Phantom SensationPain BY JOSIP SULENTIC Pain theory Phantom

Phantom Sensation/Pain BY JOSIP SULENTIC

Pain theory

Phantom Sensation Any sensory phenomenon that is felt in the absent limb or a portion of it. Up to 98% of amputees feel phantom sensation following an amputation Phantom sensation is felt by spinal cord injuries, amputees (congential, vascular, trauma etc) Types include: - Sensations of movement - Sensations of temperature, touch, pressure and itchiness - Sensations of limb position, length (telescoping) and volume

What is Phantom Pain?

What is Phantom Pain? “True phantom limb pain is a complex, poorly understood pain syndrome that is described as burning, aching, or electric-type pain in the amputated limb. The diagnosis of phantom pain should only be made after other causes of stump pain have been eliminated including ischemia, infection, neuroma, and pressure-related wounds. ” Phantom Pain is almost exclusive in amputees. Whereby amputees feel phantom sensation with PAIN. Spinal cord injury patients can feel phantom sensation WITHOUT pain.

Incidence of Phantom Pain Varies in literature – ranging from 5% to 85% - depending on diagnostic criteria that is used to define phantom pain. At Westmead, all my patients have at one point complained of phantom pain. Poor control of pain and preoperatively and postoperatively may lead to an increase in chronic phantom pain. Trauma vs vascular – Evidence suggests there is little difference between the 2 in terms of intensity. However, clinically, traumatic patients have reported greater intensity of phantom pain than vascular patients.

Pathophysiology No certain explanation regarding pathophysiology but theories that are currently accepted are: 1. Peripheral mechanisms i. e. neuromas

Pathophysiology Spinal mechanisms

Pathophysiology Central mechanisms 2. Central mechanisms

Management of Phantom Pain

Pharmacological Evidence shows that preemptive epidural analgesia or PCA 48 hours prior to amputation and 48 hours post amputation can lead to a significant decrease in phantom pain 6 months after the amputation. Morphine, gabapentine and ketamine show favourable results in the short term. Limited evidence for effects of opioids on chronic phantom pain (however, this is often prescribed for patients by the treating team).

Mirror therapy

Mirror Therapy cont’d Systematic review = 20 studies = 5 RCTs + 6 prospective studies + 9 case studies Results 17/18 studies showed low level evidence on the efficacy of Mirror Therapy on Phantom Limb Pain 1 RCT showed no significant effect of mirror therapy on Phantom Limb Pain 8 studies showed significant effects of mirror therapy on phantom limb movement, 4 low level evidence + 4 high level evidence.

Visualisation techniques

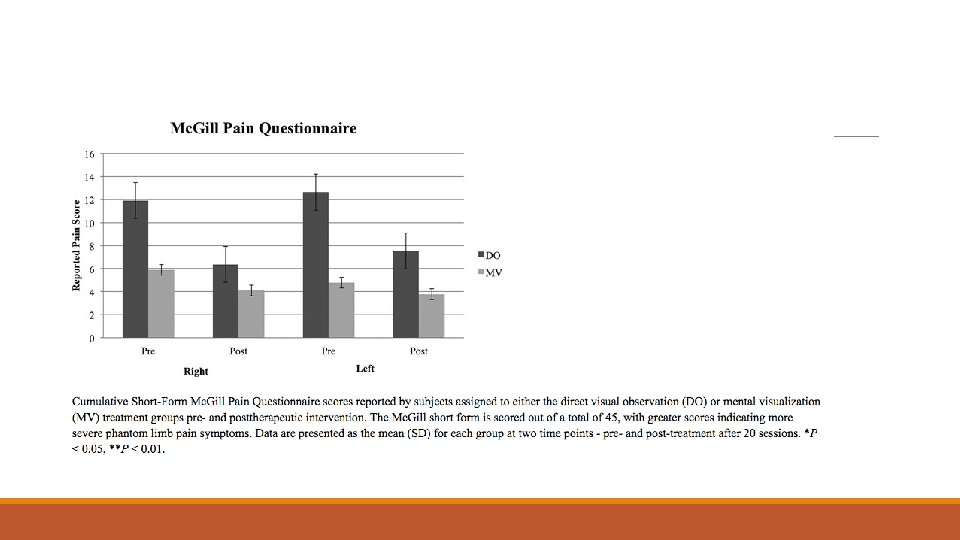
Visualisation techniques cont’d RCT of 20 bilateral amputees with Phantom Pain divided into 2 groups Group 1: n – 11 mentally visualising the movement Group 2: n – 9 patient facing the experimenter perform 7 discrete movements whilst the amputee mentally copied the movement for 20 mins/day for 1 months. 7 movements were Abduction and Adduction of the great toe, Flexion and extension of the ankle, inversion and eversion of the ankle, flexion and extension of the toes, rotation of the ankle and knee flexion and extension (for AKAs)

