PENYAKIT JANTUNG DAN KEGAWATANNYA PADA BAYI DAN ANAK

PENYAKIT JANTUNG DAN KEGAWATANNYA PADA BAYI DAN ANAK Prof. DR. Dr. Teddy Ontoseno, Sp. AK, Sp. JP, FIHA


Pediatric emergencies • • • • PEDIATRIC CARDIAC ARREST PEDIATRIC BRADYCARDIA PEDIATRIC WIDE COMPLEX TACHYCARDIA PEDIATRIC NARROW COMPLEX TACHYCARDIA PEDIATRIC RESPIRATORY DISTRESS PEDIATRIC RESPIRATORY ARREST PEDIATRIC SHOCK PEDIATRIC ALLERGIC REACTION/ANAPHYLAXIS PEDIATRIC SEIZURES PEDIATRIC ALTERED LEVEL OF CONSCIOUSNESS PEDIATRIC TOXIC EXPOSURES/INGESTIONS PEDIATRIC HEAT EMERGENCIES PEDIATRIC COLD EMERGENCIES PEDIATRIC NEAR DROWNING
 B. Progresivitasnya : lambat/cepat C. Derajatnya")
KELUHAN UTAMA A. Kapan : sejak lahir (bawaan) B. Progresivitasnya : lambat/cepat C. Derajatnya : gangguan terhadap aktivitasnya. D. Pencetusnya : ada/tidak E. Respons terhadap pengobatan D. Keluhan penyerta

TAMPILAN KLINIS KEGAWATAN DARURATAN JANTUNG PADA ANAK 1. SIANOSIS 2. TAKIPNEA 3. PENURUNAN PERFUSI / RENJATAN 4. KOMBINASI

APA YANG HARUS DICARI ? 1. AKIBAT ALIRAN DARAH KE PARU YANG MENURUN (SIANOSIS ± TAKIPNEA) 2. AKIBAT ALIRAN DARAH KE PARU YANG MENINGKAT ( SESAK / DYSPNEA) 3. AKIBAT PENURUNAN CURAH JANTUNG (GANGGUAN PERFUSI PERIFER)

GAGAL JANTUNG

Preload Afterload Heart rate Contractility


NORMAL CIRCULATION

Faktor yang mempengaruhi curah jantung Figure 20. 20

Faktor yang mempengaruhi volume sekuncup Figure 20. 23

Ringkasan pengaruh terhadap curah jantung Figure 20. 24

Determinants of Ventricular Function CONTRACTILITY PRELOAD AFTERLOAD STROKE VOLUME - Synergistic contraction - Valvular competence HEART RATE CARDIAC OUTPUT

Hemodynamics Interelationship Textbook of Pediatric Advanced Life Support, 2003

Arterial Blood Pressure • Determinants of systolic blood pressure 1. Volume of blood ejected 2. Compliance of arterial wall 3. Rate of run-off (resistance) • Determinants of diastolic blood pressure 1. Volume of blood remained 2. Compliance of arterial wall 3. Peripheral resistance

Venous Blood Pressure • Determinants of venous pressure 1. Blood volume 2. Pressure-volume characteristics of venous bed (compliance) 3. Size of venous bed (capacitance) 4. Ability of heart to eject venous return • Location of venous blood volume 1. Peripheral vein ; 65% 2. Pulmonary venous system ; 5%

