Pediatric Surgical Emergencies Dr Abdelbaset Ali Ahmed Assistant

Pediatric Surgical Emergencies Dr: Abdelbaset Ali Ahmed Assistant lecturer of Pediatric Surgery Sohag university 2017

Introduction n Neonatal intestinal bstruction u Atresias u Hirschsprung’s u Malrotation u Volvulus u Intussusception n n NEC The Acute Groin Bleeding Meckel’s Foreign Bodies

Bowel Obstruction n Diagnosis often age specific Bilious vomiting in the infant and child is a surgical emergency until proven otherwise n Abdominal distention. n constipation n Colicy abdominal pain. n

Bowel Obstruction
 n Hydrate")
Bowel Obstruction: Initial Management NG or OG to low wall suction (NPO!!) n Hydrate and replace losses u 10 cc/kg of crystalloid IS NOT AN ADEQUATE BOLUS!! n Antibiotics if suspect perforation or necrosis n Transfer to appropriate facility n

Intestinal Atresia Usually presents the first few days of life n Child may feed well for a day or two with distal atresia n Duodenal atresia often diagnosed on antenatal U/S n Atresias can occur anywhere in GI tract from pharynx to anus n

Atresias Esophageal: aspirate feeds immediately, OG tube won’t pass n Duodenal: bilious vomiting immediately, “double bubble” n Jejunal: usually present 1 st 24 hours, large dilated proximal loop or loops n

Atresias Ileal: may take 24 -48 hours before bilious emesis n Colonic: rare, may present with bilious emesis after 2 -3 days n Anal: should be diagnosed at birth, often a perineal fistula is labeled normal n

Atresias may be multiple

Jejunal Atresia

Imperforate Anus: Anal atresia

Hirschsprung’s Disease Congenital colonic aganglionosis u Physiologic obstruction n May present first few days to weeks of life n Short segment disease often tolerated for months n Starts at anus and extends proximally a variable distance n

Hirschsprung’s Disease

Hirschsprung’s Disease

Toxic Megacolon Severe enterocolitis n Usually only seen with Hirschsprung’s Disease or Ulcerative Colitis n NG decompression, IV fluids, IV antibiotics n Mortality 20 -30% in some studies n

Toxic Megacolon

Hirschsprung’s in an 8 year old

Believe it or Not. . .

Malrotation Normal

Malrotation Most often presents during the first few months of life n Infant with acute onset of bilious emesis n May be diagnosed on UGI for other reasons n Malrotation is a surgical urgency due to the possibility of volvulus n VOLVULUS IS A SURGICAL EMERGENCY n

Malrotation

Malrotation

Volvulus

Volvulus n Malrotation most common condition resulting in midgut volvulus n Can have volvulus with normal rotation

Small Bowel Obstruction

Meckel’s

Intussusception Inversion of the bowel upon itself secondary to a lead point n Juvenile intussusception most often idiopathic u Also secondary to Meckel’s n Presents 6 months to 2 years of age u As early as 1 month n

Intussusception n Acute painful episodes followed by periods of lethargy n May or may not have “currant-jelly” stool u But often stool is heme positive

Intussusception

Intussusception

Intussusception Treatment is: n hydrostatic reduction or n Operative exploration for reduction and appendectomy is needed n Recurrence after surgery rare but possible n Post-op intussusception can occur after any surgery

Necrotizing Enterocolitis Incidence: 25, 000 per year; 10 -70% mortality n Most common serious GI disease of low birthweight infants n Etiology is unknown n Most common in terminal ileum and colon u “pan-necrosis” involves >75% of gut and occurs in 19% of patients; mortality approaches 100% n

Necrotizing Enterocolitis Abdominal distention is most common finding n Feeding intolerance with bilious NG aspirate n Palpable bowel loops and crepitus n Edema and erythema of abdominal wall ® peritonitis n Rectal bleeding is common: gross and/or occult n

NEC Abdominal Films

Necrotizing Enterocolitis Initial medical management unless evidence of necrosis/perforation n OG decompression n Broad spectrum antibiotics n NPO, TPN, fluid resuscitation n Abdominal film surveillance n Serial labs: CBC with platelets, ABG, CRP n

NEC Abdomen

NEC Pneumoperitoneum

NEC Ileal Involvement

NEC Totalis

The Acute Groin

Testicular Torsion Most important, not most common cause n Peak incidence 13 to 16 years of age n Before age 16 u 60% torsion testis appendix, 30% testicular torsion, 10% epididymitis n Sudden testicular pain, nausea, palpation exquisitely tender, horizontal lie, hemiscrotum red, edematous n

Testicular Torsion

Testicular Torsion Loss of cremasteric reflex with torsion n Torsion of appendix testis similar: point tender at upper pole, testicle less tender n Ultrasound and/or nuclear blood flow study MAY be of benefit. n Do not delay surgical exploration for studies n

