Persistent postop hypoxia ICU Pamela Youde Nethersole Eastern





















- Slides: 22
Persistent post-op hypoxia ICU, Pamela Youde Nethersole Eastern Hospital Dr Emily Cheung & Dr Arthur CW Lau 24 Sep 2010 1
Case M/69, ADLI Ex smoker, drinker PMH: ◦ e. Ag negative chronic hep B ◦ Ulcerative colitis on mesalazine ◦ HT
Newly diagnosed HCC over right lobe ‘C’ adm for open right hemi- hepatectomy Uneventful operation Intra-op finding: ◦ Large tumor at seg V of liver ◦ Liver not cirrhotic macroscopically
Post op extubated and transferred to ICU for monitoring ◦ Post op on 6 L O 2, gradually tail down O 2 requirement ◦ On 2 L O 2 without SOB on discharge ◦ Discharge from ICU on D 1
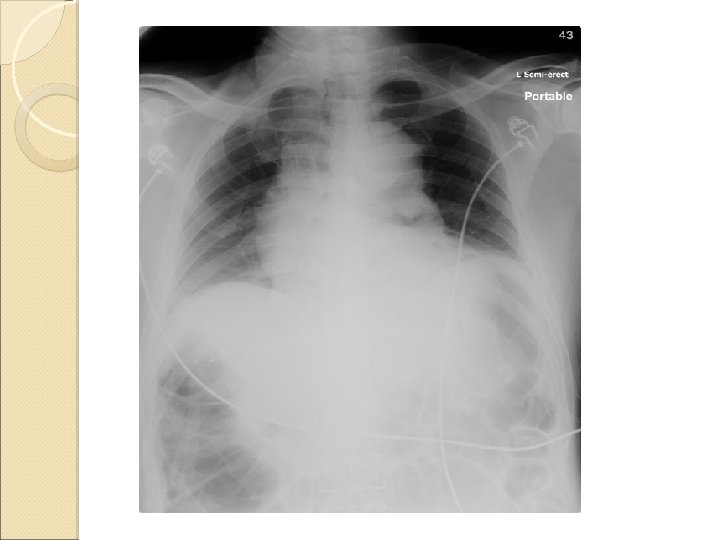
Developed abdominal distension with post-op ileus on D 3 Increasing O 2 requirement and desaturation noted in general ward Readmitted ICU on D 4 Required 12 L O 2 on admission to ICU ABG on O 2: unremarkable
CT – lung window
CXR and CT reviewed ◦ suggestive of some atelectasis in dependent part of both lower lobes ◦ Probably contributed by bowel distension ◦ No evidence of PE or chest infection
Progress ◦ NIV given for a short period of time, but not very responsive ◦ Chest physio with lung expansion by incentive spirometry started ◦ However, still noticed occasional desaturation ? Causes for persistent hypoxaemia
Detailed history taking Complaints of discomfort on sitting up while watching TV, feels better if lying down Symptoms present for 2 years P/E: ◦ No Stigmata of chronic liver disease ◦ No clubbing, spider naevi ◦ No gynecomastia
Patient complaints SOB while sitting up, relieved by lying Platypea More than three repeated trials of Sp. O 2 measurement on 3 L O 2 Orthodeoxia ◦ Lying: Sa. O 2 > 93% ◦ Sitting: Desaturated with Sa. O 2 down to 81%, not fully correctable by increasing Fi. O 2
Bedside Echo with contrast by ICU Team ◦ Chamber sizes relatively normal ◦ Presence of intrapulmonary shunt, as indicated by bubbles on left side after 3 rd beat Ddx: ◦ Intrapulmonary/Intracardiac shunt ◦ More likely intrapulmonary shunt because bubbles did not occur immediately on L side postbubble contrast injection Discharged from ICU on D 8 ◦ Reviewed by medical team
Progress Inpatient Echo repeated by Cardiac team on D 14 ◦ mild pul hypertension ◦ Bubbles contrast was seen in LA and LV after injection, suggested the presence of right to left shunt ◦ no definite intra-cardiac shunt was detected ◦ Ddx: intra-cardiac/intrapulmonary AV shunt Patient refused TEE 13
Impression of the causes of hypoxemia Hepatopulmonary syndrome, and 2. Atelectasis due to bowel distension 1.
Hepatopulmonary syndrome Characterized by a defect in arterial oxygenation induced by pulmonary vascular dilatation in the setting of liver disease Trial of ◦ Liver disease ◦ Pulmonary vascular dilatation ◦ Defect in oxygenation
Source: Roberto Rodríguez-Roisin, M. D. , and Michael J. Krowka, M. DHepatopulmonary Syndrome — A Liver-Induced Lung Vascular Disorder. NEJM, Volume 358: 2378 -2387 May 29, 2008 Number 22
Clinical features 18% asymptomatic Platypnea : ◦ Dyspnea improves when lying flat Orthodexoia: ◦ Hypoxemia worsens upon sitting up and improves when lying flat ◦ p. O 2 decreased by > 5% or > 0. 5 k. Pa
Opacification of right atrium and right ventricule with microbubbles and delayed opacification of the LA and LV 18
Pathobiology Gross dilatation of the pulomonary precapillary and capillary vessels Absolute increase in no of dilated vessels Pleural and pulmonary AV communications and portopulomonary venous anastomoses 19
Dilated capillaries not uniform blood flow Venous blood passed rapidly or directly thro intrapulmonar yshunt to pulmonary veins VQ mismatch 20
Treatment No effective medical therapies Liver transplantation is the only successful treatment ◦ p. O 2 < 60 mm. Hg is considered to be an indication for liver transplantation Long term oxygen therapy ◦ For symptomatic patients with severe hypoxaemia 21
THE END 22