PERINATAL FOLLOWUPS Seluk ZDEN MD Prof PRENATAL CARE

 is a type of preventive healthcare Allow to")





 that")



 is skin darkening of")









































 negative and are unsensitized")

 The BMI is universally expressed in kg/m 2")

















 During")














- Slides: 91
PERINATAL FOLLOW-UPS Selçuk ÖZDEN MD, Prof
PRENATAL CARE Prenatal care (antenatal care) is a type of preventive healthcare Allow to treat and prevent potential health problems throughout the course of the pregnancy while promoting healthy lifestyles that benefit both mother and child. Optimally begins before conception and extends throughout the postpartum period and interconceptional period.
PRENATAL CARE EFFECTIVENESS Prenatal care contrubuted to: Decreased maternal mortality rate from 690 per 100, 000 births in 1920 to 10 to 15 per 100, 000 in 2015, Lower rates of preterm birth and neonatal death
COMPONENTS OF PRENATAL CARE 1. Preconceptional counseling, 2. Diagnosis of Pregnancy, 3. Initial Prenatal evaluation 4. Subsequent Prenatal Visits
DIAGNOSIS OF PREGNANCY
DIAGNOSIS OF PREGNANCY Symptoms and Signs Amenorrhea Nausea & vomiting Breast changes Fetal movement Elevated basal body temperature Skin changes Pelvic organ changes
SYMPTOMS AND SIGNS Amenorrhea The abrupt cessation of menses in a healthy reproductive-aged female is highly suggestive of pregnancy. Is caused by hormones (estrogen and progesterone) produced by the corpus luteum. Is not a reliable pregnancy indicator until 10 days or more after expected menses.
SYMPTOMS AND SIGNS Nausea & vomiting is a common symptom (50% of pregnancies) that begins as early as 2 weeks’ gestational age, customarily resolves at between 13 and 16 weeks’ gestation. Hyperemesis gravidarum is an extreme form of nausea and vomiting and is characterized by dehydration, weight loss (up to 5%), and ketonuria.
SYMPTOMS AND SIGNS Breast changes Mastodyni: Breast tenderness caused by hormonal changes Breast engorgement: is seen early in pregnancy, especially in primiparous patients. Montgomery’s tubercles are the portion of the areolar glands visible on the skin surface. These tubercles occur as early as 6– 8 weeks’ gestation. Colostrum secretion: may occur during pregnancy as early as 16 weeks’ gestation.
SYMPTOMS AND SIGNS Breast changes
SYMPTOMS AND SIGNS Fetal movement The initial perception: at 18– 20 weeks’ gestation in primiparous patients and as early as 14 weeks’ gestation in multiparous patients. Elevated basal body temperature (BBT): Progesterone produces a 0. 5°F increase in the BBT.
SYMPTOMS AND SIGNS Skin Changes Chloasma (The mask of pregnancy) is skin darkening of the forehead, bridge of the nose, or cheek bones, is linked to genetic predisposition and usually occurs after 16 weeks’ gestation, is exacerbated by sunlight.
SYMPTOMS AND SIGNS Skin Changes Linea nigra: darkening of the lower midline from the umbilicus to the pubis (caused by increased Melanocyte-stimulating hormone. Striae: The striae appear late in pregnancy and are caused by collagen separation.
SYMPTOMS AND SIGNS Pelvic Organ Changes 1. Chadwick’s sign: Congestion of the pelvic vasculature causes bluish discoloration of the vagina and the cervix. 2. Hegar sign: At 6 to 8 weeks’ menstrual age, the firm cervix contrasts with the now softer fundus and the compressible interposed softened isthmus—. 3. Leukorrhea: There is an increase in vaginal discharge, containing epithelial cells and cervical mucous, secondary to hormonal changes.
SYMPTOMS AND SIGNS Hegar sign Leukorrhea
DIAGNOSIS of PREGNANCY A. Fetal Heart Tones are detectable by handheld Doppler (after 10 weeks’ gestation) or by fetoscope (after 18– 20 weeks’ gestation). The normal heart rate is 110– 160 beats per minute, with a higher fetal heart rate observed early in pregnancy.
