PELVIC OBLIQUITY Mohahad osman MD Assist prof Zagazig


PELVIC OBLIQUITY Mohahad osman, MD Assist. prof. Zagazig University
 A- PO is failure of the pelvis to")
Definition of Pelvic Obliquity ( PO) A- PO is failure of the pelvis to lie in a perfectly horizontal position in the frontal plane; interspinous line is not perpendicular to midline of body provided that legs are parallel to midline of body. B- 3 -D definition : any fixed malalignment bet. Spine & pelvis, in frontal, sagittal, horizontal or all these 3 planes.
 : 1 - Functional / non-structural PO :")
CLASSIFICATIONS of PO. I- Mayer (1936) : 1 - Functional / non-structural PO : - present only when pt. stands with knees straight & no lift under foot & disappear on sitting & on recumbency w legs parallel to midline of body - due to LLD. 2 - Structural / fixed PO : -persists in all positions & cannot be passively corrected. -Aetiology: a- infrapelvic (hips) c-suprapelvic ( spine) b- pelvic d- combined
 II- Dubousset ( 1991) : 1 - Regular")
Classifications of PO. ( cont. ) II- Dubousset ( 1991) : 1 - Regular PO : spine & pelvis in same directions of deformity. 2 - Opposite PO : in opposite directions.

INFRA-PELVIC FIXED PO. A- Congenital hip contracture: 1 - cong. Abductor contracture 2 - cong. Adduction contracture B- neuromuscular hip contractures : abd, add or both. SUPRA-PELVIC FIXED PO. : - in cong. or neuromuscular scoliosis - not in idiopathic scoliosis ( curve not extend to pelvis )

DISABILITY & SEQUILAE of PO. A- locomotor: Interferes w sitting, standing balance & walking. B- 2 ry. Deformities : * spinal : L. scoliosis( cause / result). Increased L. lordosis. * hip : Abd / add contractures. * knee : hyperextension on long side * apparent LLD. C- decubitus ulceration: ischial / G. trochanter on lower side.

DIAGNOSIS & ASSESSMENT OF PO. HISTORY GENERAL EXAM. : * CARDIOPULMONARY FUNCTION * Gait : - short leg limp ( dipping gait) - Trendlenburg gait EXAM OF DEFORMITY : * inspection * palpation

EXAM for FIXED DEFORMITY: a- Pelvic obliquity: * Oblique pelvis : interspinous line is not perpendicular to midline of body provided that legs are parallel to midline of body * functional PO. ; present only when pt. stands with knees straight & no lift under foot & disappear on sitting & on recumbency w legs parallel to midline of body * fixed PO. : persists in all positions & cannot be passively corrected 1 - infra-pelvic; overcomed by swining legs to one side or other while recumbent. 2 - supra-pelvic; never.
: B- Scoliosis: * trunk alignment : plumb line")
EXAM for FIXED DEFORMITY ( cont): B- Scoliosis: * trunk alignment : plumb line * type of curve * flexibility / rigidity of curve * rotation * neurologic exam. * clinical photographs. C- Fixed hip def. : abd, add, flexion , rotation

ROM : hip. Spine. Knee. Ankle. NEUROLOGIC EXAM: - Power sensation - specific muscles ( hip / trunk) MEASUREMENTS : - PO. - LLD ( app / true) - circumference. SPECIAL TESTS : - iliotibial band - hip instability. -

