Periodontitis Acute periodontitis l Acute inflammation of the
















- Slides: 22
Periodontitis Acute periodontitis l Acute inflammation of the perodontal ligament gradually involving the whole periodontium Causes (4 I) l Injury: trauma due to external force or bite on hard object l Infection: Pulpitis, ANUG l Irritation due to improper filling l Impaction of foreign body (meat bone) l Etiological agent – Streptococcus, Staphylococcus, Borrelia vincenti l Fusiform bacillus Dr S Chakradhar 1
Clinical features l Toothache l Patient feels that the tooth is extruded l Fever l Malaise l Enlarged cervical LN Dr S Chakradhar 4
Management l Treat/remove the cause l Soft diet l Advise not to chew from affected side l Gargle with warm saline l Analgesics and anti inflammatory l Antibiotics l Prevent further damage by proper oral hygiene Dr S Chakradhar 5
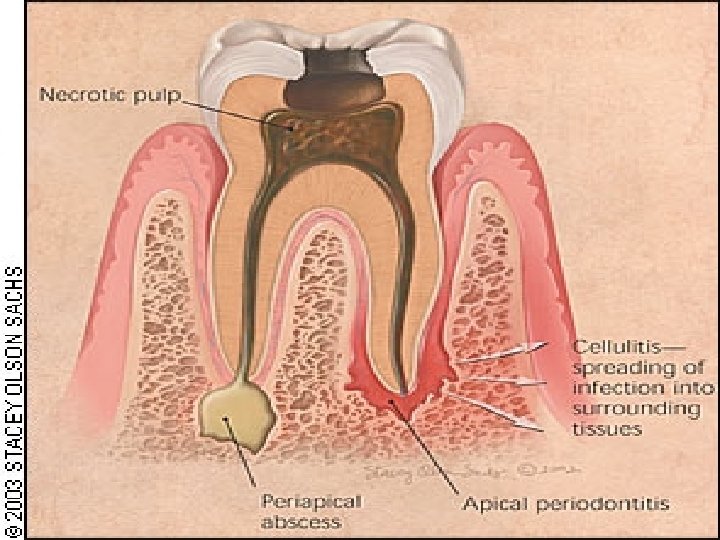
Periapical abscess l Usually a progression of periodontitis l History Severe throbbing pain l Tenderness l Diffuse swelling l Fever l
On examination l Inability to occlude l Fluctuant swelling in buccal or lingual region l Sensitive to percussion l Mobility l X ray may show periapical radiolucency
Management l Incision and drainage l Don’t give local infiltration as chances of dissemination of infection is there l Antibiotic coverage l Analgesic l Maintenance of oral hygiene
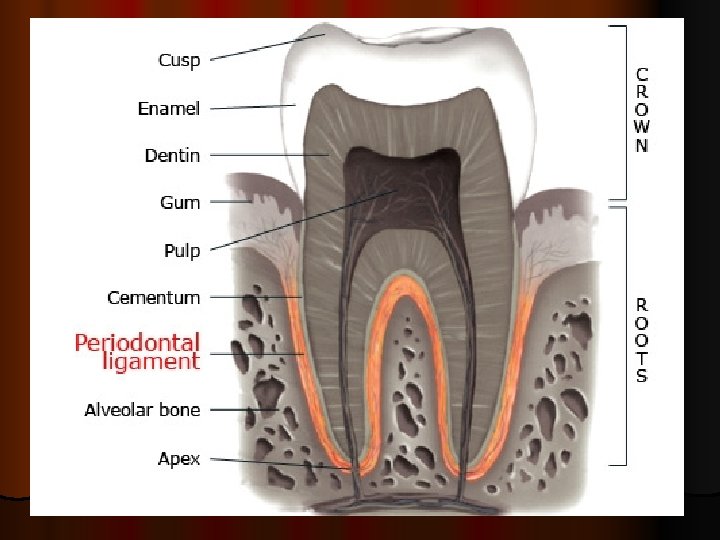
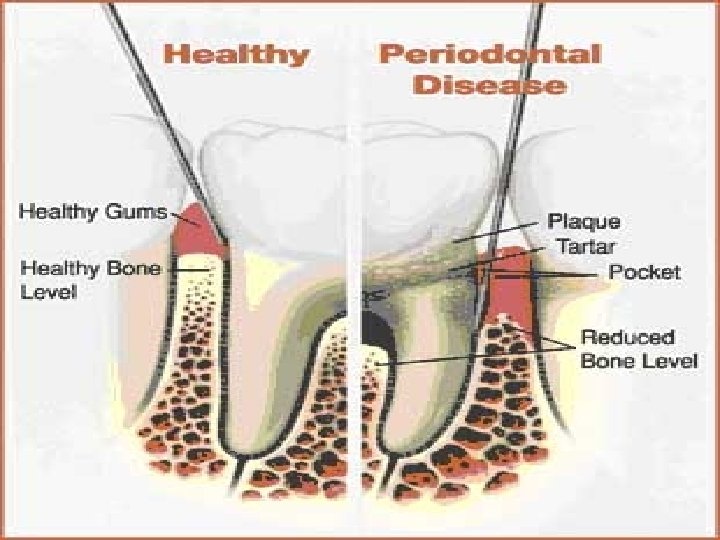
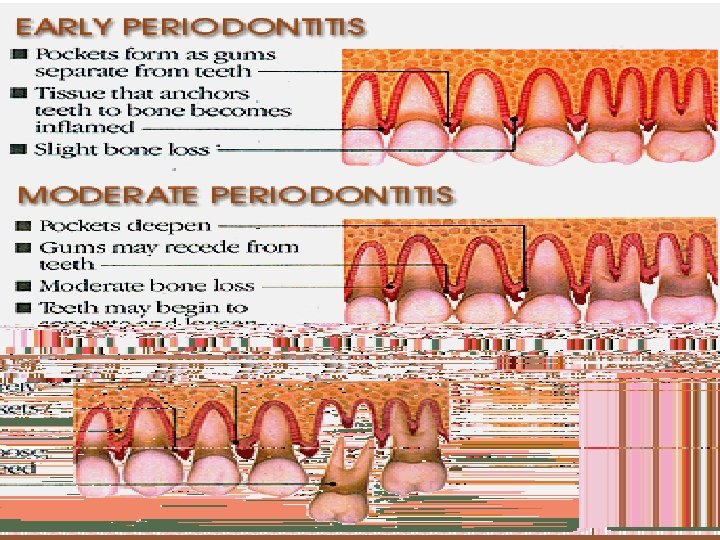
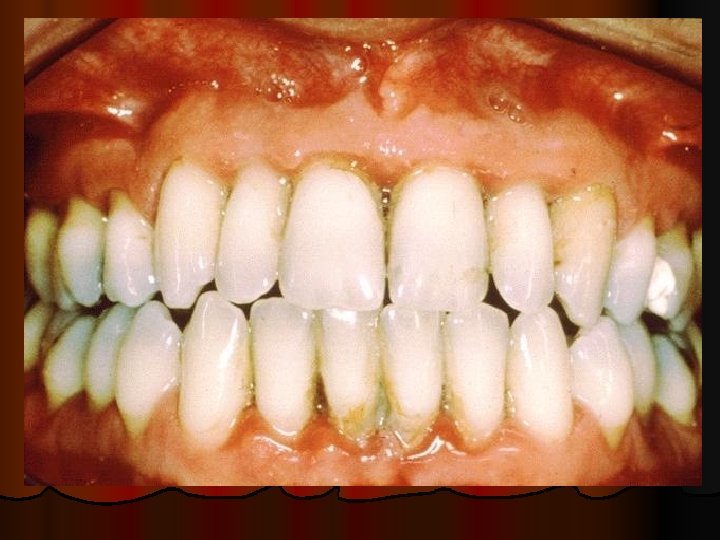
Chronic periodontitis l Causes l Chronic gingivitis l Occlusal trauma l Improper application of orthodontic appliance (excess force) Pathology l Destruction of periodontal ligament l Formation of periodontal pocket l Resorption of alveolar bone l Loosening of teeth