DIAGNOSIS of PREGNANCY B. Uterine Size/Fetal Palpation From 18 to 34 weeks there is a good correlation between the uterine fundal measurement in centimeters and the gestational age in weeks.
DIAGNOSIS of PREGNANCY B. Uterine Size/Fetal Palpation After 22 weeks, the fetus can be palpated through the maternal abdominal wall (after 22 weeks), and the position can be determined by Leopold’s maneuvers.
DIAGNOSIS of PREGNANCY C. Sonography Gestational sac is the first sonographic evidence of pregnancy. It may be seen with transvaginal sonography by 4 to 5 weeks’ gestation. Yolk sac: a brightly echogenic ring with an anechoic center. It can normally be seen by the middle of the fifth week. Fetal pole: can be seen at fifth week ’ gestation. Cardiac activity is discernible at 5– 6 weeks via transvaginal sonogram
DIAGNOSIS of PREGNANCY D. Pregnancy Tests Pregnancy tests measure changes in the level of human chorionic gonadotropin (h. CG). The β submit of h. CG may be detected in the maternal serum 8– 11 days after conception. β-h. CG levels peak at 10– 12 weeks’ gestation and decrease afterward.
PREGNANCY TESTS 1. Home pregnancy test is performed on the first voided morning urine sample. 2. Urine pregnancy test is the most common method to confirm pregnancy. 3. Serum pregnancy test. β-h. CG can be detected within 7 days after conception or at a menstrual age of 21 days’ gestation.
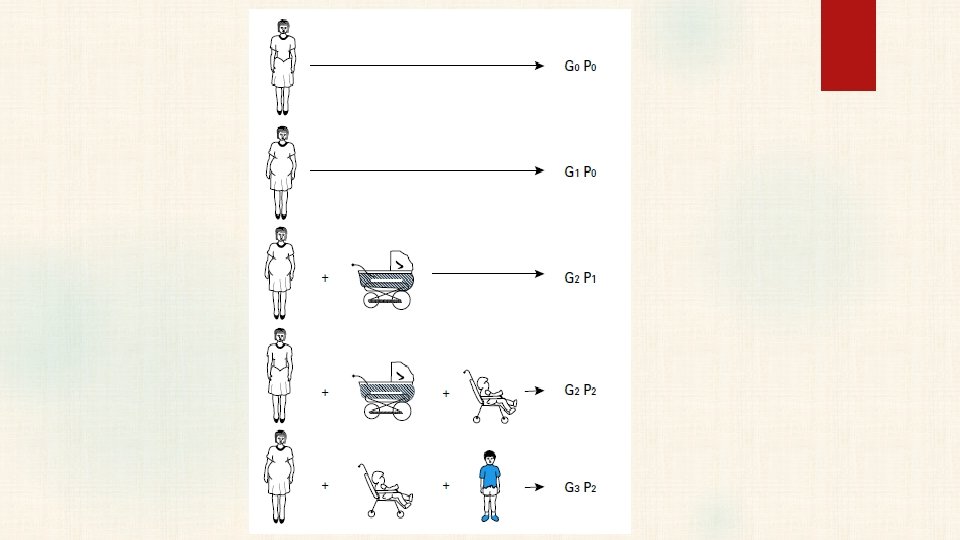
DEFINITIONS Nulligravida—a woman who currently is not pregnant nor has ever been pregnant. Gravida—a woman who currently is pregnant or has been in the past, irrespective of the pregnancy outcome. With the establishment of the first pregnancy, she becomes a primigravida, and with successive pregnancies, a multigravida.
DEFINITIONS Nullipara—a woman who has never completed a pregnancy beyond 20 weeks’ gestation. She may not have been pregnant or may have had a spontaneous or elective abortion(s) or an ectopic pregnancy. Primipara—a woman who has been delivered only once of a fetus or fetuses born alive or dead with an estimated length of gestation of 20 or more weeks. Multipara—a woman who has completed two or more pregnancies to 20 weeks’ gestation or more.