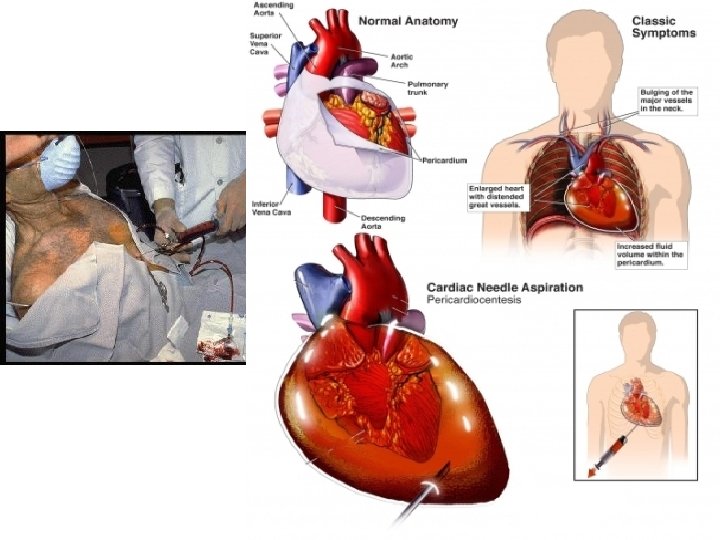
CARDIAC TAMPONADE

Tamponade- A true emergency • Phase I: – accumulation of pericardial fluid causes increased stiffness of the ventricle, requiring a higher filling pressure. RV filling pressures are higher than the intrapericardial pressure. • Phase II: – further fluid accumulation, the pericardial pressure increases above the ventricular filling pressure reduced cardiac output. • Phase III: – A further decrease in cardiac output occurs, which is due to equilibration of pericardial and (LV) filling pressures.


Pericardiocentesis

CARDIAC DYSRHTMIA
 0. 1 m. L/kg (0. 01 mg/kg) OR")
Asystole Epinephrine IV/IO (1: 10, 000) 0. 1 m. L/kg (0. 01 mg/kg) OR Epinephrine ET (1: 1000) 0. 1 m. L/kg (0. 1 mg/kg) ↓ Atropine 0. 02 mg/kg (min 0. 1 mg) max 0. 04 mg/kg
")
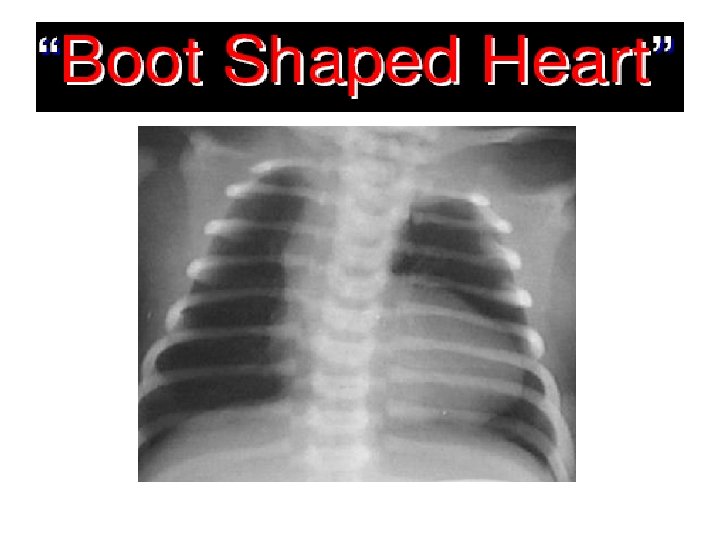
Congenital Heart Lesions that DECREASE Pulmonary Arterial Blood Flow (CYANOTIC)

Recognition is KEY • Cyanosis - is the bluish color of the skin resulting from the presence of at least 5 g/d. L of reduced hemoglobin in the capillary beds – Peripheral cyanosis (most common) related to sluggish blood flow through capillaries and is UNASSOCIATED with cardiac or pulmonary disease. • Common with cold exposure - improves with warming or movement of infant

Recognition is KEY – Central cyanosis results from an abnormality in the oxygen transport – Reflects inadequate oxygenation When severe maybe associated with ↓ oxygen supply to the brain→ hypoxic spells – Central cyanosis DOES NOT improve with warming, may increase with movement → involves trunk, extremities and mucous membranes

CARDIAC CYANOSIS 1. Kebiruan mukosa mulut, lidah, kelopak mata, yang bertambah jelas saat menangis. 2. Tidak timbul segera setelah lahir 3. Takipnea dengan / tanpa distres pernafasan 4. Suhu tetap hangat. 5. Tes hiperoksia positip AWAS : anemia, pigmen kulit, hipotermi, asfiksia

