PFC Medical Planning Use the 10 Capabilities Grid

PFC Medical Planning

Use the 10 Capabilities Grid to Figure out what capability you are deficient on and then Identify what asset in your AO has it available. • Couldn’t get a ventilator to bring? • Make finding one a priority in your planning and note it on your grid and map

10 Essential PFC Capabilities 6. Physical Exam and Diagnostics 2. Resuscitate 4. Control the Airway 5. Sedation and Analgesia BP Cuff, Stethescope, Pulse Ox, Foley Fresh Whole Blood Kit Bag-Valve-Mask with PEEP Valve Awake Ketamine Cric Opiate Analgesics titrated through IV Physical Exam without advanced clean, warm, dry, padded, catheterized Chest tube, cric Make comms, present patient and key vitals Be familiar with stressors of flight Capnometry 2 -3 cases of LR for Burn Resus O 2 Concentrator Long duration sedation Sedation with Ketamine/option of midazolam Ultrasound and point of care labs Elevate head of real beddebride, washout NG/OG Fasciotomy debridement, amputation Add labs and ultrasound video Trained in critical care transport Vital Signs Monitor PRBS, FFP, Type specific donors Portable Ventilator Proficient in Rapid Sequence Intubation Educated and practiced imulti drug sedation Experienced and trained in above Experienced in all nursing care concerns Trained and experienced in above Real time video conference Experienced in critical care transport Ruck Pulse Ox, Head Lamp 1 FWB Kit per man, 2 250 cc bag NS BVM with PEEP Valve Cric Kit, LMA/SGA, lidocaine and ketamine IM Fentanyl TML, Perc PO, Ketamine IM/ IV Urinalysis test strips, fluorescein strips Compct Foley kit, Sterile kerlix, litter padding Cric, 10 g. Needle D Scalpel Cell Phone and call sheet Have checklist available Truck BP Cuff, Stethescope, capnometry, small monitor Casre LR, Additional FWB Kits, 3% Saline SAVent or SAVE 2 RSI, LMA/SGA, Cric kit ketamine bag IV Ketamine IV with midazolam Blood tubes to drop off labs at HN clinic on the way Padded litter, NG, Sterile Chest Tube Kit with drapes Cell phone and call sheet, sat phone, radio Checklist plus flight evac kit House Add defibrillation 2 additional cases LR, Case NS, Additional 3% Saline No Ventilator; Available with SURG team at capitol All from above Add Benzo if not available for truck Same as above No Lab capability; Available with SURG team at capitol Real matress with head elevated, nursing care kit sleeping bg Sterile Surgical Kit with Drapes, Gowns and scrub soap Secure comms, email Extensive evac kit Plane Take all of above All of above SAVent on O 2 All above calculate for flight and double All above calculate for flight time and double Padded Litter, Sleeping Bag 10 g needle D Chest tube kit Cric kit Through aircraft From Above 1. Monitoring Minimum Better Best 7. Nursing and Hygeine 8. Surgical Interventions 9. Telemedical Consult 10. Package and Prepare for flight 3. Ventilate and oxygenate

Now on to the moving pieces…

Team Members/ Organic Assets Type and Name Telephone Radio Freq / Call Sign e. Mail Senior Medic: John Smith +27 456 -345 -6789 18 D 1 Junior Medic: RFR: TCCC/MARCH: CLS First Aid/Buddy Aid NO MEDICAL TRAINING (liabilities) Medical Capabilities Limitations Special Equipment

Surgical Assets Type Of Team / Number Pax? Battalion FAS SOST MFST CSH Local Surgeon Telephone / Date Last checked Radio Freq / Call Sign e. Mail Blood Available? FWB Kits Highest Trained Surgical Person Capabilities Surgical Limitations Able to Travel? How Far? With whom?

Cas. Evac Platforms Type Vehicle / Aircraft / Location Razor / ATV Team Truck HN Ambulance Civilian Helo Casa 212 Twin Otter Cessna Telephone Radio Freq / Date Last called Call Sign e. Mail Capablities / Distance / Speed / Equipment Limitations (Contract, Weather etc. . ) Military or Civilian? Country of Origin? Medic On Board? Contract Info Distance, Cash Other Good to Know Info

Strategic Evacuation Platforms Type Vehicle / Aircraft / Location C-146 C-130 C-17 Civilian Air Evac Telephone Radio Freq / Date Last called Call Sign e. Mail Capablities / Distance / Speed / Equipment Limitations (Contract, Weather etc. . ) Military or Civilian Contract Info Distance, Cash Other Good to Know Info