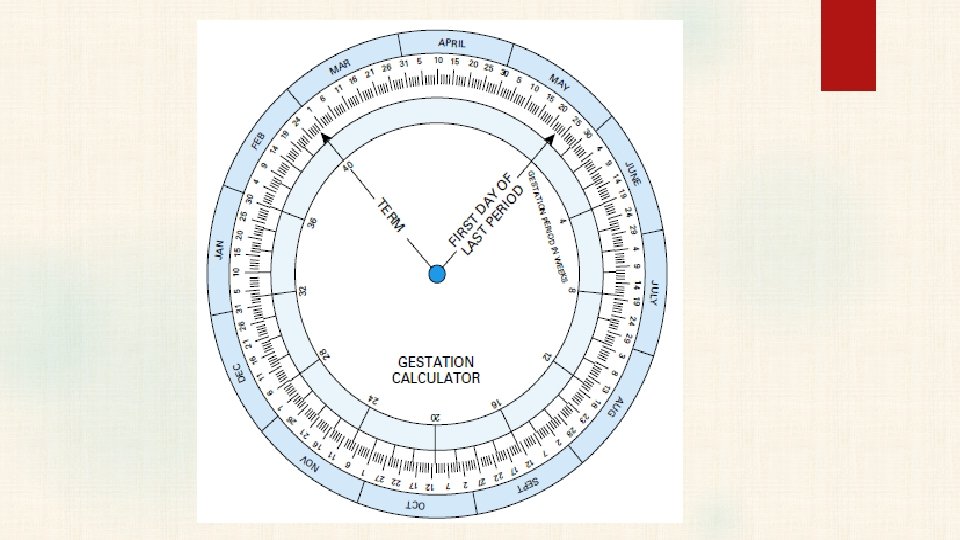
NORMAL PREGNANCY DURATION The mean duration of pregnancy: (calculated from the first day of the last normal menstrual period) is very close to 280 days or 40 weeks. Naegele rule It is customary to estimate the expected delivery date by adding 7 days to the date of the first day of the last normal menstrual period and counting back 3 months. For example, if the last menstrual period began September 10, the expected date of delivery is June 17.
NORMAL PREGNANCY DURATION Because precise knowledge of fetal age is imperative for ideal obstetrical management, the clinically appropriate unit is weeks of gestation completed. Clinicians designate gestational age using completed weeks and days, for example, 334/7 weeks or 33 + 4, for 33 completed weeks and 4 days.
TRIMESTERS Pregnancy duration is divided three equal trimesters. Thus, there are three periods of 14 weeks each. First trimester extends through completion of 14 weeks Second trimester extends through 28 weeks Third trimester includes the 29 th through 42 nd weeks of pregnancy.
INITIAL PRENATAL EVALUATION
INITIAL PRENATAL EVALUATION Major goals are : To define the health status of the mother and fetus, To estimate the gestational age, and To initiate a plan for continuing obstetrical care.
HISTORY Obstetric history Medical history Surgical history Family history
OBSTETRIC HISTORY The interview should include a discussion of current symptoms, Outcomes of all previous pregnancies, § Length of gestation, § Birth weight, § Length of labor, § Type of delivery, § Fetal/neonatal outcome, anesthesia, and any complications occurring in previous pregnancies,
MENSTRUAL HISTORY Last mentruel perid Without a history of regular, predictable, cyclic, spontaneous menses that suggest ovulatory cycles, accurate dating of pregnancy by history and physical examination is difficult. Usage steroidal contraceptives: predicting the time of conception in this circumstance may be erroneous.
MEDICAL HISTORY Cardiovascular, gastrointestinal, and endocrine disorders require careful evaluation and consultation regarding effects on the mother. Prior blood transfusion may increase the risk of hemolytic disease of the newborn because of maternal antibodies produced secondary to a minor blood group mismatch. Medical conditions of particular relevance to pregnancy include diabetes and other endocrine diseases, hypertension, epilepsy, and autoimmune diseases.
SURGICAL HISTORY A history of gynecologic, abdominal, or uterine surgery may necessitate a caesarean section. A history of cervical surgery, multiple induced abortions, or recurrent fetal losses may suggest cervical incompetence.
