Peripherally Inserted Central Catheter PICC Trouble Shooting Chantal
 Trouble Shooting Chantal Miljours, RN BSc. N Clinical Nurse")
Peripherally Inserted Central Catheter (PICC) Trouble Shooting Chantal Miljours, RN BSc. N Clinical Nurse Educator Diagnostic Imaging Department North Bay Regional Health Centre

Objectives How and why PICC lines are inserted n Identify catheter occlusion and trouble shooting methods n Identify potential causes for redness in PICC arm and at insertion site n Air Embolism n Case Studies n

Purpose of Central Venous Access Device n n n To infuse fluids (allows for large volume boluses) No peripheral access To infuse TPN To infuse medications To sample venous blood (when no peripheral access is available) To provide a method for hemodynamic monitoring i. e. : right atrial and PA pressures(acute care setting)

Blood Vessels involved in Central Venous Therapy basilic n cephalic n axillary n jugular n subclavian n innominate These veins all lead to superior vena cava n

Central Venous Access Devices Port-a-Cath Hickmann Line

Central Venous Access Devices Short term central catheter Peripherally Inserted Central Catheter

PICC Line Placement

PICC Line Placement

PICC Lines n n n PICC lines are inserted as a sterile procedure in the diagnostic imaging department Both Ultrasound and Fluoroscopy are used insert the PICC line and confirm proper placement Insertion is performed by specially trained nurses and placement is confirmed by the radiologists

STATS 2014 356 PICC lines inserted in 2014 n n 12% for TPN 39% Antibiotics 39% Chemotherapy 10 % other

Troubleshooting n In 2014 we saw 149 patients for PICC line troubleshooting n Only 57% of these patients required thrombolytics

CVAD Occlusions There are 3 types of occlusions Complete n Partial n Withdrawal n

Signs of a CVAD Occlusion Resistance when flushing n Sluggish flow n Inability to infuse fluids n Frequent occlusion alarm on infusion pump n Infiltration or extravasion or swelling or leaking at insertion site n Inability to withdraw blood n Sluggish blood return n

Complete Occlusions n n Inability to infuse or withdraw blood or fluid into the CVAD Can be mechanical, chemical or thrombotic

Withdrawal Occlusions Inability to aspirate blood but ability to infuse without resistance n Lack of free-flowing blood return n

Partial Occlusions Decreased ability to infuse fluids n Resistance with flushing and aspiration n Sluggish flow through the catheter n Can me mechanical, chemical, or thrombotic n

Types of Thrombotic Occlusions Intraluminal n n Often cause complete catheter occlusions Develops from blood build up as a result of insufficient flushing, inadequate infusion rate, or frequent blood withdrawals Fibrin Tail n n Fibrin adheres to the end of the catheter and causes more cells to be deposited on the tail Acts as a one-way valve: fluids can be pushed out but with aspiration the tail is sucked back over the opening Mural Fibrin Sheath n n Fibrin adheres to the external surface of the catheter, creating a “sock” over the catheter Occasionally the sheath covers the end of the catheter and causes occlusion n n Occurs when fibrin from a vessel wall injury binds to fibrin covering the catheter surface Caused by the catheter rubbing in the vessel, traumatic insertion, or poor blood flow
")
Dual-Lumen PICC (Navalist)

Fibrin Sheath Occlusions n n n Fluid can usually be injected, but blood cannot be aspirated Infiltration/extravasation can occur when medications are infused up the fibrin sheath and back to the insertion site May cause mixing of incompatible solutions


CASE STUDIES

Case Study #1: The Repeat Offender n 69 year old patient receiving antibiotics through the PICC line is sent to DI by homecare for a withdrawal occlusion. This patient has been seen multiple times in the past 2 weeks.

Chemical Occlusions n Many PICC line occlusions are caused by a build-up of precipitate from antibiotic or other medications

Precipitate

Troubleshooting tips First determine there is no mechanical cause for the occlusion n Assess for kinks, closed clamps, or change in external length n Assess for clogged cap or if the cap is on too tight (finger tip tight) n Assess for positional catheter: n Reposition arm, have patient cough, put patient in Trendelenberg position

The Art of Flushing n n n Knowing how PICC feels with flushing can tell you what is happening with PICC Flush with 20 ml Normal saline turbulent flush to each port after each use May require daily flushes depending on medication i. e. Vancomycin


Troubleshooting tips n n Remove any add on devices such as cap or y -connector and attempt to aspirate and flush the catheter directly at the hub with normal saline Consider changing the dressing to ensure there is no twisting/kinking of the catheter

Troubleshooting tips Once mechanical obstructions have been ruled out: n If no blood return on aspiration, may alternate gently drawing back and then gently flushing n Try using a dry 3 cc syringe to aspirate blood returns as it exerts less negative pressure when withdrawing n If still unable to get returns will require Cathflo instillation. n Consider radiography to determine

Case #2: What Do You See?