Ober test

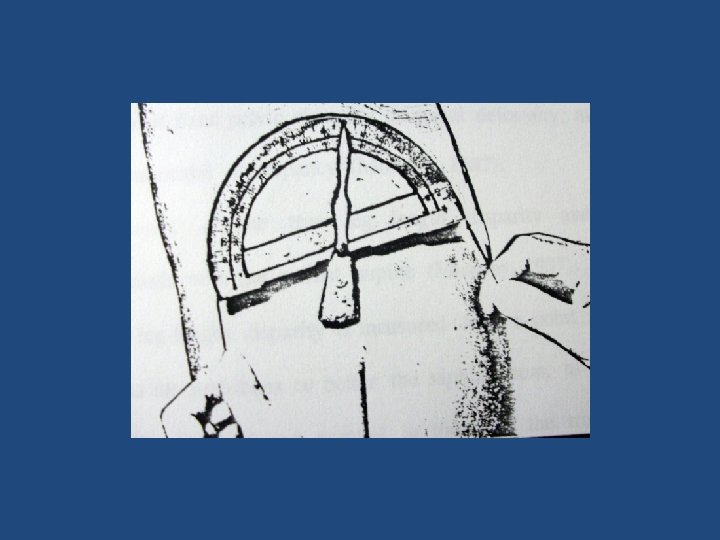
RADIOLOGIC ASSESSMENT A- Pelvic obliquity : * diagnosis of PO. : - in frontal plane - 3 -D * Angle of PO: Osebold , 1982
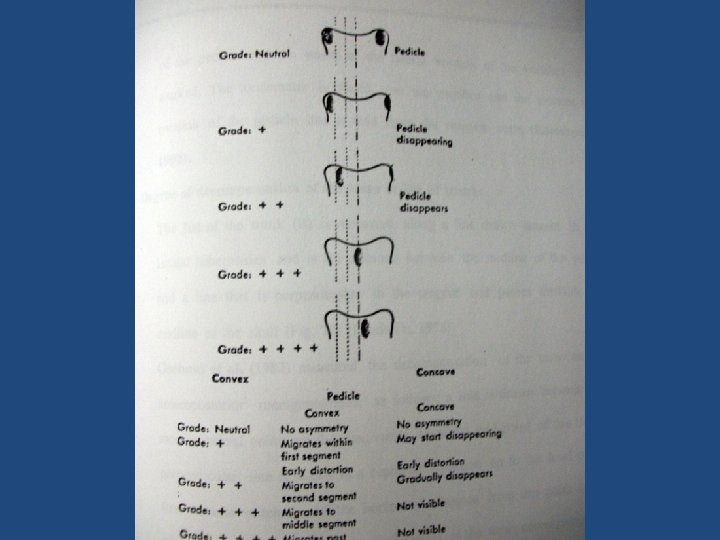
 B- rotation ( pedicles displac. ) C-")
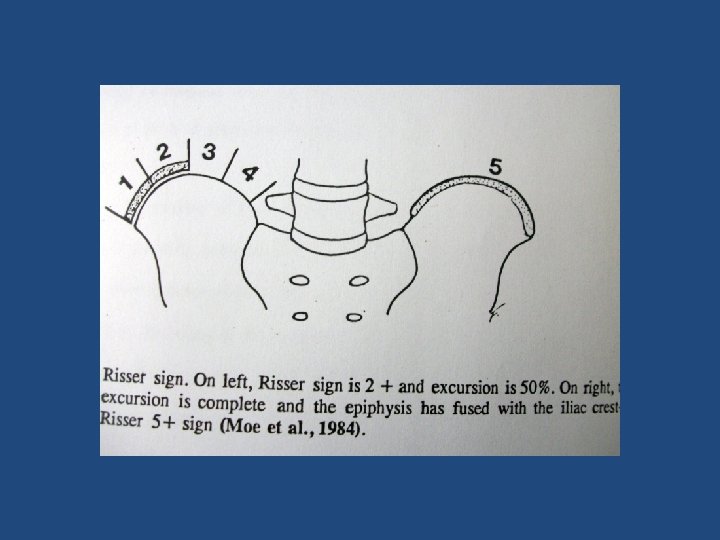
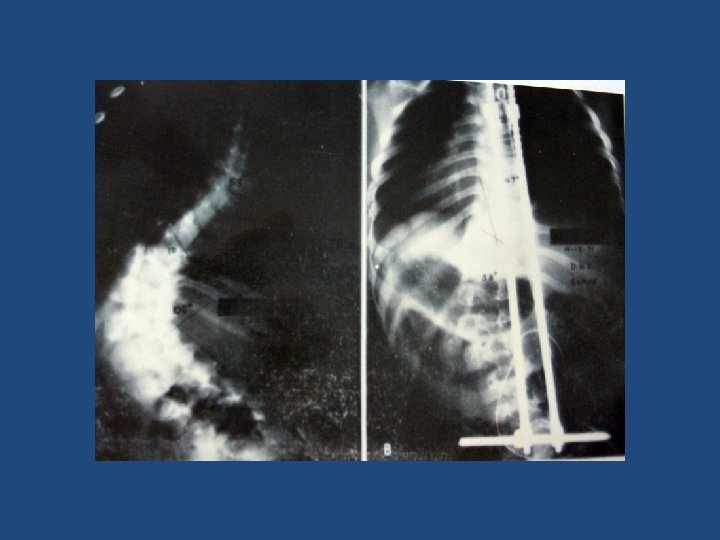
B- Scoliosis: A- Angle ( Cobb ) B- rotation ( pedicles displac. ) C- c rigidity : - side bending - traction D- Torso decompensation: Osebold E- Pt. maturation : Risser sign LORDOSIS SPINA BIFIDA 2 ry changes in hips CT MRI - suspension