FAMILY HISTORY A family history of diabetes mellitus should alert the clinician. Familial disorders is also important in pregnancy management. Antenatal screening tests are available for many hereditary diseases. A history of twinning is important
PREVIOUS AND CURRENT HEALTH STATUS Cigarette Smoking Potential teratogenic effects, Placenta previa, placental abruption ↑ Premature membrane rupture ↑ Low-birthweight infant ↑ Sudden infant death syndrome (SIDS) ↑ Spontaneous abortion, fetal death, and fetal digital anomalies ↑
PREVIOUS AND CURRENT HEALTH STATUS Alcohol Ethyl alcohol is a potent teratogen that causes fetal alcohol syndrome characterized by growth restriction, facial abnormalities, and central nervous system dysfunction Women who are pregnant or considering pregnancy should abstain from using any alcoholic beverages.
PREVIOUS AND CURRENT HEALTH STATUS Illicit Drugs Agents may include heroin and other opiates, cocaine, amphetamines, barbiturates, and marijuana. Chronic use of large quantities is harmful to the fetus. Well-documented sequelae include fetal-growth restriction, low birthweight, and drug withdrawal soon after birth.
PREVIOUS AND CURRENT HEALTH STATUS Intimate Partner Violence Is a major public health problem. Most abused women continue to be victimized during pregnancy. The prevalence during pregnancy: 4 -8% Associated adverse perinatal outcomes: Preterm delivery, Fetal-growth restriction, Perinatal death
CLINICAL EVALUATION General physical examination should be completed at the initial prenatal encounter.
CLINICAL EVALUATION Pelvic examination The cervix is visualized employing a speculum To identify cytological abnormalities, a Pap smear is performed Specimens for identification of Chlamydia trachomatis and Neisseria gonorrhoeae are also obtained when indicated.
CLINICAL EVALUATION Bimanual examination is completed by palpation, with special attention given to: § the consistency, length, and dilatation of the cervix; § uterine and adnexal size; § the bony pelvic architecture § any vaginal or perineal anomalies.
GESTATIONAL AGE ASSESSMENT Precise knowledge of gestational age is one of the most important aspects of prenatal care. Gestational age assesment: Last menses, Carefully performed clinical uterine size examination, First-trimester crown-rump length is the most accurate tool.
LABORATORY TESTS Initial blood tests include: Complete blood count, Blood type with Rh status, Antibody screen. Human immunodeficiency virus (HIV) testing, Hepatitis B virus, syphilis, and immunity to rubella Urine culture Cervical culture for Chlamidia trachomatis and N gonorhea
LABORATORY TESTS
PREGNANCY RISK ASSESSMENT High-risk pregnancy Many factors exist that can adversely affect maternal and/or fetal well- being. Some conditions may require the involvement of a maternal-fetal medicine subspecialist, geneticist, pediatrician, anesthesiologist, or other medical specialist in the evaluation, counseling, and care of the woman and her fetus
PREGNANCY RISK ASSESSMENT
SUBSEQUENT PRENATAL VISITS
SUBSEQUENT PRENATAL VISITS Subsequent prenatal visits have been traditionally scheduled Until 28 weeks: at 4 -week intervals, Until 36 weeks, at 2 weeks intervals After 36 weeks: at weekly intervals. Complicated pregnancies: at 1 - to 2 -week intervals.
SUBSEQUENT PRENATAL VISITS At each return visit: The well-being of mother and fetus are assessed, Fetal heart rate, growth, amnionic fluid volume, and activity are evaluated. Maternal blood pressure and weight are assessed. Symptoms such as headache, altered vision, abdominal pain, nausea and vomiting, bleeding, vaginal fluid leakage, and dysuria are sought.
PRENATAL SURVEILLANCE Fundal Height Between 20 and 34 weeks, the height of the uterine fundus measured in centimeters correlates closely with gestational age in weeks This measurement is used to monitor fetal growth and amnionic fluid volume. It is measured as the distance along the abdominal wall from the top of the symphysis pubis to the top of the fundus.
PRENATAL SURVEILLANCE Fetal Heart Sounds The fetal heart rate ranges from 110 to 160 beats per minute and is typically heard as a double sound. Fetal heart is audible by 20 weeks in 80 percent of women, and by 22 weeks, heart sounds were heard in all.