Case #2 n n n Patient sent to ED with a blocked PICC line, home care nurse unable to flush or get venous returns Upon assessment in ED blood noted backed up in catheter hub. Cathflo instilled overnight in ED for complete occlusion. Patient to return in am for follow up assessment in am with DI Nurse.

Case# 2 What is missing? n What is wrong with this PICC? n

Solution n n When questioned about the missing clamp, the patient states “ the nurse cut it off because it was digging into his skin” Do Not Remove any clamps that is attached a CVAD RISK OF AIR EMBOLISIM Patient required new PICC line insertion If unsure about type of CVAD device look it up or consult with DI nurse.

CVAD 911 Emergency! Damaged PICC line, hickmann line or any central line n RISK FOR AIR EMBOLUS n DVT n

Air Embolism Venous air embolism can occur during time CVC insertion, while catheter in place or at time of removal n Air can easily get into vascular system when needle or catheter open to atmosphere n As little as 200 ml of air can be fatal n

Signs and Symptoms Air Embolism Sudden complaints of dyspnea n Respiratory distress n Coughing n Chest pain n Tachyarrhythmia's n Cardiovascular collapse n

Treatment for Air Embolus Lay patient on left side n Trendelenberg position n 100% oxygen n Call 911 n Supportive measures ( i. e. fluid resuscitation) n

Case #3 : What Do You See?

CASE: 3 65 year old woman with breast cancer is receiving chemo through a PICC line in the right basilic vein n CT tech unable to get blood returns from PICC n Pt had states had a recent fall on the ice injuring her right shoulder n Upon further exam noted distended veins n

Case #3: Deep Vein Thrombosis The patient had an obstrutive DVT in her right arm from the basilic vein to the subclavian vein n Sent to ER for treatment of DVT n PICC line pulled and reinserted after DVT resolved “ 70 -80% of thrombotic events occurring in superficial and deep veins of upper extremity are due to the presence of intravenous catheters” n
")
DVT n n An extraluminal thrombus can progress to a deep vein thrombosis (DVT) Fibrin build-up from the vein wall to the catheter may cause blockage of blood flow in the vein This can lead to SVC syndrome when the SVC is completely occluded and venous return cannot empty into the right heart to be oxygenated This is an emergency!

DVT n n Pt may experience redness to arm localized or can extend up arm Swelling to arm or hand(compare to non PICC line arm. May experience pain to arm chest neck No fever noted

Vein Measurement

Thrombus to Vein

Case Study # 4: The Quick Draw 60 year old female with hx of breast cancer, presented to ED with a fever. n Urine culture came back positive and admitted to hospital for urosepsis and was started on antibiotics n No blood culture drawn from PICC n PICC line pulled and tip sent for culture, came back negative n

Case # 4 Patient starting to improve on antibiotics n A febrile now n Limited peripheral veins due to lymph node involvement n Important to establish if patient has a true Catheter Related Blood Stream Infection (CRBSI) in order to decide whether to salvage, exchange, or remove the catheter. n

Systemic Antibiotic Therapy is NOT required for the following: Positive catheter tip in absence of clinical signs of infection n Positive blood cultures obtained through a catheter with negative cultures through a peripheral vein n Phlebitis in the absence of infection, the risk of CRBSI usually low n

CRBSI –catheter removal Severe sepsis n Hemodynamic instability n Endocarditis or evidence of metastatic infection n Erythema or exudate due to suppurative thrombophlebitis n Persistant bacteremia after 72 hrs of antimicrobial therapy to which the organism is suseptible n

Difficult PICC line Removal This usually due to venous spasm n Sometimes PICC lines can be difficult to remove especially if catheter too big for size of vein n Ask patient to relax arm n Apply warm compress n After these measures the PICC line usually comes out easily n

Case #5: What do you see?

Contact Dermatitis n Dermatitis presents as reddened irritated skin at the site n Always allow antiseptic (ie. Chlorhexidine) to dry completely before applying dressing n Consider changing dressing to IV 3000 n Consider changing antiseptic solution to povidone-iodine solution

Case #6 : What Do You See?

PICC Line Site problems Infection vs Dermatitis n Dermatitis presents as reddened irritated skin at the site n Infection presents as redness, swelling, warmth, and possible purulent drainage at site? n Does patient have a fever? n Does patient have any swelling to arm?

What do you See?