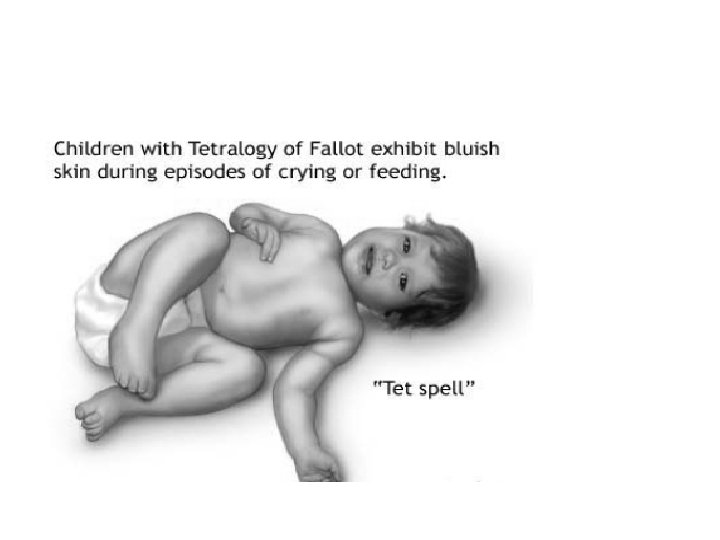
Hypercyanotic spell • a. k. a. “Tet spell”, “paroxysmal hyperpnea” • Etiology uncertain – “Infundibular spasm” – Decrease in systemic vascular resistance • Goal of therapy is to increase pulmonary blood flow

Nursing Considerations • Do not interfere if child is squatting • Organize care to decrease child’s energy expenditure • Administer oxygen as needed • Meet needs quickly; prevent crying • Use soft nipples to decrease energy of sucking
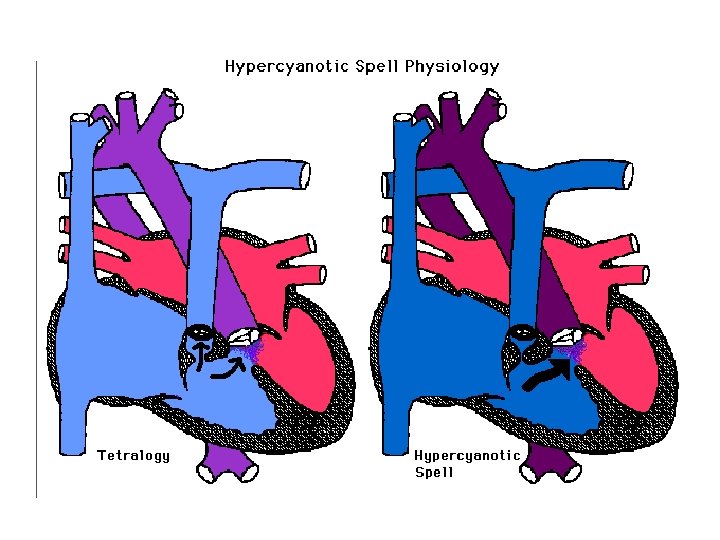


PVR

SVR

Recognition of hypercyanotic spell • Symptoms include: irritability, crying, loss of consciousness • Physical examination may demonstrate tachypnea, deepening of cyanosis, and loss of systolic ejection murmur • Laboratory data would reveal metabolic acidosis

Treatment • • Knee-chest positioning Morphine, 0. 1 -0. 2 mg/kg IV or SC Oxygen (perhaps limited value) Intravenous volume expansion, 10 cc/kg isotonic Sodium bicarbonate 1 -2 m. Eq/kg/dose Propanolol, 0. 15 -0. 25 mg/kg IV over 2 -5 minutes Phenylephrine, 0. 1 mg/kg IM or SC General anesthesia

SHOCK/RENJATAN

Shock Syndromes • Hypovolemic Shock – blood VOLUME problem • Cardiogenic Shock – blood PUMP problem • Distributive Shock [septic; anaphylactic; neurogenic] – blood VESSEL problem

Cardiogenic Shock • Low CO and high systemic vascular resistance • Result of primary cardiac dysfunction: } A compensatory increase in SVR occurs to maintain vital organ function } Subsequent increase in LV afterload, LV work, and cardiac oxygen consumption } CO decreases and ultimately results in volume retention, pulmonary edema, and RV failure

Cardiogenic Shock Etiologies • Congenital heart disease • Arrhythmias • Ischemic heart disease • Myocarditis • Myocardial injury • Acute and chronic drug toxicity • Late septic shock • Infiltrative diseases – mucopolysaccharido ses – glycogen storage diseases • Thyrotoxicosis • Pheochromocytoma