PRENATAL SURVEILLANCE Sonography provides invaluable information regarding fetal anatomy, growth, and well-being,
SUBSEQUENT LABORATORY TESTS Fetal aneuploidy screening may be performed at 11 to 14 weeks and/or at 15 to 20 weeks Serum screening for neural tube defects is offered at 15 to 20 weeks. Hematocrit or hemoglobin determination at 28 to 32 weeks HIV testing in the third trimester for women at increased risk. Hepatitis B at the time of hospitalization for delivery.
SUBSEQUENT LABORATORY TESTS Antibody screening: Women who are D (Rh) negative and are unsensitized should have an antibody screening test repeated at 28 to 29 weeks. Group B Streptococcal Infection Vaginal and rectal group B streptococcal (GBS) cultures be obtained in all women between 35 and 37 weeks’ gestation.
SUBSEQUENT LABORATORY TESTS Gestational Diabetes screening All pregnant women should be screened for gestational diabetes mellitus between 24 and 28 weeks’ gestation , whether by history clinical factors, or routine laboratory testing.
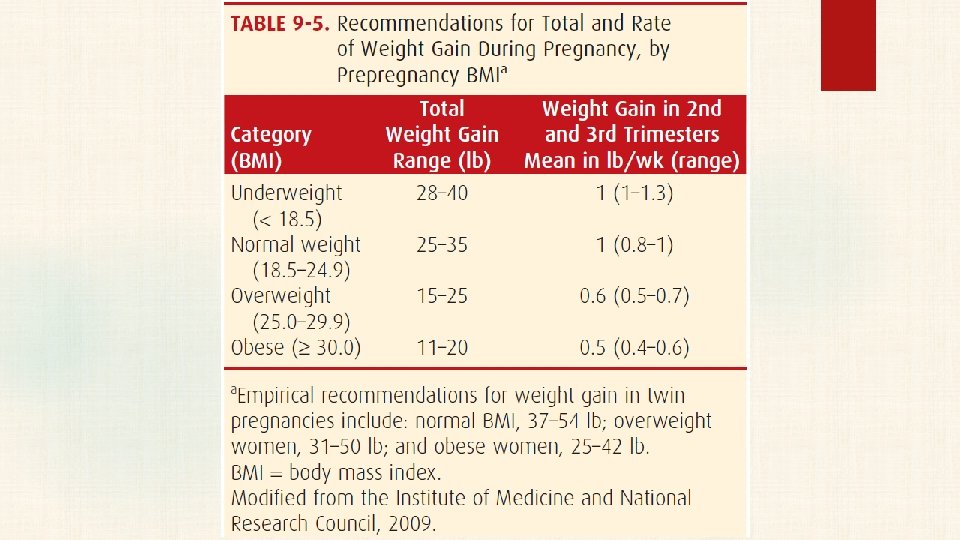
NUTRITIONAL COUNSELING Body mass index (BMI) The BMI is universally expressed in kg/m 2 BMI=Mass(kg)/height (m 2) BMI can easily be calculated with commonly available graphs
NUTRITIONAL COUNSELING Obesity is associated with significantly increased risks for gestational hypertension, preeclampsia, gestational diabetes, macrosomia, cesarean delivery, and other complications. Severe Undernutrition Birthweight can be influenced significantly by starvation during later pregnancy.
NUTRITIONAL COUNSELING Recommended Dietary Allowances The use of excessive supplements has led to concern regarding nutrient toxicities during pregnancy. Those with potentially toxic effects include iron, zinc, selenium, and vitamins A, B 6, C, and D. Excessive vitamin A more than 10, 000 IU per day—may be teratogenic Vitamin and mineral intake more than twice the recommended daily dietary allowance should be avoided.
NUTRITIONAL COUNSELING Calories Pregnancy requires an additional 80, 000 kcal, mostly during the last 20 weeks. To meet this demand, a caloric increase of 100 to 300 kcal per day is recommended during pregnancy Calories are necessary for energy. Whenever caloric intake is inadequate, protein is metabolized rather than being spared for its vital role in fetal growth and development.