Refueling Stations / FARPs Name MSS 1 MSS 2 Airstrip A Airstrip B Main Airport FARP II Telephone / Date Last Checked? By Whom? Radio Freq / Call Sign e. Mail Location Country / State / City / Address / Grid Manned? By Whom? Limitations Evaluation Last Done. By whom? Other Good to Know Info

Telemedicine Contacts Who Telephone / Date last checked Radio Freq / Call Sign e. Mail Last time checked? By whom? Level of Training / Specialty Location

Facilities Name MSS 1 MSS 2 Team House / Aid Station Battalion FAS CSH Local Clinic Local Hospital Telephone / Date Last Checked? By Whom? Radio Freq / Call Sign e. Mail Location Country / State / City / Address / Grid Capabilities Surg? Blood? Imaging Limitations Evaluation Last Done. By whom? Other Good to Know Info

Add Regional Map And Locations Clinic Team Houses / Bases 600 km LZ 143 C-130 Coalition Med Facility / Team Host Nation Med Facility Air Port / Landing Strip H LZ / FARP MSS 600 km Scale Range / Distance

Add Local Map and Locations Clinic Team Houses / Bases 50 km H Coalition Med Facility / Team LZ 143 MI 17 Helo Host Nation Med Facility Air Port / Landing Strip H LZ / FARP MSS 50 km Scale Range / Distance
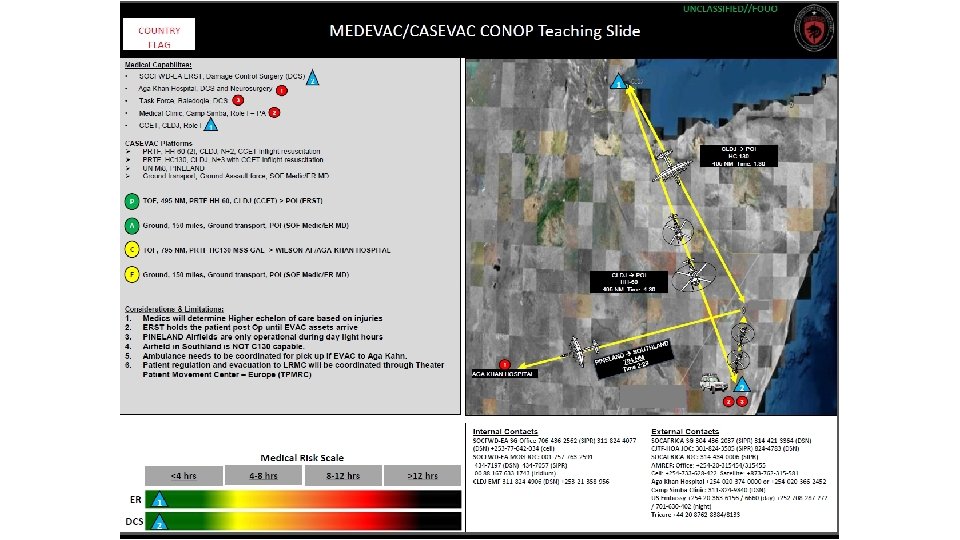

Medical/CASEVAC CONOP slide • Why • • • Amount of force providers rotating Different medical plans Lack of research Mutual support Other COCOM priorities Squeezing the balloon