Cardiogenic Shock • Initial clinical presentation can be identical to hypovolemic shock • Initial therapy is a fluid challenge • If no improvement or if worsens after giving volume, suspect cardiogenic shock • Usually need invasive monitoring, further evaluation, pharmacologic therapy • Balancing fluid therapy and inotropic support can be very difficult. – Call an intensivist and/or a cardiologist

Cardiogenic Shock PCWP < 18 mm. Hg PCWP > 18 mm. Hg Expand Blood Volume Inotropic drug Diuretic Vasodilator Mechanical Asst.





Cardiovascular Changes in Shock Type Preload Afterload Contractility Cardiogenic Hypovolemic Distributive early late No change Septic

Infections and cardiovascular disease
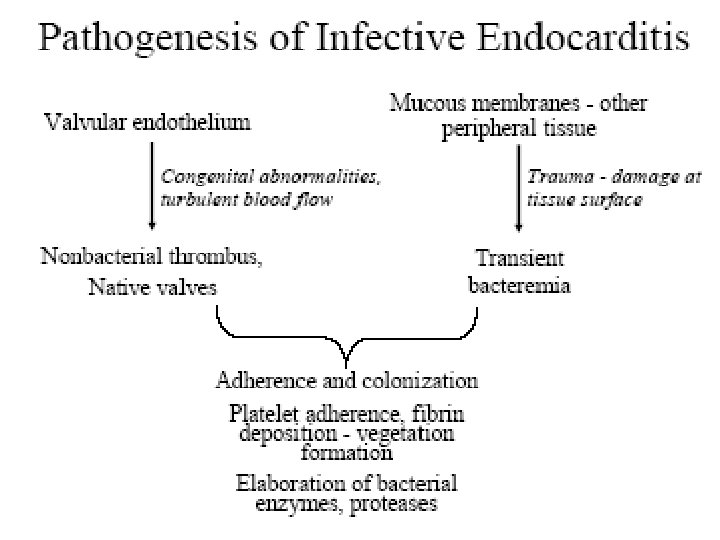


Prevention of bacterial endocarditis


Rheumatic fever
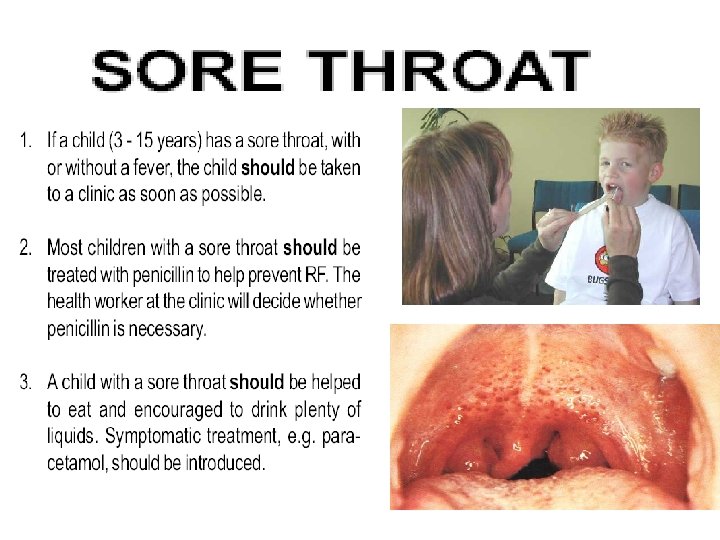
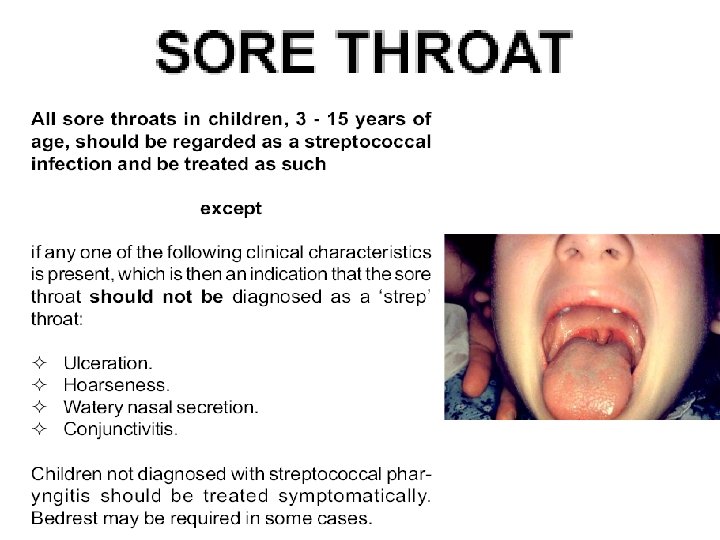
 streptococcal")
Rheumatic Fever: Definition: • • Autoimmune Multisystem Inflammatory disorder Following group A, (ßhemolytic) streptococcal pharyngitis.