NUTRITIONAL COUNSELING Protein Preferably, most protein should be supplied from animal sources, such as meat, milk, eggs, cheese, poultry, and fish. Milk and dairy products have long been considered nearly ideal sources of nutrients,
COMMON CONCERNS Seafood Consumption Fish are an excellent source of protein and contain omega-3 fatty acids. Because nearly all fish and shellfish contain trace amounts of mercury, pregnant and lactating women are advised to avoid specific types of fish with potentially high methyl mercury levels. These include shark, swordfish, king mackerel, and tile fish.
NUTRITIONAL COUNSELING Iron As little as 30 mg of elemental iron provides sufficient iron to meet pregnancy requirements and to protect preexisting iron stores. The pregnant woman may benefit from 60 to 100 mg of elemental iron per day if she is large, has twin fetuses, begins supplementation late in pregnancy, takes iron irregularly, or has a somewhat depressed hemoglobin level. It is not necessary to provide supplemental iron during the first 4 months of pregnancy. .
NUTRITIONAL COUNSELING Iodine The use of iodized salt and bread products is recommended during pregnancy. Severe maternal iodine deficiency predisposes offspring to endemic cretinism, characterized by multiple severe neurological defects. To obviate this, many prenatal supplements now contain various quantities of iodine.
NUTRITIONAL COUNSELING Vitamins The increased requirements for most vitamins during pregnancy usually are supplied by any general diet that provides adequate calories and protein. The exception is folic acid
NUTRITIONAL COUNSELING Folic Acid More than half of all neural-tube defects can be prevented with daily intake of 400 μg of folic acid throughout the periconceptional period. This dose should be consumed as a separate supplement and not as multivitamin tablets. This practice avoids excessive intake of fat- soluble vitamins.
NUTRITIONAL COUNSELING Vitamin A This vitamin has been associated with congenital malformations when taken in higher doses (> 10, 000 IU per day) during pregnancy. Most prenatal vitamins contain vitamin A in doses considerably below the teratogenic threshold. Additional supplementation is not routinely recommended.
NUTRITIONAL COUNSELING Vitamins B 12 Vitamin B 12 occurs naturally only in foods of animal origin, and strict vegetarians may give birth to infants whose B 12 stores are low. Low levels of vitamin B 12 preconceptionally, similar to folate, may increase the risk of neural-tube defects.
NUTRITIONAL COUNSELING Vitamin D deficiency is common during pregnancy. This is especially true in high-risk groups such as women with limited sun exposure, ethnic minorities—particularly those with darker skin, and vegetarians. An adequate intake of vitamin D during pregnancy and lactation was 600 IU per day. In women suspected of having vitamin D deficiency, serum levels of 25 - hydroxyvitamin D can be obtained.
COMMON CONCERNS Employment In the absence of complications, most women can continue to work until the onset of labor. Any occupation that subjects the pregnant woman to severe physical strain should be avoided. Ideally, no work or play should be continued to the extent that undue fatigue develops. Adequate periods of rest should be provided.
COMMON CONCERNS Exercise Pregnant women do not need to limit exercise, provided they do not become excessively fatigued or risk injury. Exercise consisted of treadmill running, step aerobics, or stair stepper use for 20 minutes three to five times each week. Pregnant women should refrain from activities with a high risk of falling or abdominal trauma.
COMMON CONCERNS Automobile and Air Travel Women should be encouraged to wear properly positioned three-point restraints throughout pregnancy while riding in automobiles. Airbags should not be disabled for the pregnant woman. In the absence of obstetrical or medical complications, pregnant women can safely fly up to 36 weeks’ gestation.
COMMON CONCERNS Coitus In healthy pregnant women, sexual intercourse usually is not harmful. Whenever abortion, placenta previa, or preterm labor threatens, however, coitus should be avoided. Intercourse late in pregnancy specifically has not been found to be harmful.
COMMON CONCERNS Dental Care Examination of the teeth should be included in the prenatal examination, and good dental hygiene is encouraged. Periodontal disease has been linked to preterm labor. Importantly, pregnancy is not a contraindication to dental treatment including dental radiographs.
PRENATAL IMMUNISATION Routin Prenatal Immunisations Tetanus toxoid + Diphtheria toxoid, Acellular pertussis (Tdap) During influenza season Inactivated influenza vaccines are routinely recommended during pregnancy. Live vaccines are generally avoided during pregnancy because of a theoretical risk to the fetus. Pregnancy should be avoided for 28 days following administration of a live vaccine.
