PEG TUBE PLACEMENT IN ELDERLY PATIENTS STEPHANIE CHUANG

PEG TUBE PLACEMENT IN ELDERLY PATIENTS STEPHANIE CHUANG REBECCA VALDESUSO JETLY KAMARA PATRICIA OBENG

Learning Objectives Upon completion of this presentation, readers will be able to: 1. Develop basic understanding about PEG Tubes. 2. Identify the common reasons for PEG tube placements. 3. Identify the common complications associated with PEG Tubes. 4. Identify some ethical issues that are related to PEG feeding tubes placement.

TARGET AUDIENCE Patients Families Primary Caregivers

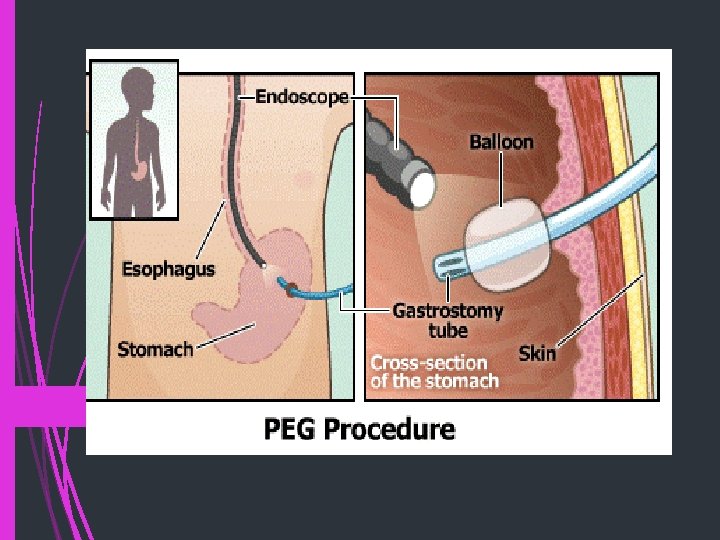
BASIC DEFINITIONS WHAT IS A PEG FEEDING TUBE? PEG stands for Percutaneous Endoscopic Gastrostomy. PEG feeding tubes are placed by using an endoscope and making a surgical incision to place the tube into the stomach. PEG tubes are placed so that patients may receive artificial nutrition and hydration directly into their stomach.
 is a medical")
WHAT IS ARTIFICIAL NUTRITION AND HYDRATION? Artificial nutrition and hydration (ANH) is a medical treatment that is often given to individuals who can no longer eat or drink by mouth.

REASONS FOR PEG TUBE PLACEMENT: There are many medical conditions that cause a temporary inability to maintain nutrition or hydration from oral (mouth) intake. PEG tube placement supports patient’s healing and recovery by providing needed nutrition and hydration. PEG tube placement prevents patients who can no longer eat or drink by mouth from dying due to dehydration. Many people believe nutrition and hydration is ordinary and basic care and should be provided to all patients.

REASONS NOT TO PLACE A PEG TUBE: In patients with terminal conditions such as cancer or severe dementia, PEG tube placement does not support a return to health, but prolongs the end of life process. Patients who do not receive ANH via a PEG tube do not suffer. When a patient stops eating and drinking, death comes from dehydration, not starvation. Dehydration occurs fairly swiftly and painlessly in most patients. ANH is not standardized care, it is an individual choice. In patients with terminal conditions, loss of a desire to eat or drink is part of the natural dying process. PEG tubes can be burdensome to the patient and are not risk free.

RELATED TO PLACEMENT OF PEG FEEDING TUBES .

WHAT ETHICAL CONSIDERATIONS SURROUND PLACING A PEG TUBE FOR ARTIFICIAL NUTRITION AND HYDRATION? Autonomy Beneficence Non-Maleficence Justice

AUTONOMY Autonomy describes an individual’s right to make their own decisions without interference or control of others. Caregivers and families must respect a patient’s decision for or against the placement of a PEG tube for ANH. Family or surrogate decision makers who may find themselves deciding for or against PEG tube placement must remember and commit to a decision the patient would want for themselves. When making a decision, families or surrogates must remove their self interest.

BENEFICENCE Beneficence is taking action for the benefit of others. Beneficent acts are taken to prevent harm or improve the circumstances of another person. When healthcare providers offer the treatment option of PEG tube placement, they must consider factors such as the patient’s condition and prognosis. Will PEG tube placement and ANH prevent harm to the patient or will it improve their condition?

Non-Maleficence means to do no harm Healthcare providers must refrain from offering medical treatments that bring more risk of harm than benefit. A physician who recommends and places a PEG tube for a patient who is clearly at the end of life may not be acting in a nonmaleficent manner.

JUSTICE The ethical term of justice describes the distribution of benefit, risk and cost equally among all patients A physician who only recommends PEG tube placement as an option to terminally ill patients who have insurance would not be following this principle.

COMPLICATIONS WITH PEG TUBES PLACEMENT

COMPLICATIONS WITH PEG TUBES PLACEMENT Aspiration: Aspiration of stomach content into the lungs can occur during insertion of the PEG tube because the esophageal sphincter that stops gastric contents from refluxing into the esophagus is held open by the endoscope (Malhi & Thompson, 2014). Blockage: PEG blockages occur by inadequate flushing of the tubes after feeding or medication administration. Site infection: This is the most common complication, which may be due to poor hygiene when handling the tube. This can cause inflammation around the tube which can cause purulent drainage and pain.