PICC Line Infection Send to ER with signs of sepsis (ie. Fever, chills, tachycardia, hypotension) n Rule out other sources of infection n Obtain cultures – draw blood culture from PICC line (do not discard a waste sample) and consider swab for C&S if site infection noted n Administer antimicrobials n Do not necessarily pull the PICC! n

Prevention n n Good hand hygiene Ensure to “Scrub the hub” with Chlorehexidine for minimum 30 sec prior to accessing devices Wear sterile gloves and mask (pt should wear mask as well) anytime opening dressing. Removal of unnecessary CVC should be regularly assessed.

Leaking at PICC site n n n If leaking at site is present when flushing or infusing through CVAD Send to DI for cathetero-gram (to rule out a hole in the catheter) Doppler studies (to rule out thrombosis

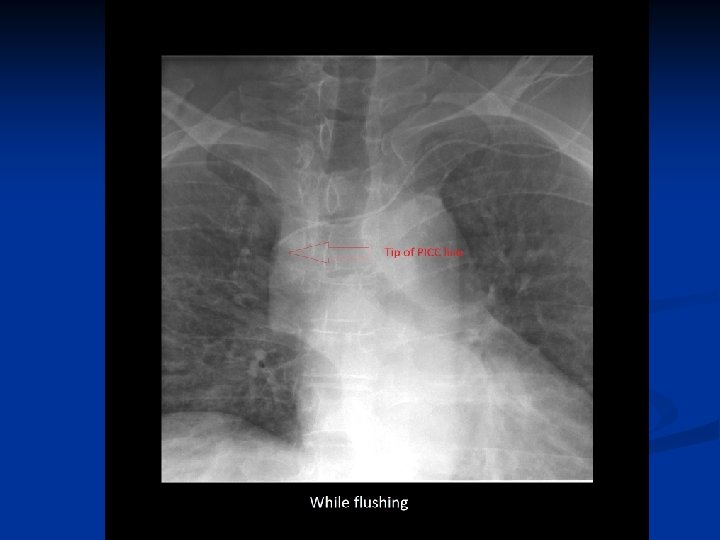
Case 4: Pain in the neck A 59 year old man with a PICC line in the right basilic vein presents with a withdrawal occlusion. n Has also been complaining lately of a constant “wooshing” sound in his right ear n The patient has been vomiting lately due to chemo treatment n Chest xray done to confirm proper placement… n
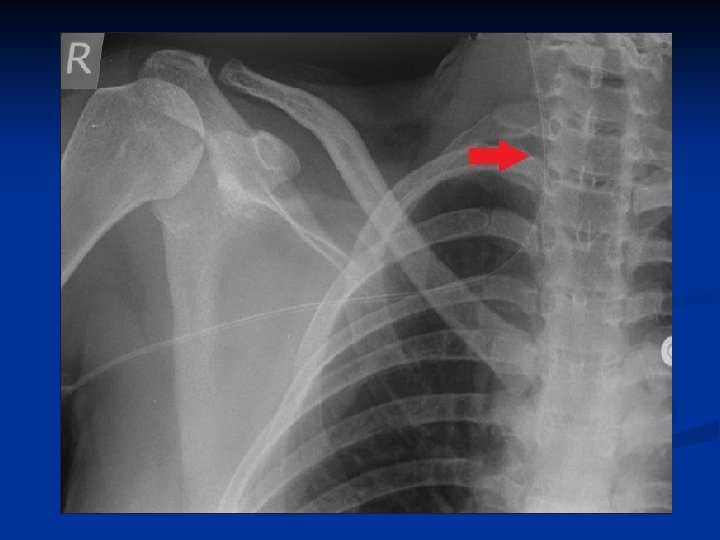

PICC line malposition PICC line must be removed and reinserted n If PICC pulled out more than 2 cm from original position, tape it in current position do not pull it out completely n Do Not attempt to push catheter back into position n Do not use PICC until tip placement confirmed by chest X-ray n

Cracked PICC If there is a crack or a hole present, determine location n Fold catheter over on itself and cover with tegaderm or other film dressing n Close catheter clamp if there is one n Send to hospital right away n

Cap on TOO Tight Crack more visible with cap on Crack faintly visible with cap off

Prevent Damage to PICC Never put steri-strips over picc line, always make sure they are underneath the line or on top of white wing n Do not force fluid into PICC if resistance is met n Ensure clamps are open before attempting to flush n Do not over tighten cap n

Broken PICC n n n If the end of the catheter breaks off grab CVAD (to prevent it from migrating internally) Fold catheter over, cleanse catheter, tape securely to arm, and send patient to hospital right away with the external portion of the catheter Monitor for air embolism

Broken PICC n If catheter disappears inside vein: Apply tourniquet to upper arm close to axilla n Place patient in Trendelenburg position n Call 911 n Monitor for air or obstructive embolism n

QUESTIONS ? ? ?
- Slides: 67