A- side-bending XR B- suspension XR A B C- traction XR C

Torso decompensation / trunk list

C- MEASUREMENT of LEG LENGTH -Plain X- ray: scanogram - CT OTHER INVESTIGATIONS: * cardiopulmonary * Biochemical ; ms dystrophy

TREATMENT TTT of PO is directed to the specific cause Ttt of functional PO: - by leg length balancing - up to 3 cm LLD ; shoe lift - > 20 cm LLD; orthosis - 3 -20 cm LLD; shortening, lengthening or both. * correct bony def. or jt. Contracture 1 st.

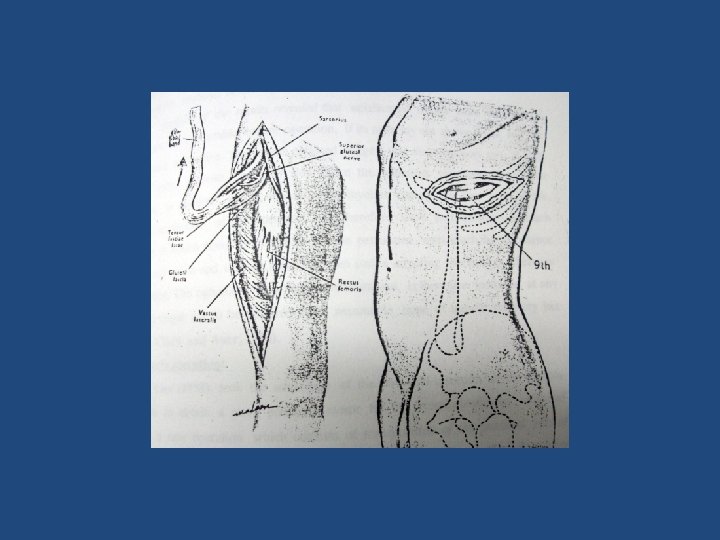
TTT of infra-pelvic type: A- cong hip contractures: - early ; stretching / traction and spica casting - neglected ; surgical release & splinting. B- Paralytic hip contractures ; surgical - abd contracture by ; 1 - soft tissue release ( prox & distal). 2 - STR+ erector spinae transplant or 3 - STR+ intertroch. femoral osteotomy ; > 3 y old, severe, 3 -D - add contracture ;

TTT of supra-pelvic type A- Abdominal fascial plastic operations B- Muscle- tendon transplant operations C- Spinal surgery.

Spinal surgery : Objective: correction of def. to the point at which pelvis is level & then fusion of spine & pelvis in that corrected position. Methods : A- Post. Surgery only; if pelvis can be levelled by passive bending / traction * Harrington sacral bar * Luque * recent segmental instrumentations B- Combined ant. & post. Surgery ; if pelvis can not be levelled by passive bending / traction or deficient post. elements * ant correction& fusion without instrumentation * ant correction& fusion with instrumentation ( Dwyer system).

TTT of combined type A- correct hip & knee def. 1 st then spinal fusion, otherwise spinal def will recur [ Barr, 1950 & Turek, 1984] B- Beaty [1992]; when PO is moderate & L. scoliosis is fixed , correct scoliosis w instrumentation 1 st.

