Pharmacological therapies in fibromyalgia R 3 Guo Shulin

Pharmacological therapies in fibromyalgia R 3 Guo, Shu-lin 92. 08. 18
 • Common, chronic, widespread pain syndrome • Predominantly middle-aged")
Introduction • Fibromyalgia syndrome (FMS) • Common, chronic, widespread pain syndrome • Predominantly middle-aged women • Philosophy of management • Symptom palliation • Functional restoration
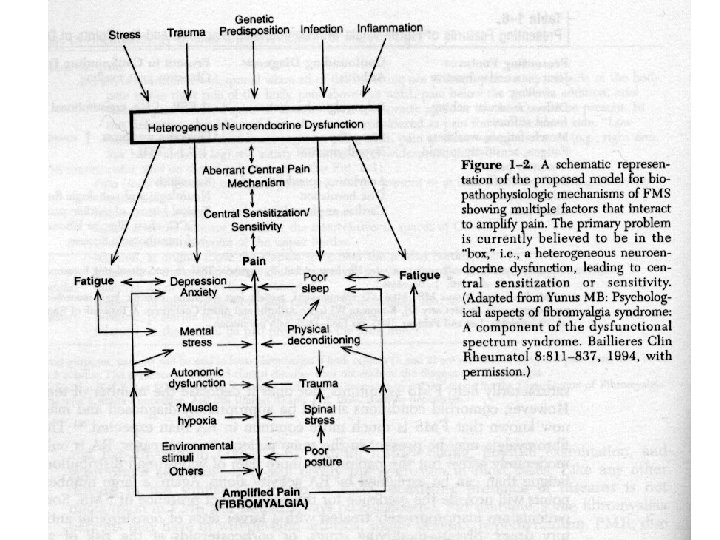

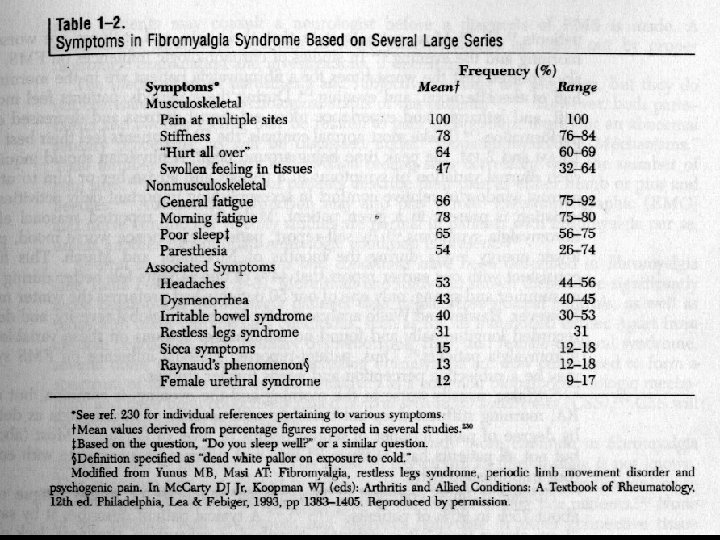
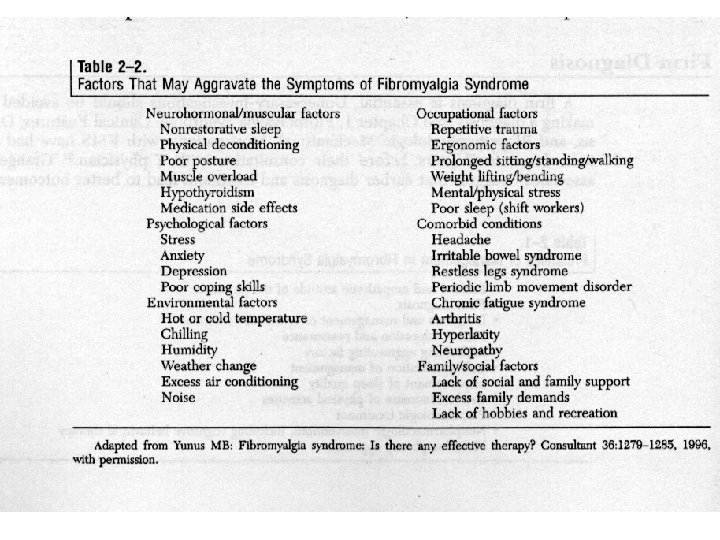
Symptoms and comorbid syndromes • Quantitative abnormalities in pain perception • the form of both allodynia and hyperalgesia • A lot of complaints beyond pain • Table. 1
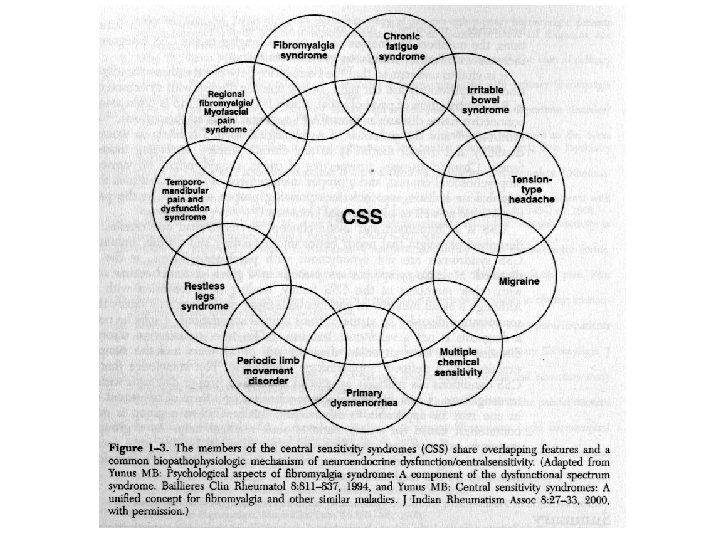
 =? Functional somatic syndromes (FSS) Table. 2")
Symptoms and comorbid syndromes • Fibromyalgia (FMS) =? Functional somatic syndromes (FSS) Table. 2 • FSS includes • • • Irritable bowel syndrome (IBS) Chronic low-back pain (CLBP) Tempomandiblular disordoer (TMD) Chronic fatigue syndrome (CFS) Interstitial cystitis (IC) Multiple chemical sensitivity (MCS)