COMPLICATIONS CONT. Leakage: leaking of food contents or stomach content around the PEG tube due to improper positioning. Granuloma formation: A granuloma is a nodule of granulation tissue at the PEG insertion site and is an immune response by the body to a foreign body that it is unable to eliminate. This can produce exudate which can make the skin sore Buried bumper syndrome: Buried bumper syndrome is caused by the external fixation plate being placed too tightly against the patient's skin, which causes the internal bumper to erode into the lining of the stomach.

ALTERNATIVE TO PEG TUBE Careful Hand Feeding: Patients had dysphagia before feeding tubes were invented. Slow and very careful hand feeding is a proven alternative to peg tubes. Social Effect: Careful hand feeding provides patients with the enjoyment of eating and a therapeutic socialization with caregivers.

RECOMMENDATIONS DECISION-MAKING PROCESS: The decision to receive a PEG tube is a personal choice. The federal Patient Self-Determination Act of 1990 requires healthcare providers to inform the patient of their rights to make decisions about their medical care and for providers to respect those wishes (Congress. gov).

RECOMMENDATIONS COLLABORATION: Healthcare providers needs to work with patients and families to provide the best outcome for the patient. This is a partnership relationship. Providers are to discuss nutritional issues, skin or emotional concerns, cultural and religious aspects. We will provide you with the information to make informed choices to respect the rights and dignity of the patient at the end of life (Sorrell, 2010). Ethics will guide us in our decision making process. We will work with you in assuring your wishes are confirmed in a written document. COMMUNICATION/ADVANCED DIRECTIVES: The patient may convey their wishes through an advanced directive. An advanced directive can be an oral statement to family or friends, an oral statement to a physician, or in a written advance directive (Lo, p. 91). As healthcare providers, our responsibility is to honor those directives.

RECOMMENDATIONS COMMUNICATION/ADVANCED DIRECTIVES : We provide information on advanced directives to all patients on admission. An advanced directive can specify whether a procedure or treatment be provided or withheld such as hydration or nutrition, it also allows the patient to appoint an agent to make their decisions if they are incapacitated (Virginia. gov). If you are this person, they have entrusted you to carry out their wishes as stated. We will honor the patient’s advanced directive. MAINTAINING QUALITY OF LIFE: Nutrition is always a primary concern in healthcare. We as caregivers know that with aging, a gradual disinterest in food is normal. It is a natural part of the aging process (Dibartolo, 2006). Will placing a feeding tube contribute to the quality of life?
. Pause before a PEG: A")
REFERENCES Aparanji, K. P. & Dharmarajan, T. S. (2010). Pause before a PEG: A feeding tube may not be necessary in every candidate. Journal of the American Medical Directors Association, 11(6), 453 -456. doi: 10. 1016/j. jamda. 2009. 11. 016 Brody, H. , Hermer, L. D. , Scott, L. D. , Grumbles, L. L. , Kutac, J. E. , & Mc. Cammon, S. D. (2011). Artificial nutrition and hydration: The evolution of ethics, evidence and policy. Journal of General Internal Medicine, 26(9), 1053 -8. doi: 10. 1007/s 11606 -011 -1659 -z Di. Bartolo, M. C. (2006). Careful hand feeding: A reasonable alternative to PEG tube placement in individuals with dementia. Journal of Gerontological Nursing, 32(5), 2533; quiz 34 -5. Retrieved from http: //search. proquest. com. mutex. gmu. edu/docview/204201343? accounti d=14541 Ganzini, L. (2006) Artificial nutrition and hydration at the end of evidence. Palliative and Supportive Care, 4, 135 -143. life: Ethics and Hoefler, J. M. (2000). Making decisions about tube feeding for severely demented patients at the end of life: Clinical, legal and ethical considerations. Death Studies, 24, 233 -254 Lawrence, D. J. (2007). The four principles of biomedical ethics: A foundation for current bioethical debate. Journal of Chiropractic Humanities. Retrieved from http: //archive. journalchirohumanities. com/Vol%2014/ JChiropr. Humanit 2007 v 14_34 -40. pdf Lo, B. (2013). Resolving ethical dilemmas (5 th ed. ). Philadelphia: Lippincott Williams & Wilkins
. PEG tubes: Dealing with complications.")
REFERENCES. Malhi, H. , & Thompson, R. (2014, Nov). PEG tubes: Dealing with complications. Nursing Times, 110, 18 -21. Retrieved from http: //search. proquest. com. mutex. gmu. edu/docview/1625411894? a ccountid=14541 Percutaneous Endoscopic Gastrostomy (PEG) | ACG Patients. (n. d. ). Retrieved from http: //patients. gi. org/topics/percutaneousendoscopic-gastrostomy-peg/ Sorrell, J. M. (2010). Use of feeding tubes in patients with advanced dementia. (2010). Journal of Psychosocial Nursing & Mental Health Services, 48(5), 15 -18. doi: http: //dx. doi. org. mutex. gmu. edu/10. 3928/02793695 -2010033102
- Slides: 23