PEDIATRIC SURGERY2018 No 5 Attendance Obligatory Type of

PEDIATRIC SURGERY-2018 No. : 5 Attendance: Obligatory Type of lecture: theory Place : Hall no. 4 college of medicine –Mustansiriyah University. Date : Wednesday 5 th of March 2018. Time : 12: 00 – 1: 00 AM. Students: 4 th year / college of medicine / Mustansiriyah University By : Dr. Ali E. Joda M. B. Ch. B. - F. I. C. M. S. - pediatric surgeon. E. mail : ali. egab. joda@uomustansiriyah. edu. iq

Objectives: What is Hirschsprung's disease, its pathophysiology, clinical features & way of diagnosis? What are the congenital anorectal malformations, the spectrum of the disease, classification of the types & the options of surgical treatment? By the end of this lecture, you have to be able to: Summarize the main outlines of resuscitation in cases of acute presentation of these conditions. Verifying the staged surgical approach of these conditions.
 Is a functional intestinal obstruction due to congenital")
Hirschsprung's disease (Congenital megacolon, colonic aganglionosis) Is a functional intestinal obstruction due to congenital absence of ganglion cells in the recto-sigmoid region & extend proximally for varying length result in failure of propagation of peristalsis & absence of relaxation of internal anal sphincter. so there will be dilated proximal colon (mega) , narrow distal colon , the aganglionosis may be in a short segment , long segment or even total colon.

Incidence 1 in 5000 newborn. 70 -80 % in males. 25% with family history of the same disease & having other associated anomalies.