Clinical features l Features of chronic gingivitis l Swollen, soft, discolored l Bleeds on probing l Gingival pocket ( >4 mm) l False pocket if gingiva is elongated towards crown. Recession of gum margin Mobile tooth Halitosis
Management l. Maintain oral hygiene l. Brushing l. Mouth l. Scaling wash to remove plaque and calculi l. Subgingival curettage of pocket, to allow normal reattachment of gingival and periodontal tissue l. Mucogingival flap operation: curettage of granulation tissue, dead bone and cementum beneath a flap of gingiva
Complications l Intraoral and extraoral abscess l Maxillary sinusitis l Ostemyelitis of jaw l Cellulitis of face l Dissemination of infection: bacteremia, septicemia
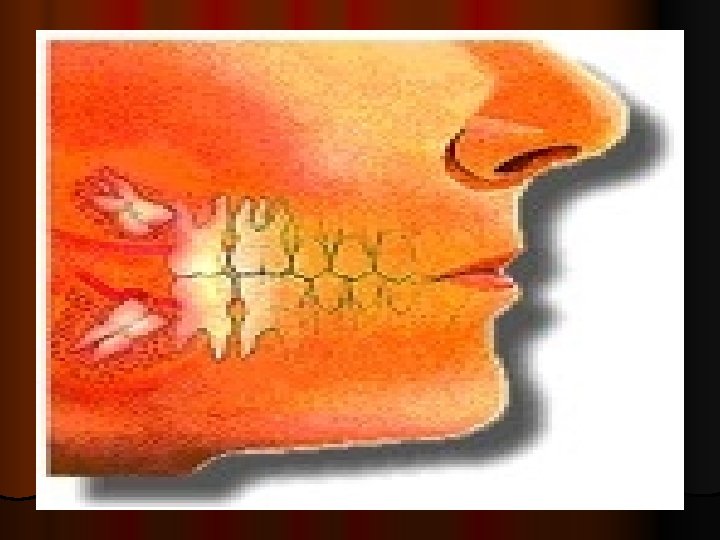
Pericoronitis l Inflammation of the gingival tissue around an erupting tooth l When the eruption is partial, there is an opening through the mucus membrane and l rest of the crown is covered by a flap of gum which is known as operculum l Commonly occurs in the lower 3 rd molar at the age of 18 to 25 yrs l But any tooth can be affected
Causes l Food stagnation and impaction l Upper tooth traumatizing lower gum flap l Vincent’s infection – acute gingivitis caused by borella vincemtis & fuscobacterium l Eruption irritation l Immunocompromised host
Clinical features l Pain l Swollen operculum l Trismus l Halitosis l Fever and enlarged cervical LN l Purulent exudate l Abscess formation
Management l Clean with 3%H 2 O 2 l Nascent O 2 is bactericidal l Normal saline wash l Maintain oral hygiene l Brushing l Antiseptic mouthwash l Chlorhexidine, Betadine, l Soft diet l Analgesic and anti inflammatory l Amoxycillin 500 mg tds for 5 to 7 days Or Erythromycin 250 mg qid for 5 to 7 days l Operculectomy l Removal of upper tooth may be necessary