Testicular Torsion

Inguinal Hernia From Atlas of Pediatric Surgery, Ashcraft, 1994

Incarcerated Inguinal Hernia

Hernia Reduction From Surgery of Infants and Children, Oldham, et. al. , 1997
 n If able to")
Incarcerated Hernia If unable to reduce: urgent operative exploration (NPO) n If able to reduce without sedation: urgent surgical referral with repair soon n If extremely difficult (sedation, surgical referral): repair next day n Watch child for obstructive symptoms n
 n Bleeding most")
Meckel’s In newborns and infants present as bowel obstruction (volvulus, intussusception) n Bleeding most common presentation in children n Painless, massive, requiring transfusion n Bleeding due to peptic ulceration at the base of diverticulum n

Meckel’s

Foreign Bodies Laryngeal: Hoarseness, aphonia, dyspnea, cyanosis n Tracheal: asthmoid wheeze, subglottic “thud” n Bronchial: period of coughing and wheezing, then asymptomatic interval n

Bronchial Foreign Body n Check valve obstruction u partial obstruction inspiration, complete obstruction expiration u obstructed lung expanded during expiration
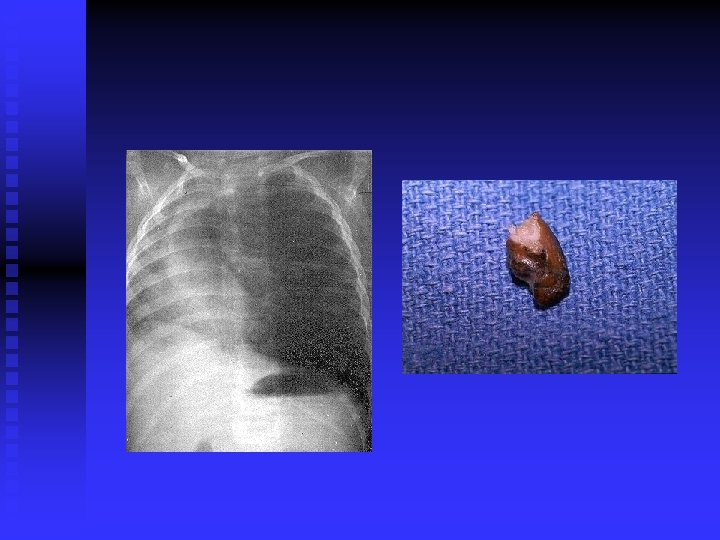
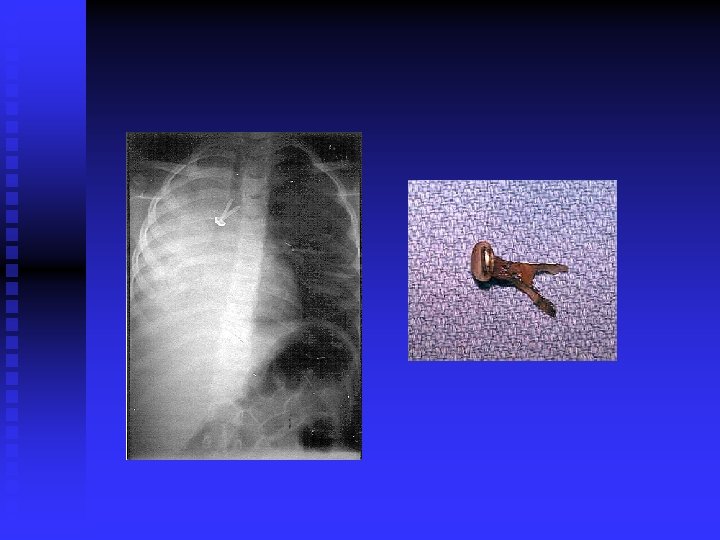

Treatment n Removal under direct vision as soon as possible by a “skilled” bronchoscopist u removal with grasper or balloon catheter n Laryngeal FB may require emergent cricothyrotomy

Complications Loss of airway u partial obstruction object may become complete with paralysis n Pneumothorax u vigorous positive pressure ventilation n Post-obstructive pneumonia n

Esophageal Foreign Bodies Coins most common n Four cardinal areas or narrowing u below the cricopharyngeus muscle u level of the aortic arch u carina u just above the diaphragm n

Signs and Symptoms Episode of coughing, choking and drooling n Pain and dysphagia n After an asymptomatic period get signs of obstruction n Pain, fever, and shock occur with perforation n

Diagnosis History suggests n CXR/Neck films show radiopaque coins and foreign bodies n May need contrast study to diagnoses radiolucent objects n

Esophageal Coin

Treatment Removal of foreign body under direct vision with rigid esophagoscope n If object has passed into stomach, observation warranted n Post removal CXR n

Complications Aspiration pneumonia n Esophageal stricture n Esophageal perforation u secondary to erosion u iatrogenic n Small bowel obstruction n

Batteries If in esophagus, treat with removal n Most recommend removal endoscopically if in stomach n Difficulty arises if already in small bowel u would require laparotomy to remove u reports of ulceration/perforation as well as successful passage n

Question 2? Why are Pediatric Surgeons so interested in flatus? Contrary to popular belief, kids (and adults) with obstruction can still have bowel movements, but they won’t pass gas!

Summary n Bowel Obstruction u Atresias u Hirschsprung’s u Malrotation u Volvulus u Intussusception n n NEC The Acute Groin Bleeding Meckel’s Foreign Bodies

- Slides: 66