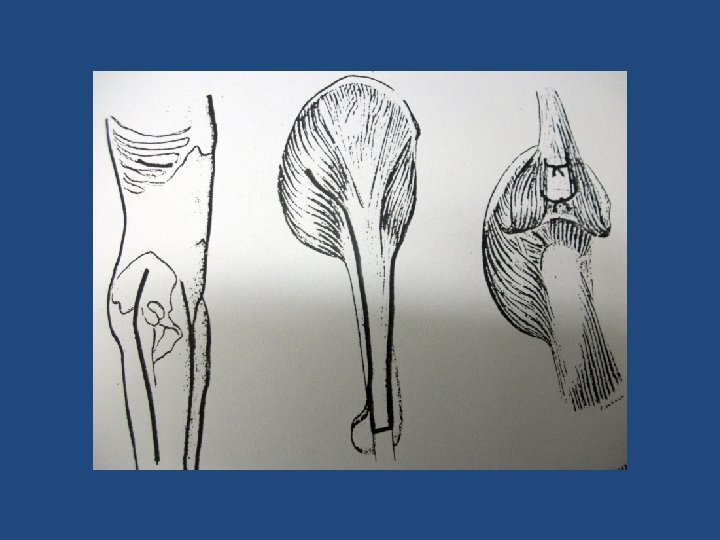
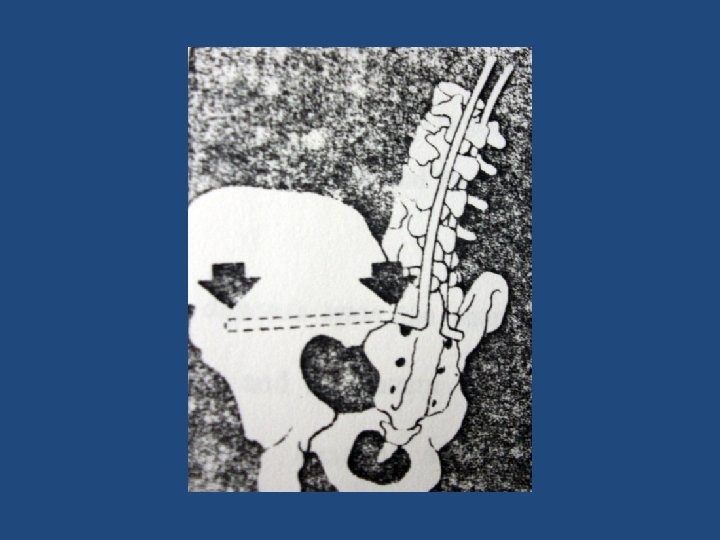
TTT of PO that cannot be corrected by hip / spinal surgery INDIC. : 1 - 2 ry osseous hip changes or 2 ry arthritic changes in L spine rendering full correction impossible. 2 - residual significant fixed PO [ 18 deg] METHODS: 1 - LL realigning to trunk by femoral osteotomy 2 - post iliac osteotomy [ Lindseth, 1978]; compensating pelvic def. placing isch tuberosities & acetabla in planes perpendicular to long axis of body 3 - ischium excision; partial / complete
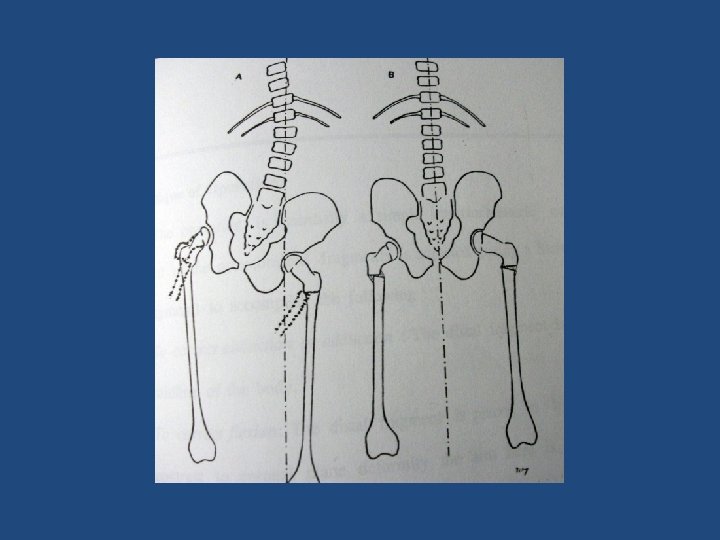
![post iliac osteotomy [ Lindseth, 1978];](http://slidetodoc.com/presentation_image_h2/8eac76eaff6057595599fd31fcfa7ee2/image-32.jpg "post iliac osteotomy [ Lindseth, 1978];")
post iliac osteotomy [ Lindseth, 1978];
- Slides: 32