Perspectives in Palliative Care Palliative Care in noncancer










. • Performance status")


- Slides: 14
Perspectives in Palliative Care • Palliative Care in non-cancer conditions • Dr Claire Douglas • Consultant in Palliative Medicine
Overview of the afternoon • Introduction – Why do we need to address the issue of palliative care in non-cancer conditions • Presentations from non-cancer specialties • Summary and objectives for the group
Death in Scotland §Number of deaths per year is expected to rise by 9000 to 62, 000 per year by 2037 (ONS, 2015) • Location of deaths in Scotland: o. Acute setting 52. 3% (Decreasing) o. Community 30. 3% (Increasing) o. Hospice 17. 4% (Increasing) (Sharpe et al, BMJ Supportive and Palliative Care 2015) §On a given day in Scottish hospitals: 30% of those admitted died within the next year o 10% die during that admission o(Clark et al, Pal Med 2014)
Deaths per GP in the UK Home death more likely if: • Cancer • Young • Professionals to support carers • Live with someone
Symptoms Symptom Cancer % HF % COPD % CKD % Dyspnoea 10 -70 60 -88 90 -95 11 -62 Pain 35 -96 41 -77 34 -77 47 -50 Fatigue 32 -90 69 -82 68 -80 73 -87 Depression 3 -77 9 -36 37 -71 5 -60 Anxiety 13 -79 49 51 -75 39 -70 Anorexia 30 -92 21 -41 35 -67 25 -64 Solano, Gomes and Higginson JPSM, 2006
By 2021 all people who need palliative care should have access to it’
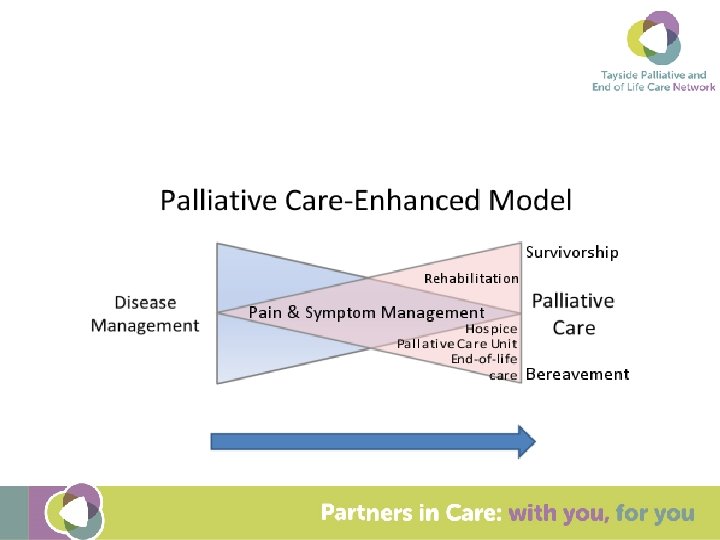
What is palliative care and end of life care? Palliative care is an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, by means of early identification and assessment and treatment of pain and other problems, physical, psychosocial and spiritual. (WHO, 2010) It is part of core business and need varies: Generalist palliative care needs Specialist palliative care needs End of Life care relates to last year of life Care of Dying – last days / hours of life
What do people want at the end of life To be with loved ones To avoid life prolonging treatments and interventions To put their affairs in order To have good symptom control
Barriers to palliative care in non-malignant disease Difficulty in recognizing patient may be in last months / year of life Uncoordinated care / communication between primary and secondary care
Prognostication Disease Trajectories Murray et al. BMJ 2005
Triggers for palliative care approach and assessment • Unplanned hospital admission(s). • Performance status is poor or deteriorating • Significant weight loss • Persistent symptoms despite optimal treatment of underlying condition(s). • The person (or family) asks for palliative care; chooses to reduce, stop or not have treatment; or wishes to focus on quality of life.
Review current care and care planning. • Review current treatment and medication • Consider referral for specialist assessment if symptoms or problems are complex • Agree a current and future care plan
Summary Palliative Care needs in non-malignant disease are high Optimal medical management can occur alongside palliative approach Should focus on the problems not prognosis for non-malignant disease and plan for future deterioration How can this group help address the palliative needs of patients with non-cancer illness in Tayside?