ETIOLOGY Capsule Cell wall Protein antigens Group carbohydrate Peptidoglycan Cyto. membrane Cytoplasm Antigen of outer protein cell wall of GABHS induces antibody response in victim which result in autoimmune damage to heart valves, sub cutaneous tissue, tendons, joints & basal ganglia of brain

AETHIOPATHOGENESIS A. Only infections GABHS of the pharynx initiate or reactivate RF. B. Rheumatogenic strains of GABHS M types l, 3, 5, 6, 18 & 24 have antigenic domains similar to antigens in components of the human heart C. Anti-M antibodies against the streptococci may cross-react with heart tissue, causing the pancarditis that is observed in RF.

Clinical Features: • Acute Rheumatic Fever – Acute Inflammatory Phase – Heart – Pancarditis (40 -50%) – Skin – Erythema Marginatum/ S. nodule (10%) – CNS – Sydenham Chorea (15%) – Migratory polyarthritis (75%) • Chronic Rheumatic Fever – Deforming fibrotic valvular disease.


The Jones Criteria for Rheumatic Fever, Updated 1992 • Major Criteria – – – • Minor Criteria Carditis Migratory polyarthritis Sydenham's chore Subcutaneous nodules Erythema marginatum plus – Clinical • fever • Arthralgia – Laboratory • Elevated acute phase reactants • Prolonged PR interval Ø Supporting evidence of a recent group A streptococcal infection • positive throat culture or • rapid antigen detection test; and/ or elevated or • increasing streptococcal antibody test (e. g. , anti-streptolysin O, anti-deoxyribonuclease B, anti-hyaluronidase).
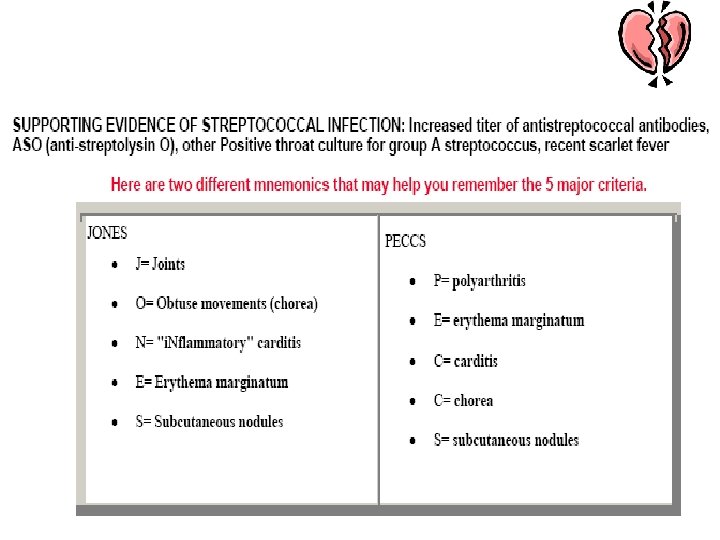

Major criteria of Jones Help to remember : CAPOCHES Carditis Polyarthritis Chorea Erythema Marginatum Subcutan nodule