Etiology & genetics : The ganglion cells are derived from neural crest of embryo, which undergo migration through GIT from proximal to distal after differentiation into mature ganglion cells. In infant with Hirschsprung's disease (HD, ) this process is disturbed & the ganglion cells are absent in distal bowel. The genesis of Hirschsprung's disease is multifactorial (genetic + environmental). The most common identified gene is RET proto-oncogen. Other genes involved may be GDNF (glial cell line derived neurotrophic factor), END 3, ENDB (endotheline) , S 10 X 10 gene , S 1 P 1 gene.
 Neonatal intestinal obstruction: (failure or delayed passage of meconium, abdominal")
Diagnosis: Clinical presentation: 1) Neonatal intestinal obstruction: (failure or delayed passage of meconium, abdominal distension, & vomiting). 2) Chronic constipation: some patients present in later childhood with chronic constipation especially those with short segment HD, they usually had history of delayed passage of meconium for more than 48 hr. , failure to thrive, malnutrition, hypoproteinemia, anemia, gross abdominal distension, dependence on laxatives & enemas, but without encopresis or soiling. 3) Enterocolitis : 10% of children with HD present with fever , abdominal distension , offensive diarrhea due to Hirschsprung's disease associated enterocolitis (HAEC). stasis of fecal materials in the colon lead to bacterial overgrowth & invasion of Clostridium difficilli & Rota virus to the bowel wall causing secondary infection ( enterocolitis )which may cause life threatening toxic megacolon.
 Neurocristopathy syndromes: 1. Waardenberg –shah syndrome.")
Associated anomalies : Down syndrome (trisomy 21 ) Neurocristopathy syndromes: 1. Waardenberg –shah syndrome. 2. Goldberg – shprintzen syndrome. 3. Yemenite deaf blind hypopigmentation syndrome. 4. Piebaldism. 5. SLOS Smith-Lemli Optiz syndrome. 6. MEN 2 (multiple endocrine neoplasia). 7. Haddad syndrome (ondine curse). Rectal examination : Hypertonic anal sphincter (long gripping of index finger). Empty rectum. Or explosive discharge of fluid stool & gases suggestive of enterocolitis.
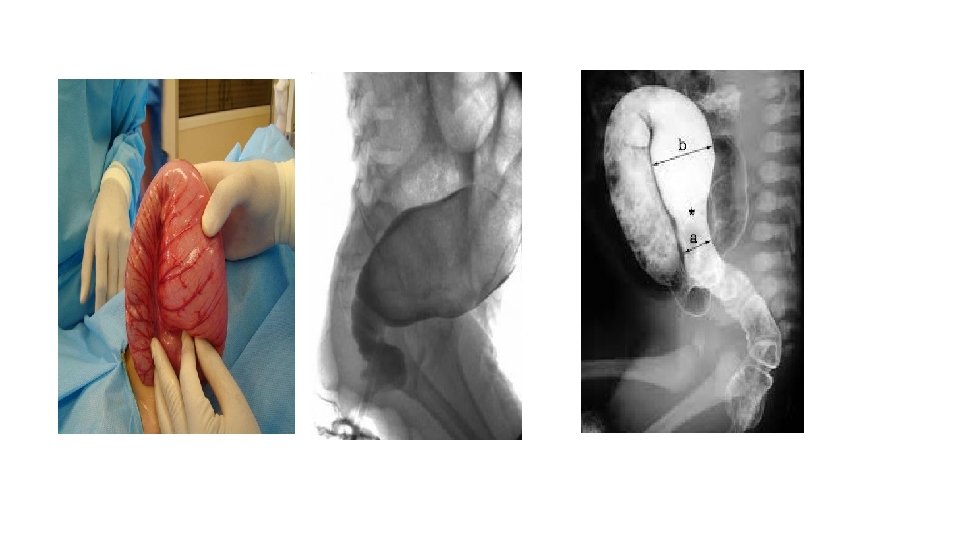
 Barium enema : (Narrow segment distally, transitional zone, dilated segment proximally).")
Investigation : 1) Barium enema : (Narrow segment distally, transitional zone, dilated segment proximally). Recto-sigmoid ratio less than 1 (transvers diameter of rectum / transverse diameter of sigmoid) (a/b = < 1). Retention of contrast material in the colon more than 24 hr post filming. Neonate with HD may have false negative result of contrast enema.
 Anorectal manometry: recto-anal inhibitory reflex is defined as reflex relaxation of internal anal")
2) Anorectal manometry: recto-anal inhibitory reflex is defined as reflex relaxation of internal anal sphincter in response to rectal distension. This is normally present in normal children & absent in HD. But it is not reliable in neonate because of immaturity of the reflex & artifact created by movement & crying of the baby. 3) Rectal biopsy: give the definitive diagnosis of HD by histological confirmation of (absence of ganglions, hypertrophy of nerve fibers, increase staining of acetyl choline esterase) in both submucosal plexus of Meisner & meyenteric plexus of Aurbach. It can be done either by suction rectal biopsy (mucosa & submucosa) or by full thickness rectal biopsy.

Pre- operative management : Resuscitation for neonate with intestinal obstruction or children with enterocolitis by I. V. F (intravenous fluid), electrolytes , broad spectrum antibiotics , nasogastric tube decompression , digital rectal stimulation or colonic irrigation with normal saline enema. Emergency stoma is indicated if the above measures failed.
: • Stoma formation: as an")
Surgical treatment for Hirschsprung's disease: • three stages (Usually): • Stoma formation: as an emergency procedure or electively performed to protect future colonic anastomosis. • Pull-through procedure: resection of aganglionic segment & bringing the normally innervated bowel down to be anastomosed with the low rectum or anus. The Pull-through procedures may be : -

Pull-through procedure: resection of aganglionic segment & bringing the normally innervated bowel down to be anastomosed with the low rectum or anus. The Pullthrough procedures may be : q Swenson pull-through. q Soave ( endorectal pull-through ). q Duhamel (retrorectal pull-through). q Rehbein pull-through. q Trans-anal pull-through. q Laparoscopic pull-through. • Closure of stoma. • Two stages (standard): colostomy + pull-through In 1 st stage then closure of stoma in 2 nd stage. • One stage (for selected cases).
- Slides: 13