Visualisation techniques

Muscle relaxation, MI and Phantom Xs

Muscle relaxation, MI and Phantom Xs RCT unilateral amputees with phantom pain or sensation 1. Experimental group n=27 = Progressive mm relaxation exercises i. e. moving the mind through different regions of the body to re-establish contact with it. Imagined movements – copy position of phantom limb to intact limb and then move in opposite direction and treturn to start – repeated 15 times or until phantom pain disappeared 2 times a week for 4/52 2. Control group n=24 = general Xs program in addition to standard physical therapy, Xs included strengthening, stretching, dynamic isometric Xs for the residual limb.

Results

Acupuncture

Acupuncture cont’d RC feasibility study 24 Amputees included, 15 particpated, 8 males, 7 females (8 vascular, 4 Trauma, 3 other), 6 AKAs, 9 BKAs Control = usual care = pharmacological intervention Experimental group = followed TCM British guidelines – mirroring local and distal points by needling the intact limb = 8 session for 1 hour x 2/week for 4/52. Needles in situ for 20 -30 mins
 scores = Control 5. 43 to 4. 43 Experimental 5.")
Acupuncture results NRS (VAS) scores = Control 5. 43 to 4. 43 Experimental 5. 44 to 2. 75 Cohen’s different size = 0. 64 ~ medium to large effect bw groups

Weird stuff

Weird stuff cont’d RCT, 57 subjects, upper and lower limb amputees with a healed residual limb who had 3 or more episodes of phantom pain in the last 3 months. Experimental = n = 30, wore the Farabloc limb cover the prosthesis and wore the cover the residual limb when the prosthesis was taken off. The cover was worn for 24 hours a day, 7 days a week for 12 weeks Control = n = 27, wore sham cover for the same period of time. Results – non significant reductions in phantom pain for both groups. Phantom pain scores were comparable in both groups.

Practice at Westmead Combination of pharmacological and non-pharmacological treatments. Motor functional empathy Left/Right discrimination Visualisation techniques Mirror Therapy Neural glides TENS machine

Mirror therapy Imagining L/R movements L/R discrimination, recognise/orientate apps Watching someone do the movement

Motor functional empathy

Left/Right discrimination

Explicit MI/Visualisation techniques

Mirror therapy

Neural glides

Tens machine

References 1. Alviar, M. J. , Hale, T. and Dungca, M. , 2011. Pharmacologic interventions for treating phantom limb pain. Cochrane Database Syst Rev, 12. Hsiao, A. F. , York, R. , Hsiao, I. , Hansen, E. , Hays, R. D. , Ives, J. and Coulter, I. D. , 2012. A randomized controlled study to evaluate the efficacy of noninvasive limb cover for chronic phantom limb pain among veteran amputees. Archives of physical medicine and rehabilitation, 93(4), pp. 617 -622. 3. Tung, M. L. , Murphy, I. C. , Griffin, S. C. , Alphonso, A. L. , Hussey‐Anderson, L. , Hughes, K. E. , Weeks, S. R. , Merritt, V. , Yetto, J. M. , Pasquina, P. F. and Tsao, J. W. , 2014. Observation of limb movements reduces phantom limb pain in bilateral amputees. Annals of clinical and translational neurology, 1(9), pp. 633 -638. 4. Brunelli, S. , Morone, G. , Iosa, M. , Ciotti, C. , De Giorgi, R. , Foti, C. and Traballesi, M. , 2015. Efficacy of progressive muscle relaxation, mental imagery, and phantom exercise training on phantom limb: a randomized controlled trial. Archives of physical medicine and rehabilitation, 96(2), pp. 181 -187. 5. Trevelyan, E. G. , Turner, W. A. , Summerfield-Mann, L. and Robinson, N. , 2016. Acupuncture for the treatment of phantom limb syndrome in lower limb amputees: a randomised controlled feasibility study. Trials, 17(1), p. 519. 6. Ephraim PL, Wegener ST, Mac. Kenzie EJ, et al. Phantom pain, residual limb pain, and back pain in amputees: results of a national survey. Arch Phys Med Rehabil 2005; 86: 1910. 7. Barbin, J. , Seetha, V. , Casillas, J. M. , Paysant, J. and Perennou, D. , 2016. The effects of mirror therapy on pain and motor control of phantom limb in amputees: A systematic review. Annals of physical and rehabilitation medicine, 59(4), pp. 270 -275.
- Slides: 34