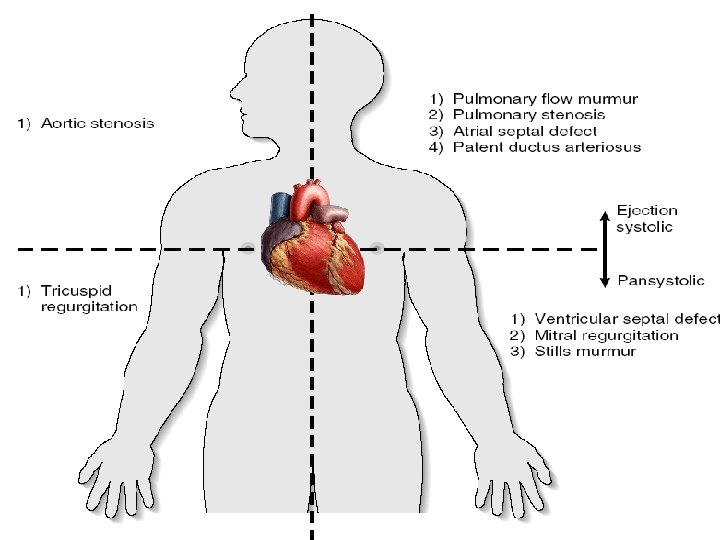
Carditis of ARF • Pancarditis • 40 and 60% of patients with ARF • Characterised by – sinus tachycardia, –Organic cardiac murmurs not previously present (mitral regurgitation) – pericardial friction rub – cardiomegaly – prolonged PR interval and evidence of heart failure may be present – nonspecific

Carditis • Course : mild – fulminant • Onset : first 3 weeks of illness • Cardiac enzymes: normal or minimally elevated

Subcutaneous nodules • Rarely seen and when present • Usually associated with severe carditis. • Painless, firm, movable, measuring around 0. 5 to 2 cm. • Located over extensor surfaces of the joints, particularly knees, wrists and elbows

Erythema Marginatum erythematous lesions with pale centers and rounded or serpiginous margins

Rheumatic Valve Disease: • Gross: – Leaflet thickening – Commissural fusion – Shortening, Thickening & fusion of chordae tendinae. • Microscopic: – Fibrosis – Neovascularisation – Calcification • Mitral 68%, Mitral+Aortic 25%, • 99% of Mitral stenosis is due to RHD.

Acute Rheumatic vegetations:

Valvulitis Aortic valve showing active valvulitis. The valve is slightly thickened and displays small vegetations – "verrucae"

Valve Pathology: Rheumatic SLE Thrombotic Infective

Mitral regurgitation • Apical blowing holosystolic murmur Pure rheumatic MR due to shortening of valve cusps and of papillary muscles chordae tendineae that become matted and adherent to the valve.

Chronic RHD: • Valve leaflet thickening. • Shortening, thickening and fusion of tendinous cords.

Mitral Stenosis • Apical diastolic rumbling murmur • Almost always caused by previous rheumatic fever • Rheumatic fever cause – *a chronic process of valvular fibrosis – *commissures are fused – * the cusps are severely thickened – *calcification with shortened, thickened chordae tendineae

Laboratory Investigations: No specific laboratory investigations I. Acute phase reactant (CRP, SAA, SAP, Complements, Coagulation Proteins) 2. Serologis and bacteriologis (ASO, Anti-DNAse B titres, Culture) 3. Electrocardiography, radiology, echocardiograpphy

RADIOLOGIS

RADIOLOGIS Same patient after 4 weeks

Treatment The reduction of inflammation with anti-inflammatory medications such as aspirin or corticosteroids. Individuals with positive cultures (? ) for strep throat should also be treated with antibiotics.

Treatment • Another important cornerstone in treating rheumatic fever includes the continuous use of low dose antibiotics (such as penicillin, sulfadiazine, or erythromycin) to prevent recurrence.