Irritable bowel syndrome • A common disease includes abdominal pain, bloating, and disturbed defecation • The prevalence of IBS is between 823% in general population • Three subtypes of IBS are recognized as diarrhea, constipation and discomfort/pain predominant

Chronic low back pain • Up to 70% of adults have at least one episode of back pain during the course of their lifetime • CLBP defines as pain persisting beyond 3 months

Temporomandibular joint disoroders • A cluster of common chronic orofacial pain syndromes of unknown etiology • Classified into three groups as myofascial, joint disorder and combined

Chronic tension-type headaches • CTTH are defined by the presence of bilateral headaches that are mild to moderate in intensity, occurring more than 15 days per month for more than 6 months • Associated symptoms include nausea, photophobia and phonophobia

Psychological distress • Approximately 20 -30% of FMS patients have significant current major depressive disorder and about 60% have a lifetime prevalence of depressive illness • Post-traumatic stress disorders and other anxiety disorders may also represent an important cause of psychological distress in fibromyalgia

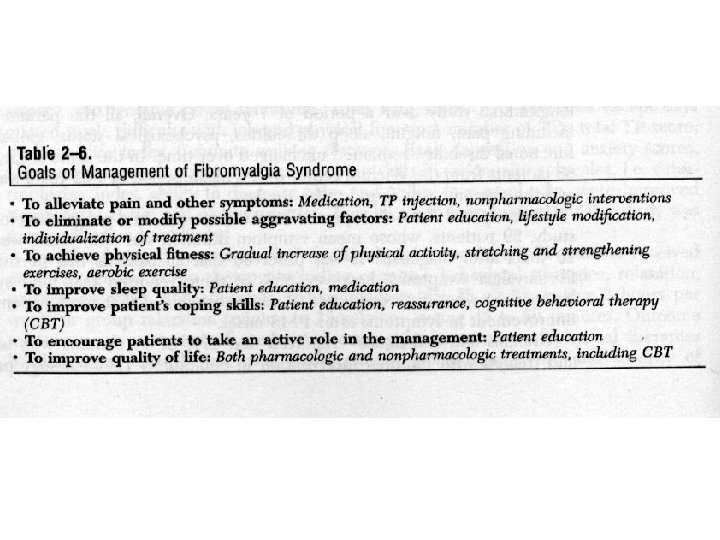
Treatment strategies • Nonpharmacologic and pharmacologic intervention • Aerobic exercise • EMG-biofeedback • Acupuncture • Physical therapy • Cognitive behavioral therapy
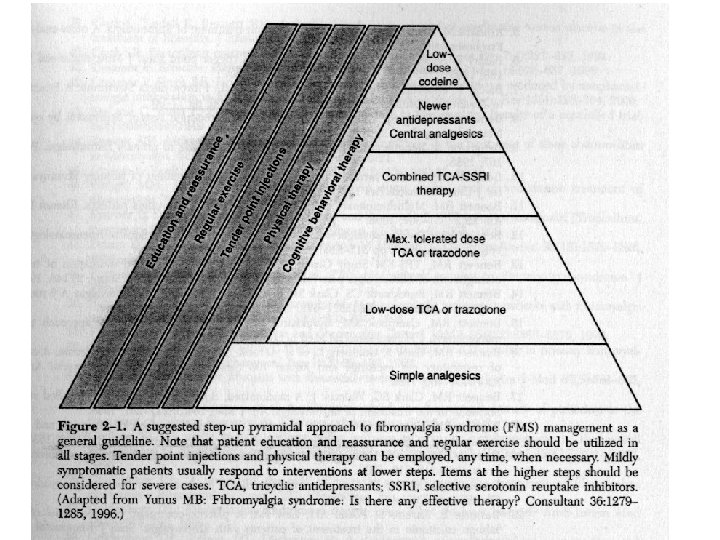

Simple analgesia • NSAID and acetaminophen • Numerous studies failed to confirm their effectiveness as analgesics in FMS • If co-morbid with OA, RA and SLE, patients can experience enhanced analgesia with combinations of NSAIDs and other agents

Tricyclic antidepressants • Most TCAs increase the concentration of 5 -HT and NE by directly blocking re-uptake • Additional blockade of certain cation channels as histamine, acetylcholine and NMDA mediated glutamatergic neurotransmission • Poor side effects about antihistaminergic and antiacetylcholinergic ability
: pain, poor sleep and fatique, but not mood-elevating effects")
