pain due to trauma or cancer (burns) v. Visceral pain (appendicitis) v. Majority used to relieve acute or chronic pain. v. Few, such as fentanyl (Sublimaze, Duragesic), alfentanil (Alfenta), and sufentanil (Sufenta), are primarily indicated for preoperative sedation to reduce patient apprehension. v. Also used to suppress cough and treat diarrhea 124
Some of the Opioids found in the TOP 200 Ø#1. Hydrocodone Ø#32. Tramadol Ø#105. Oxycodone Ø#133. Oxy. Contin Ø#156. Fentanyl transdermal Ø#175. Methadone HCl noninjectable 125