Plan Of Action • Step 0 : Primordial prevention • Step I : Primary prevention (eradication of streptococci) • Step II : anti inflammatory treatment (aspirin, steroids) • Step III : supportive management & management of complications • Step IV : Secondary prevention (prevention of recurrent attacks)

Plan of Action Step o : Primordial prevention Pharyngitis GABHS strain 1, 3, 5, 6, 18, 24 Step I : Primary prevention Latent periode Rheumatic Fever (by Jones criteria) Step II : Anti inflammation Step III : supportive and complications management Step IV : Secondary prevention Carditis + Carditis – (Mur-mur, Pericarditis, Tacycardia) Mild Mod Severe Cardiomegali + + MR gr 2 >2 >2 CHF -
 Agent Dose Benzathine")
STEP I: Primary Prevention of Rheumatic Fever (Treatment of GABHS Tonsillopharyngitis) Agent Dose Benzathine penicillin G Mode Duration 600 000 U for patients Intramuscular 27 kg (60 lb) 1 200 000 U for patients >27 kg Once or Penicillin V Children: 250 mg 2 -3 times daily Oral (phenoxymethyl penicillin) Adolescents and adults: 500 mg 2 -3 times daily 10 d For individuals allergic to penicillin Erythromycin: 20 -40 mg/kg/d 2 -4 times daily (maximum 1 g/d) Oral 10 d Estolate Oral 10 d or Ethylsuccinate 40 mg/kg/d 2 -4 times daily (maximum 1 g/d) Recommendations of American Heart Association

 Agent Dose")
STEP IV : Secondary Prevention of Rheumatic Fever (Prevention of Recurrent Attacks) Agent Dose Benzathine penicillin G Mode 1 200 000 U every 4 weeks* Intramuscular 250 mg twice daily Oral or Penicillin V or Sulfadiazine 0. 5 g once daily for patients 27 kg (60 lb 1. 0 g once daily for patients >27 kg (60 lb) Oral For individuals allergic to penicillin and sulfadiazine Erythromycin 250 mg twice daily *In high-risk situations, administration every 3 weeks is justified and recommended Recommendations of American Heart Association Oral

Duration of Secondary Rheumatic Fever Prophylaxis Category Duration Rheumatic fever with carditis and residual heart disease (persistent valvar disease*) At least 10 y since last episode and at least until age 40 y, sometimes lifelong prophylaxis Rheumatic fever with carditis but no residual heart disease valvar disease*) 10 y or well into adulthood, whichever is longer (no Rheumatic fever without carditis 5 y or until age 21 y, whichever is longer *Clinical or echocardiographic evidence. Recommendations of American Heart Association
 initially treat GABHS pharyngitis •")
The roles for antibiotics in Rheumatic Fever • (1) initially treat GABHS pharyngitis • (2) prevent recurrent streptococcal pharyngitis, RF, and RHD • (3) provide prophylaxis against bacterial endocarditis.

Prevent bacterial endocarditis • Alternate drugs recommended by the American Heart Association for these patients include oral clindamycin (children: 20 mg/kg; adults: 600 mg) and oral azithromycin or clarithromycin (children 15 mg/kg; adults: 500 mg)
 or stenosis (chronic RF). * Atrial")
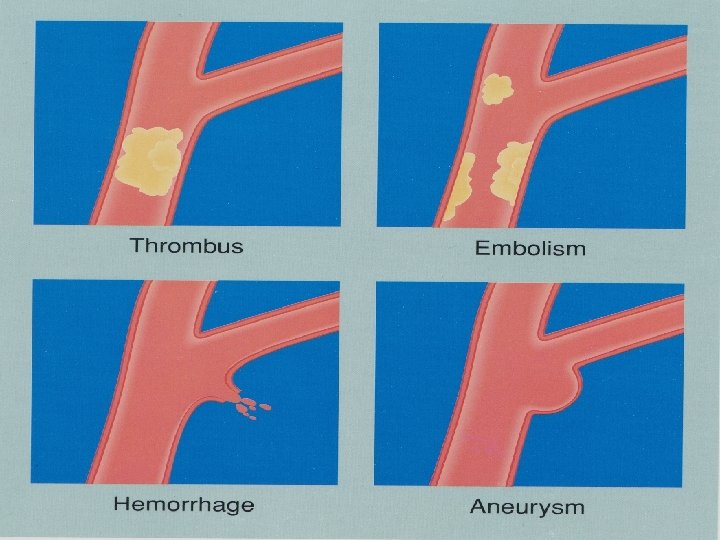
Complications: * CHF from valve insufficiency (acute RF) or stenosis (chronic RF). * Atrial arrhythmias * Pulmonary edema * Recurrent pulmonary emboli * Infective endocarditis * Thrombus formation * Systemic emboli.

- Slides: 101