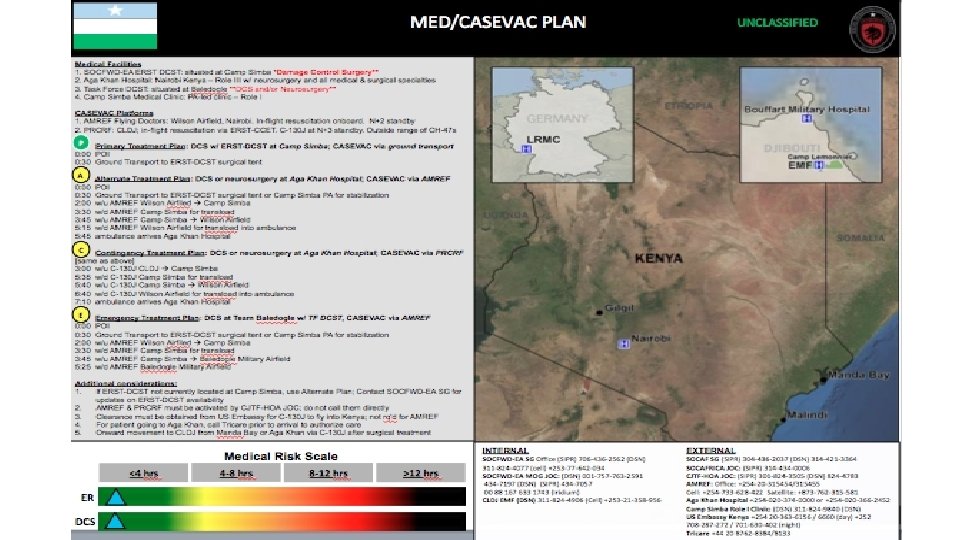
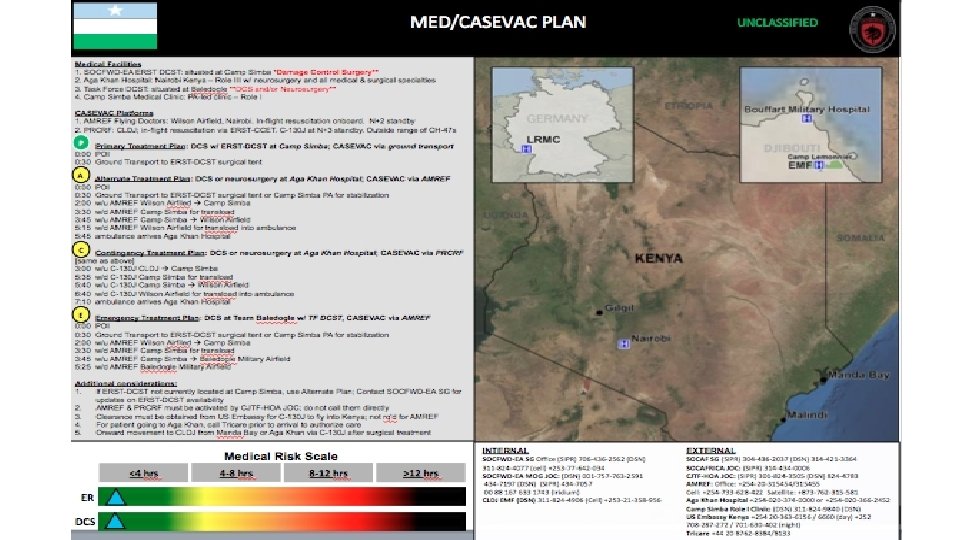
Header/top of slide • Classification noted • Country of operations. If it’s multiple countries, use SOCFWD flag • SOCAFRICA flag on the right • Title will be Operation/Team name MEDEVAC or CASEVAC CONOP

Medical Capabilities • Focus to care is beyond the capabilities of SF/SOF medic • “Self aid/buddy aid” and “all team members are TCCC qualified” are unacceptable - already assumed. Underwear goes on the inside. • Designated numbers/letters within this block will correspond throughout the plan. • Triangle will correspond with the medical risk scale at the bottom and the map • The circled numbers will correspond where on the map they are located

CASEVAC PLATFORM: Thought should be given to infil and exfil platform. • Can they loiter if immediate exfil is needed? • Include all platforms intended to be used in CASEVAC plan (Contract Aviation, Personal Recovery, SOCAF owned, Coalition and HN (if feasible). • What is your platform’s spin up and launch times over the geographical distance? , • Thought to platforms ability to land on improved/ unimproved surfaces and travel time and speed. • This needs to be captured in a narrative portion of the plan and depicted on the map to the right.

PACE OPTIONS • A coherent application of assets available to you

Considerations & Limitations • Highlight relevant issues noted • “Driving through Nairobi at night will affect patient transportation to AGA KHAN • “Pilots are not NVG qualified to fly at night” • Relevant facts to this specific mission • What are the refuel times if you have to “lily pad” across to your next destination? • What are your patient transfer times? • Expect changes due to operational needs

Medical Risk Scale • This is in reference to your BEST plan; which is your “P. ” • “ER” is your primary ER • “DCS” is your primary DCS Definitions: ER – Emergency Room is a facility/location that is able to stabilize a patient prior to surgery. It’s also a capability above the tactical element (ex: TCCET, MOG UN ER, CCET, SOST) DCS- Damage Control Surgery is the rapid initial control of hemorrhage and contamination with packing and a temporary closure.

MAP • This is a pictorial representation of all the information we had on the left translated onto the map • A visual for your information • Should systematically match what you have on the left • The Blue triangles connote where your closets American DCS and ER assets are located and matches your medical risk scale

CONTACT INFORMATION • Order of precedence of phone numbers • Clear and concise • Split up in 2 sections: Internal/External • Internal should be “down and in” • External should be “up and out” • Phone numbers should be limited due to the SOCFWD JOC’s and the Surgeons will coordinate follow on care.
- Slides: 25