Tricyclic antidepressants • TCAs (Amitriptyline): pain, poor sleep and fatique, but not mood-elevating effects • IBS, TMD and CLBP are treated by TCAs • Dose: from 10 mg 1 -2 h before sleep, and to max dose 50 mg/day • Morning “hangover”, sicca symptoms and BW gain • With caution, patients with cardiac disorders esp. arrhythmia

Selective serotonin reuptake inhibitors • SSRIs primarily inhibit the re-uptake of 5 -HT, and they typically lack the extra-monoaminergic activity • SSRIs are well suited for patients presenting with significant mood disorders, particularly those not tolerant to TCA side effects • Combination of SSRIs with low-dose TCAs can be synergic

Monoamine oxidase inhibitors • MAOIs block monoamine breakdown after release from the neuron • MAOIs show greater efficacy than TCAs in treating atypical depression, a subtype of depression associated with chronic pain conditions

Anti-epileptic drugs • AEDs increase the seizure threshold through sodium and calcium channel blockade or increasing inhibitory neurotransmission • Clonazepam may be a useful agent in FMS with TMD and leg restless syndrome • Neurontin is specific for postherpetic neuralgia, and can treat a variety of pain

Sedative- hypnotics • Zopiclone and zolpodem at standard doses have been shown to improve sleep in FMS • The importance of improving sleep in FMS should not be under-rated, as a poor night’s sleep has been shown to result in more pain and fatigue the next day

Muscle relaxants • Cyclobenzaprine is taken before sleep appears to improve sleep and pain in FMS • Morning hangover and dry mouth is its common side effects • Tizanidine is a centrally acting alpha -2 agonist for treatment of muscle spasticity associated with multiple sclerosis and stroke • A reduction in Sub P level in CSF of patients with FMS

Opiates • The main problems are the effects on cognition, reduced motivation to pursue non-pharmacological treatment modalities, and aggravation of depression • Tramadol from 50 mg bid to 100 mg qid • Ultracet (tramadol 37. 5 mg + acetaminophen 325 mg) is better tolerated than tramadol alone

Question ?
- Slides: 26