PRENATAL IMMUNISATION Immunisations for special circumstances Pneumococcal Yellow fever Haemophilus influenzae type b Poliovirus Meningococcal Typhoid Hepatitis B Smallpox Hepatitis A Rabies Antrax
PRENATAL IMMUNISATION Immunisations to Avoid During Pregnancy Human papillomavirus Measles, mumps, rubella LAIV — The live-attenuated influenza vaccine (LAIV) Varicella Tuberculosis MMRV vaccine — A combination Zoster measles, mumps, rubella, and varicella vaccine
COMMON CONCERNS Caffeine consumption Heavy intake of coffee each day—about five cups or 500 mg of caffeine —slightly increases the abortion risk. It is unclear if caffeine consumption is associated with preterm birth or impaired fetal growth.
COMMON CONCERNS Nausea and Vomiting Tend to be worse in the morning— frequently continue throughout the day. Eating small meals at more frequent intervals but stopping short of satiation is valuable. The herbal remedy ginger İs likely effective. Hyperemesis gravidarum—vomiting so severe that dehydration, electrolyte and acid-base disturbances, and starvation ketosis become serious problems
COMMON CONCERNS Backache Low back pain to some extent is reported by nearly 70 percent of pregnant women. It can be reduced by squatting rather than bending when reaching down, by using a pillow back support when sitting, and by avoiding high-heeled shoes.
COMMON CONCERNS Varicosities Susceptible women develop leg varicosities that typically worsen as pregnancy advances, especially with prolonged standing. Treatment is generally limited to periodic rest with leg elevation, elastic stockings, or both. Surgical correction during pregnancy generally is not advised,
COMMON CONCERNS Varicosities and Hemorrhoids are rectal vein varicosities Pain and swelling usually are relieved by topically applied anesthetics, warm soaks, and stool-softening agents. Thrombosis of an external hemorrhoid, may be relieved by incision and removal of the clot under local analgesia.
COMMON CONCERNS Heartburn This symptom is caused by gastric content reflux into the lower esophagus. The increased frequency of regurgitation during pregnancy most likely results from upward displacement and compression of the stomach by the uterus, combined with relaxation of the lower esophageal sphincter.
COMMON CONCERNS Pica The craving of pregnant women for strange foods is termed pica. At times, nonfoods such as ice—pagophagia, starch— amylophagia, or clay—geophagia may predominate. This desire has been considered by some to be triggered by severe iron deficiency.
COMMON CONCERNS Sleeping and Fatigue Beginning early in pregnancy, many women experience fatigue and need increased amounts of sleep. This likely is due to the soporific effect of progesterone Most women experience some degree of sleep disturbance by the third trimester. Daytime naps and mild sedatives at bedtime such as diphenhydramine (Benadryl) can be helpful.
COMMON CONCERNS Leukorrhea Increased mucus secretion by cervical glands in response to hyperestrogenemia is undoubtedly a contributing factor. Occasionally, troublesome leukorrhea is the result of vulvovaginal infection.
COMMON CONCERNS Cord Blood Banking There are two types of cord blood banks. Public banks promote allogeneic donation, for use by a related or unrelated recipient, similar to blood product donation. Private banks were initially developed to store stem cells for future autologous use and charged fees for initial processing and annual storage.
COMMON CONCERNS The likelihood that cord blood would be used for the child or family member of the donor couple is considered remote and estimated to be about 1 in 2700 individuals. It is recommended that directed donation be considered when an immediate family member carries the diagnosis of a specific condition known to be treatable by hemopoietic transplantation.
REFERENCES 1. Cuningham G, Williams Obstetrics, 24 th edition, 2014, Mc. Graw-Hill Education 2. Kevin P. Hanretty. Obstetrics Illustrated, Sixtth ed. Churchill Livingstone, London, 2004 3. Alan H. De. Cherney, , CURRENT Diagnosis & Treatment Obstetrics & Gynecology, 11 th edition, The Mc. Graw-Hill Companies, 2013 4. Creasy And Resnik’s Maternal-fetal Medicine, Seventh Edition, Elsevier saunders, 2014